
Abstract
Background
The diagnosis of acute diverticulitis is mainly based on clinical, biological and computed tomography (CT)-scan findings. Elective colonoscopy is recommended after medical treatment, to rule out another diagnosis and to detect associated conditions; however, the relevance of this recommendation has been questioned.
Patients and methods
Between January 2005 and December 2011, we retrospectively identified in three referral centers the consecutive patients whom underwent a colonoscopy after the medical treatment of a CT scan-proven acute diverticulitis episode. We excluded from the analysis patients with haematochezia or recent change in bowel habits. Sex and age-matched asymptomatic patients undergoing a screening colonoscopy were chosen as a control group. We collected and compared the results of colonoscopy and histological findings in both groups.
Results
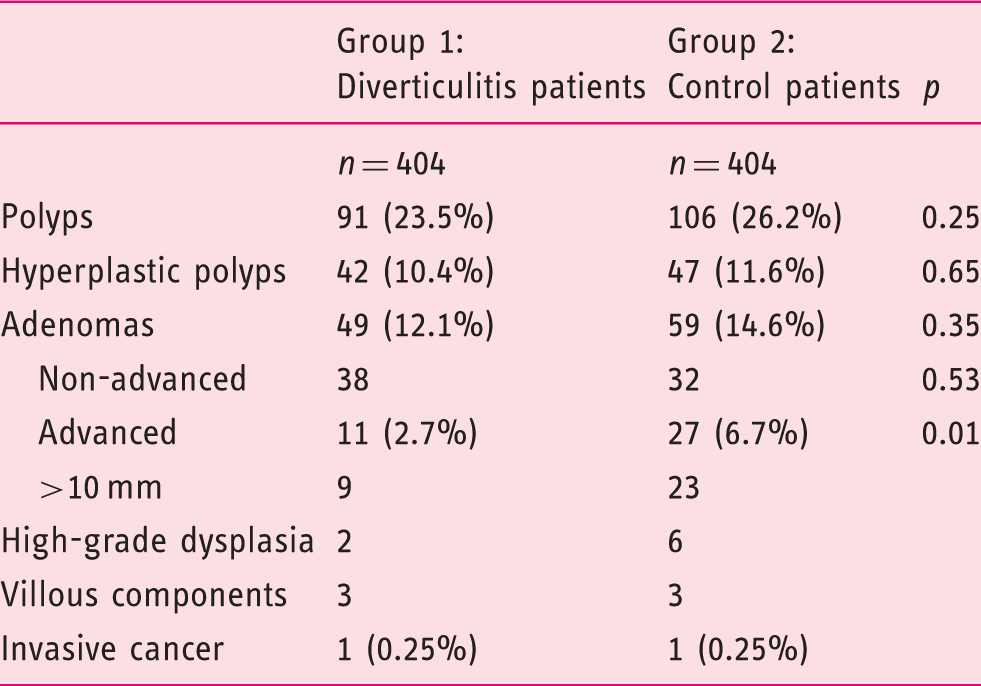
We matched 404 patients whom underwent a colonoscopy after an episode of acute diverticulitis with 404 control patients. Their mean age was 60.9 years, with 59% being women. Colorectal adenoma, advanced adenoma and cancer detection rates in acute diverticulitis patients were 12.1%, 2.7% and 0.25%, respectively; versus 14.6% (p = 0.35), 6.7% (p = 0.01) and 0.25% respectively, in control patients.
Conclusions
Diagnosis rates for adenomas and for colorectal cancer during a colonoscopy scheduled after acute diverticulitis were similar than those of control patients undergoing a screening colonoscopy, while the detection rate of advanced adenomas was lower. We suggest that colonoscopy should be indicated only in selected patients, i.e. those presenting with reasonable doubt on initial CT-scan, those with alarm symptoms, and those with identified risk factors for colorectal cancer.
Introduction
Diverticular disease is a common condition in Western countries. It is estimated that 10–25% of patients with diverticulosis develop an acute diverticulitis in their life time. 1 To date, it is recommended to perform a colonoscopy in patients after a first acute uncomplicated diverticulitis treated successfully by medical management and prior to a potential colonic resection of the diverticular area, in order to exclude other diagnoses, mainly a colonic cancer. 2 This recommendation was based on the low sensitivity of former radiological techniques, such as barium enema, to analyze the colonic lumen and to differentiate a pure diverticular disease from a diverticular disease associated with a colonic carcinoma.3,4
Nowadays, the diagnosis of acute diverticulitis when suspected by the clinical setting is confirmed by computed tomography (CT) scan, a technique able to show the colonic diverticular disease with localized colonic wall thickening and to analyze the pericolonic fat. Sensitivity and specificity of a CT scan for the diagnosis of acute diverticulitis are close to 100% and 95%, respectively. 5 The CT scan also permits to distinguish uncomplicated diverticulitis from cases with complications, such as a perforation or a peri-colonic abscess 1 ; however, CT scan is not the gold standard to detect abnormalities possibly associated with acute diverticulitis.
Thus, routine post-diverticulitis colonoscopy is indicated, to preclude a colorectal cancer; however, a recent retrospective uncontrolled series suggests that the frequency of advanced colonic neoplasia in patients undergoing a routine colonoscopy after an episode of acute diverticulitis could be equivalent or even lower than that of screening colonoscopy in asymptomatic, average-to-high-risk individuals. 6 According to this latter result, one could wonder whether routine colonoscopy after acute diverticulitis is still systematically mandatory. On the other hand, another retrospective study carried out in patients with a left-sided diverticulitis reports a 26% risk of adenomas and a 2.8% risk of colorectal cancer. Associated colonic lesions were particularly observed in patients presenting with complicated diverticulitis (abscesses or perforation). 7 Regarding these results, the authors indicate colonoscopy after diverticulitis, in patients without recent colonic luminal evaluation.
Considering these contradictory studies, we performed a large controlled study, to compare the detection rate of adenomas and neoplastic lesions results between patients whom were explored after an episode of acute diverticulitis, and age- and sex-matched patients undergoing colonoscopy due to a familial history of colorectal cancer or adenomas.
Patients and methods
Patients
We retrospectively included all patients whom were hospitalized for an acute diverticulitis in three French referral centers (i.e. Lariboisière Paris 10 University Hospital, Montfermeil General Hospital and Rouen University Hospital), between January 2005 and December 2011, and whom underwent a colonoscopy within the 6 months following the acute episode. The search was performed by crossing the codes for ‘diverticulitis’ and ‘colonoscopy’. Acute diverticulitis was defined by a typical clinical setting associated with a CT scan confirmation of the disease, with the presence of colonic diverticula, a localized colonic wall thickening and the stranding of pericolonic fat. 1 In these three centers, colonoscopy was routinely performed as recommended by the American Society of Colon and Rectal Surgeons, 2 during the weeks following diverticulitis in all patients, in order to rule out an associated and/or misdiagnosed colorectal cancer and to confirm the diverticular disease. We excluded from the analysis all patients with haematochezia, recent change in bowel habits or a personal history of colorectal neoplasia. We also excluded patients whom had undergone a colonoscopy within the 2 years before the episode of acute diverticulitis.
Patients from the diverticulitis group were sex- and age-matched with patients from a control population of the Rouen University Hospital with:
A familial history of colorectal adenoma or neoplasia; No digestive complain or symptom; and A screening colonoscopy in the same three hospitals during the same 7-year period.
In this control group, we excluded: Patients with alarm symptoms, such as hematochezia, abdominal pain or recent change in bowel habits; patients with a history of inflammatory bowel disease or carrier of a genetic mutation, such as Lynch syndrome or familial adenomatous polyposis (FAP); patients with a personal history of colorectal neoplasia; and patients with a familial history of colorectal neoplasia that occurred before 50 years of age.
Demographic data, including age and gender, were obtained for all patients. For patients with recurrent onset of diverticulitis, only the first episode was taken into account.
Endoscopy and histology
Large bowel cleansing for colonoscopy was based on the same practices in the three study centers, with a low-fiber diet during the 3 days prior to the procedure; and then the ingestion of 4 liters of polyethylene glycol (PEG) solution the night before the examination. All procedures were performed under general anesthesia. We recorded the presence of adenomatous and/or hyperplastic polyps or a colonic cancer. In the case of polyp removal, the histological findings were categorized on the basis of the most advanced lesion identified. Lesions considered as adenomas included adenomas of any size, any type and any grade of dysplasia (including adenocarcinoma and serrated adenoma). Advanced adenoma was defined either as an adenoma with a diameter of at least 10 mm, or with high-grade dysplasia, a villous component larger than 25%, or an invasive cancer.
Statistical analysis
Descriptive statistics were used in both groups to indicate the patient's demographic features, endoscopic findings and histological analyses. Categorical variables were presented as percentages and numerical variables as means and ranges. Results were expressed as percentages or means ± standard deviation (SD), for continuous variables. Chi-square test, Fisher's exact test and Mann-Whitney test were used to compare non-continuous and continuous data between the two patient groups.
Results
During the study period, 467 patients had a colonoscopy during the 3 months following an acute diverticulitis episode. We excluded 39 patients for whom the diagnosis of acute diverticulitis was purely based on clinical data or on non-contrast enhanced CT scan from the analysis. We also excluded 22 patients presenting with hematochezia at admission and 2 patients with a personal history of colorectal cancer. Finally, we included 404 patients with an acute episode of diverticulitis in the study group (Group 1). Among them, contrast-enhanced CT scans showed a complicated diverticulitis in 41 patients (10%). Complications were: an abscess in 34 cases and a perforation in the remaining 7 cases. In one case, the radiologist suggested a sigmoid cancer, which was confirmed at colonoscopy.
The control group (Group 2) was obtained by selecting 404 age- and sex-matched patients whom underwent a screening colonoscopy, as detailed in the Methods section. The mean age was similar in both groups: 60.9 +/– 12.6 years in the study group versus 60.7 +/– 13.4 years in the control group. In both groups, 88 patients were younger than 50 years. There were 238 women (59%) and 166 men in each group.
Endoscopy
We performed colonoscopy after a mean delay of 62 days after admission for acute diverticulitis. Colonoscopy was complete in 391 patients from Group 1 and 396 patients from Group 2 (97% versus 98%: not statistically significant (ns)). In Group 1, incomplete colonoscopy was related to a significant diverticular stenosis (11 cases), technical difficulties (2 cases) and an obstructing cancer (1 case). In Group 2, colonoscopy was not complete in 7 patients because of technical difficulties and in 1patient, because of an obstructing cancer. In all cases, incomplete colonoscopies were followed by a CT colonography that did not detect any additional lesions. Two perforations occurred in patients from Group 1, versus none in patients from the control Group 2 (ns). The two colonic perforations were located to the sigmoid colon: The first occurred after a polypectomy in a diverticular area; the second one occurred in a diverticular area without polypectomy.
In Group 1, we detected 94 colorectal polyps in 91 patients (23.5%); while 111 polyps were detected among 106 patients (26.2%) in Group 2 (p = 0.25). In patients younger than 50 years of age, we found 8 adenomas in patients from Group 1 versus 17 adenomas in patients from Group 2 (9% versus 19%; p = 0.03). No adenoma larger than 10 mm was detected in Group 1, while 3 polyps were endoscopically-advanced adenomas in Group 2 (p = 0.24).
One colonic cancer was found in each group, in one 72- and one 69-year old patient in Group 1 and Group 2, respectively. In Group 1, the colonic cancer was located in the sigmoid colon, while cancer was found in the ascending colon in the Group 2 patient.
Histology
Colonoscopic findings per patient, according to the most advanced lesion
Colonoscopic findings in patients with diverticulitis, per study center
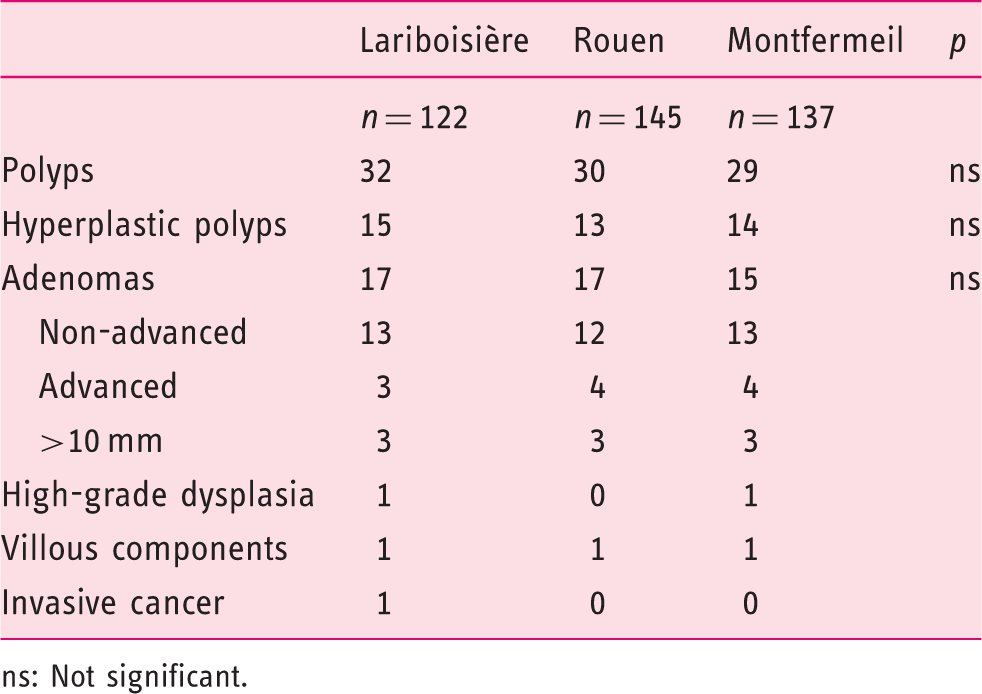
ns: Not significant.
Discussion
In this large controlled study, we found that patients whom were explored after a first episode of acute diverticulitis had a similar or even a reduced risk of advanced colorectal neoplasia, by comparison with a population of asymptomatic patients at an average risk of colorectal cancer. This result suggested that after a first episode of acute diverticulitis documented by CT-scan, routine colonoscopy should not be systematically indicated, but recommended only in selected patients with associated symptoms or recognized risk factors for colorectal cancer. Indeed, with the rising clinical burden of diverticular disease, the current strategy of routine colonic evaluation following any initial episode of acute diverticulitis may become, in the future, a significant factor limiting the provision of colonoscopy to other patients at higher risk of colorectal cancer. Moreover, even if it is low, any colonoscopy carries a risk of procedure-related complication to which it is not justified to expose the patient, when the indication for the endoscopic procedure is not clearly demonstrated.
The current recommendation of routine colonoscopy after a first episode of acute diverticulitis is based on the poor visualization of the large bowel by former radiological techniques such as barium enema, which are unable to differentiate between diverticular disease and carcinoma.3,4 Colonoscopy is proposed to rule out differential diagnosis and to detect associated conditions, such as advanced adenomas or cancer. To date, the diagnosis of acute diverticulitis relies on CT scan, with a sensitivity close to 100% and a specificity of 95%. 5 Moreover, CT scan is able to provide further information regarding the intra-luminal abnormalities that may be associated with the diverticular disease. However, routine contrast-enhanced CT scan without colonography is not the first-line investigation for detecting unsuspected colorectal cancer, as it has been demonstrated that it has a sensitivity of 72.4% for colorectal cancer detection. 8 Thus, patients with a CT-proven diverticulitis could be considered to have undergone a moderately sensitive test for colorectal cancer. Moreover, it has been suggested that the presence of an abscess or local perforation or fistula on a CT scan could be associated with increased odds of diagnosis of colorectal cancer in control colonoscopy. 7 We did not observe this correlation in our series; however, we only found one colorectal cancer at colonoscopy, within the 404 patients from the diverticulitis group.
Patients with associated symptoms, such as hematochezia, change in bowel habits, or chronic abdominal pain may be at a higher risk of having other lesions; and thus, need colonoscopy after acute diverticulitis. For this reason, we excluded these patients from our study. The question of the elderly should also be assessed. In our study, we found significantly more colorectal adenomas in patients aged <50 years in the control group, as compared to young patients with acute diverticulitis. These results suggested that routine colonoscopy in patients <50 years old after a first acute diverticulitis episode is less effective than in an age and sex-matched average-risk population undergoing a screening colonoscopy.
There are conflicting data in the medical literature concerning the association between diverticular disease and colorectal carcinoma. Some authors assume that a causal association exists between sigmoid diverticulitis and long-term increased risk of left-sided colon cancer, 9 while others show that patients with diverticulitis present a decreased rate of advanced colonic neoplastic lesions. 10 Moreover, Meurs-Szojda et al. demonstrate, in a large retrospective study of 4241 patients referred for colonoscopy, that there is no correlation between patients with diverticulosis and a higher incidence of polyps or colorectal cancer. 11 Sharma et al., in a recent meta-analysis, suggest that routine colonoscopy may not be necessary in the absence of other indications. 12 In our controlled study, we also observed that patients with acute diverticulitis presented significantly less advanced neoplasia than patients referred for a screening colonoscopy, as well as exhibiting a trend for presenting with fewer adenomas.
A drawback of our study is its retrospective design; however, we included in our three centers all the patients hospitalized for a CT-scan-proven diverticulitis whom underwent, in their 3-month follow-up, a colonoscopy at the same center. To date, it is the policy of our centers to routinely perform a colonoscopy on all patients after a first episode of acute diverticulitis. We excluded from our analysis the patients with a purely clinical diagnosis of diverticulitis. Indeed, it is our opinion that the lower diagnostic uncertainty in these patients required a further colonoscopy, to confirm the diverticular disease and to rule out other diagnoses, as suggested by Westwood et al. 6
In order to reinforce our results, we compared the rate of colorectal adenoma and colorectal neoplasia found in patients with a first episode of acute diverticulitis to that of a control population. The latter was constituted of asymptomatic patients undergoing a screening colonoscopy for a familial history of colorectal neoplasia that had occurred after 50 years of age, after exclusion of patients with a history of inflammatory bowel disease or genetic colorectal cancer predisposition (Lynch syndrome or FAP). Our choice of these control patients, whom were age and sex-matched with those presenting with a diverticular disease, was based on the fact that this control group, without symptoms and without personal history of colorectal adenoma or neoplasia, carried a low rate of presenting a colorectal adenoma or neoplasia, as described in previous series. Indeed, it has been proven that colonoscopy performed in asymptomatic individuals present with a detection rate of colorectal adenoma of approximately 15%, of an advanced colorectal adenoma varying between 5–6%, and a detection rate of colorectal cancer close to 1%.13–15 In our study, the detection rate at colonoscopy of colorectal adenoma, advanced adenoma and cancer in the control group was 14.6%, 6.7% and 0.25%, respectively, which is very close to previously-observed results and probably reflects the relevance of the chosen control group.
Colonoscopy in patients with diverticular disease may be technically difficult, because of luminal narrowing, spasm, muscular hypertrophy and fixation. 16 In particular, there is a potential risk of turning a sealed perforation into a free one, while performing colonoscopy. Diverticular disease is also associated with a higher rate of incomplete colonoscopy, as compared with the general population. 17 In our series, we observed two perforations in 404 patients (0.5%), which was higher than the perforation rate of 0.01% currently observed in the medical literature. 14 The rate of perforation and complete colonoscopy was not significantly different between patients with diverticular disease and control patients, but the statistical power of our study was not high enough to properly answer this question.
In conclusion, in this large multicenter controlled study, the yield of advanced neoplasia in patients with CT-diagnosed acute diverticulitis was low enough to suggest that colonoscopy after a first episode of acute diverticulitis could be reserved for patients with additional symptoms, such as hematochezia or change in bowel habit, and for patients with a personal history of colorectal neoplasia. Large-scale prospective studies are warranted to confirm these preliminary results, before revising the current recommendations.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there are no conflicts of interest.