
Abstract
Objectives:
The high mortality and morbidity rates associated with heart failure are still not well explained. A few psychosocial factors have been studied and explain some of this risk, but other factors, like stress, remain largely unexplored in heart failure. This study aimed to (1) examine the association of stress with 6-month cardiac event-free survival, (2) examine the relationship of stress with salivary cortisol, and (3) examine the association of salivary cortisol level with 6-month cardiac event-free survival.
Method:
A total of 81 heart failure patients participated. Stress was measured using the brief Perceived Stress Scale. Cortisol was measured from unstimulated whole expectorated saliva. Cox regression analyses were used to determine whether stress predicted event-free survival, and if salivary cortisol predicted event-free survival. Linear and multiple regressions were used to determine the association of stress with salivary cortisol.
Results:
Stress was not a significant predictor of event-free survival in heart failure (heart rate = 1.06; 95% confidence interval = 0.95–1.81; p = 0.32). Salivary cortisol was a significant predictor of event-free survival in the unadjusted model (heart rate = 2.30; 95% confidence interval = 0.99–5.927; p = 0.05), but not in the adjusted model. Stress (β 1.06; 95% confidence interval = 0.95–1.18; p = 0.32) was not a significant predictor of salivary cortisol level.
Conclusion:
Stress is a complex phenomenon, and our measure of stress may not have captured it well. Alternatively, the physical stressors acting in heart failure produce levels of neurohormonal activation that mask the effects of psychosocial stressors or an indirect association of stress with outcomes that is mediated through another construct. Future studies are needed to investigate stress in patients with heart failure to provide definitive answers.
Introduction
Worldwide, heart failure (HF) is considered a major public health problem.1–9 Although there have been significant therapeutic advances in pharmacological and surgical treatment of HF, hospital admission and readmission rates are extremely high for exacerbations of HF, and the 1-year mortality rate of HF patients with progressive symptoms still approaches 40%.10–13 The high mortality and morbidity rates associated with HF are not completely explained by biological mechanisms, 14 as psychological factors are important predictors of morbidity and mortality in HF. One psychological factor that might contribute to morbidity and mortality in patients with HF is stress.14–20
Stress is the condition that occurs when environmental demands exceed an individual’s ability to adapt to the demands. 21 A prerequisite for stress to occur is the individual’s perception that stressors are perceived as a persistent threat to their physical and/or psychological health or well-being. 22 Stress is an umbrella term that summarizes the effects of psychological and environmental stressors on an individual’s physical and mental health.23,24 HF is commonly perceived by patients as a very stressful experience both physically and psychologically.16,25
There is limited information about the relationship between stress and HF. However, in patients with cardiovascular disease, psychological stress was associated with multiple adverse effects on patient health outcomes.26–30 In patients with cardiovascular disease, psychological stress has been associated with decreased coronary artery blood supply, greater severity of cardiac disease, worse prognosis, and poorer cardiac function.31–35 Stress is also associated with multiple psychological factors such as anxiety and depression that have negative effects on health outcomes like mortality and morbidity in HF and cardiac disease.15,36–38
Given the likelihood that HF is a substantial stressor for many patients, the examination of the role of stress on health outcomes in patients with HF is important. The specific aims of this study were to (1) examine the association of stress with 6-month cardiac event-free survival, controlling for anxiety, depression, and New York Heart Association (NYHA) functional class; (2) examine the relationship of stress with salivary cortisol; and (3) examine the association of salivary cortisol level with 6-month cardiac event-free survival, controlling for age, gender, and NYHA class. We hypothesized that stress and salivary cortisol are predictors of event-free survival in HF patients. In addition, we hypothesized that stress is a predictor of salivary cortisol level in HF patients.
Method
Design, sample, and setting
A prospective design was used in which patients were followed for 6 months to determine occurrence of 6-month cardiac event-free survival, defined as time to the combined endpoint of cardiac rehospitalization or all-cause death. This study was a part of the Heart Outcomes Prevention Evaluation (HOPE) study at the University of Kentucky that investigated depression among hospitalized patients with HF. The parent study and the current study were approved by the Institutional Review Board at the University of Kentucky. The sample consisted of 81 patients with confirmed HF who were hospitalized for cardiac reasons (i.e. hospitalization for HF, acute coronary syndrome, dysrhythmias) at the University of Kentucky Chandler Medical Center or GoodSamaritanHospital, which are located in Lexington, Kentucky.
Patients with a diagnosis of chronic HF confirmed by echocardiogram and cardiologist were eligible for participation in the study if they met the following criteria: (1) admitted to the hospital with a primary or secondary diagnosis of exacerbation of chronic HF or any other cardiac diagnosis, (2) 21 years or older, (3) able to read and speak English, and (4) no obvious cognitive impairment. Patients with HF with either preserved or non-preserved ejection fraction were included. Patients were excluded from the study for the following reasons: (1) co-existing terminal illness likely to be fatal within the next 6 months; (2) presence of a left ventricular assist device, continuous inotropic infusion, or hospice care; (3) active suicidality (defined as choosing option 2 or 3 on item 9 of the Beck Depression Inventory-II); (4) history of the death of a spouse or child within the past month; (5) history of psychotic illness or bipolar illness; (6) current alcohol dependence or other substance abuse; and (7) new-onset HF.
Measures
Stress
Stress was measured using the brief version of the Perceived Stress Scale. 39 The brief version consists of a 4-item scale which has been demonstrated to be reliable and valid. 39 The 4 items are as follows: (1) How often have you felt that you were unable to control the important things in your life? (2) How often have you felt confident about your ability to handle your personal problems? (3) How often have you felt that things were going your way? (4) How often have you felt difficulties were piling up so high that you could not overcome them? Each item is rated by respondents on a scale ranging from 0 (never) to 5 (very often). Higher scores indicate greater levels of stress. In this study, the Cronbach’s alpha of the 4-items perceived stress scale was 0.70.
Event-free survival
Event-free survival was defined as the combined endpoint of cardiac rehospitalization or all-cause death. Hospitalization data were determined through a combination of patient and family interviews and a review of medical records. Hospitalizations were verified by trained research assistants who reviewed medical records and clinic notes on a weekly basis. Given the possibility that patients could have been hospitalized at different facilities other than the three sites involved in the study, trained research assistants carefully questioned the patients or family members by phone to determine whether hospitalization had occurred.
All-cause mortality was determined by interview with the patient’s family, medical record review, and review of county death records. At enrollment, the patient was asked for contact information of a close friend or family member in case the patient could not be contacted. At follow-up, if a patient could not be reached by phone, hospital records were searched. When information regarding the patient was not available, family members or friends were contacted. If these contacts could not be reached, county death records were used to determine patient death.
Salivary cortisol
Cortisol was measured from saliva obtained from patients at baseline through an unstimulated whole expectorated saliva collection protocol. Patients were provided a 20-mL vial containing freeze dried protease inhibitor. Patients were asked to swallow once and begin expectorating approximately every 20–30 s until 5 mL is collected. The specimen was kept on ice until returned to the lab. Salivary sample was obtained in the morning (9:00 a.m.) on the day of enrollment. The salivary samples were stored in a −80°C freezer until they were analyzed using a commercially available enzyme immunoassay kit designed for cortisol quantification in saliva (Salimetrics LLC, State College, PA, USA). This assay has a sensitivity of <0.007 µg/dL and is strongly correlated with serum cortisol measurement (0.91). Salivary cortisol is considered a more accurate and reliable measure for the clinical assessment of adrenocortical function than serum cortisol.40,41
Depressive symptoms
The Patient Health Questionnaire–9 (PHQ-9)42,43 was used to measure depressive symptoms. The PHQ-9 is a 9-item, self-reported measure of depressive symptom severity. Patients respond to each item on a Likert scale ranging from 0 (not at all) to 3 (nearly every day). The total summary score can range from 0 to 27; a higher score reflects more severe depressive symptoms. Good internal consistency, stability, construct, and concurrent validity of the PHQ-9 have been supported.42,44 The standard published cut point of 10 was selected in this study for PHQ-9 to identify those in the sample who had moderate to severe depressive symptoms. 28 This cut point was reported to have 88% sensitivity and 88% specificity for diagnosing major depression.44,45 In this study, the Cronbach’s alpha of the PHQ-9 scale was 0.73.
Anxiety
The Brief Symptom Inventory (BSI) anxiety subscale was used to measure anxiety.46,47 The subscale consists of six questions, each of which is scored by patients using a scale that ranges from 0 (not at all) to 4 (extremely). The total score is calculated as the mean of the 6-item scores. Thus, the possible range of scores for the anxiety scale is 0–4, with higher scores indicative of higher levels of anxiety. The BSI has demonstrated internal consistency, stability, construct, and concurrent validity in other studies.46,47 In this study, the Cronbach’s alpha of the anxiety scale was 0.77. A standard published mean score of 0.35 was used to identify those in the sample who were anxious and those who were not anxious. 48
Demographic and clinical variables
Data on demographic variables and clinical characteristics were collected by reviewing medical records and interviewing patients. These variables included age, gender, ethnicity, and NYHA class. The NYHA class indicates the level of functional impairment reported by patients as a result of symptoms and was rated by trained research nurses. These variables were selected because of their effects on the outcome variable as suggested in the literature.45,49
Procedure
Protocols for this study were approved by institutional review board of The University of Kentucky. All procedures were in accordance with institutional guidelines for research using human subjects. Hospitalized patients were identified by clinicians and referred to research staff. The research staff determined the patient’s eligibility. The study was thoroughly explained to each patient, and signed consent was obtained after answering any questions about the study. The research staff met with the patient to administer study questionnaires via the web-based SurveyMonkey. The questionnaires took approximately 20 min to complete. A paper copy also was offered to the patient if they did not feel comfortable with the web-based survey.
As a part of HOPE study, patient were contacted by phone to complete the follow-up questionnaire at 2 weeks, 3 months, and 6 months from hospital discharge. At each telephone contact, the research staff asked the patient whether he or she has been hospitalized or visited the emergency unit. At the end of the study period and intermittently thereafter, hospital records were reviewed to confirm deaths, re-hospitalizations, or emergency department visits.
Salivary samples were obtained for cortisol measurement in the morning at baseline at the time of questionnaires completion. All saliva samples were stored at −80°C until analysis of samples at the University of Kentucky Dentistry Research laboratory.
Statistical analysis
Data were analyzed using SPSS software, version 20.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics, including mean, standard deviation, and frequency distribution, were used to describe sample characteristics. To test Specific Aim 1, unadjusted, followed by adjusted, Cox regression analyses were used to determine whether stress independently predicted event-free survival. The following covariates were considered in the adjusted analysis and entered hierarchically: age, gender, NYHA class, and anxiety and depression. Demographic and clinical variables were entered first into the model. Then, anxiety and depressive symptoms were entered. Finally, stress as a continuous level variable was entered into the model. The same analysis was conducted using categorical level variables with the mean and median as cut-points.
To test Specific Aim 2, linear and multiple regressions were used to determine the association of stress with salivary cortisol. This analysis included a sample of 70 patients because not all of the patients were able to provide a salivary sample. Two groups, low and high salivary cortisol level, were created based on the median of salivary cortisol level and used in this analysis. This analysis was conducted using both categorical and continuous level variables of salivary cortisol. To test Specific Aim 3 using the same sample size (n = 70), unadjusted Cox regression analysis was conducted to determine whether cortisol predicted event-free survival. Then, a hierarchal Cox regression analysis was used controlling to the following covariates: age, gender, and NYHA class. Again, this analysis was conducted using both categorical and continuous level variables of salivary cortisol. The demographic and clinical variables were entered first and cortisol was entered second. The assumptions of all Cox regressions, and linear and multiple regressions, were tested for violations and none were noted. A p-value of ≤0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of patients (N = 81) are summarized in Table 1. The average stress score in this sample was 9.47 ± 3.86, with a range of 4–20. No cut point has been defined for this instrument to date; however, the mean stress score in this study was higher than has been reported in other studies for the same scale.39,50,51 For example, in a study of college students, the mean score was 5.6 ± 3.6, 39 and in a study of Chinese patients with cardiac conditions, the mean was 6.0 ± 2.0. 51
Sample characteristics (N = 81).

SD: standard deviation; NYHA: New York Heart Association.
The average anxiety score was 0.58 ± 0.68. Using the published BSI average in the general population of 0.35, 48 46.7% scored as anxious. The average depressive symptoms score was 8.00 ± 4.87, and using the standard published PHQ-9 cut point 10, 28 29.6% of the sample was suffering from depressive symptoms. The average salivary cortisol level was 0.32 ± 0.23 µg/dL.
Specific aim 1: stress and the prediction of event-free survival
A total of 28 (35%) patients had an event. Six (7.4%) died and 22 (27.2%) were hospitalized for cardiac reasons during the study. In the unadjusted model, stress (heart rate (HR) = 1.04; 95% confidence interval (CI) = 0.95–1.13; p = 0.46) was not a predictor of event-free survival. In the adjusted model with age, gender, NYHA, anxiety, and depressive symptoms as covariates, the overall model (χ2 = 3.14, df = 6; p = 0.79) was not significant (Table 2). None of the variables were significant in any step of the hierarchal Cox regression. In the final model, stress (HR = 1.06; 95% CI = 0.95–1.81; p = 0.32) was not a predictor of event-free survival. An additional exploratory Cox regression analysis was conducted using stress as a categorical variable. The results were similar in that stress did not predict the outcome.
Adjusted Cox proportional hazards regression model of variables associated with cardiac event-free survival (stress model).

CI: confidence interval; NYHA: New York Heart Association.
Specific aim 2: association of stress and salivary cortisol
The linear and multiple regressions (n = 70) showed that stress level was not a significant predictor of salivary cortisol (Tables 3 and 4). In addition, none of the covariate variables (age, gender, NYHA, and anxiety) in the multiple regression analysis was a significant predictor of salivary cortisol except age (HR = 0.26; 95% CI = 0.00–0.01; p = 0.04) (Table 4). An additional exploratory Cox regression analysis was conducted using salivary cortisol as a categorical variable. The results were similar in that salivary cortisol did not predict the outcome.
Linear regression of stress level associated with salivary cortisol of patients with heart failure.
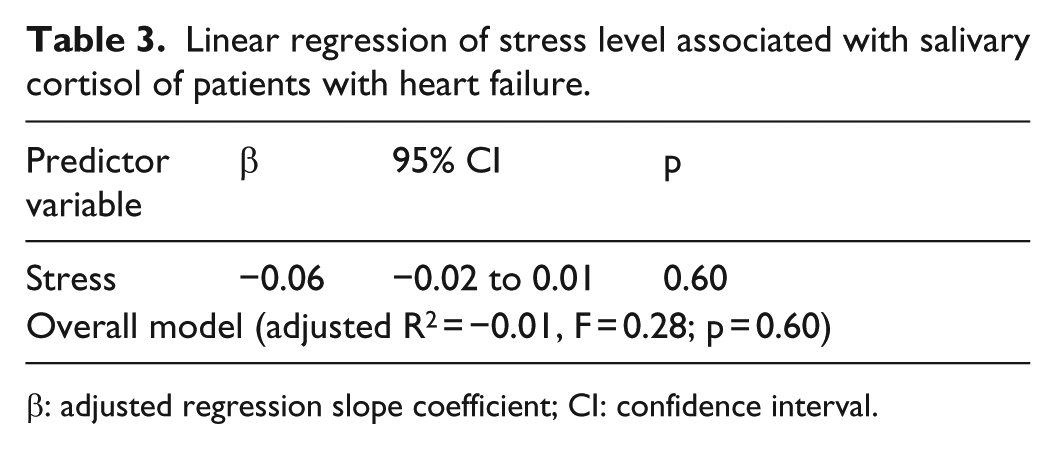
β: adjusted regression slope coefficient; CI: confidence interval.
Multiple linear regression of variables associated with salivary cortisol of patients with heart failure.

β: adjusted regression slope coefficient; CI: confidence interval; NYHA: New York Heart Association.
Specific aim 3: salivary cortisol and the prediction of event-free survival
In the Cox regression analysis, where salivary cortisol level was the independent variable (n = 70), 24 patients (34.3%) had an event. In all, 4 (5.7%) of the participants died and 20 (28.6%) were hospitalized during the study. In an unadjusted model, salivary cortisol (HR = 2.30; 95% CI = 0.99–5.93; p = 0.05) was a significant predictor of event-free survival (Table 5 and Figure 1). However, in the adjusted model with age, gender, and NYHA as covariates, the overall model (χ2 = 5.34, df = 4; p = 0.25) was not significant. None of the variables were significant in any step of the hierarchal Cox regression. In the final model, higher level of salivary cortisol (HR = 2.03; 95% CI = 0.84–4.93; p = 0.12) was not a predictor of event-free survival (Table 6). An additional exploratory Cox regression analysis was conducted using salivary cortisol as a continuous variable. The results for both adjusted and unadjusted models were not significant.
Unadjusted Cox proportional hazards regression model of variables associated with cardiac event-free survival (salivary cortisol model).

CI: confidence interval.
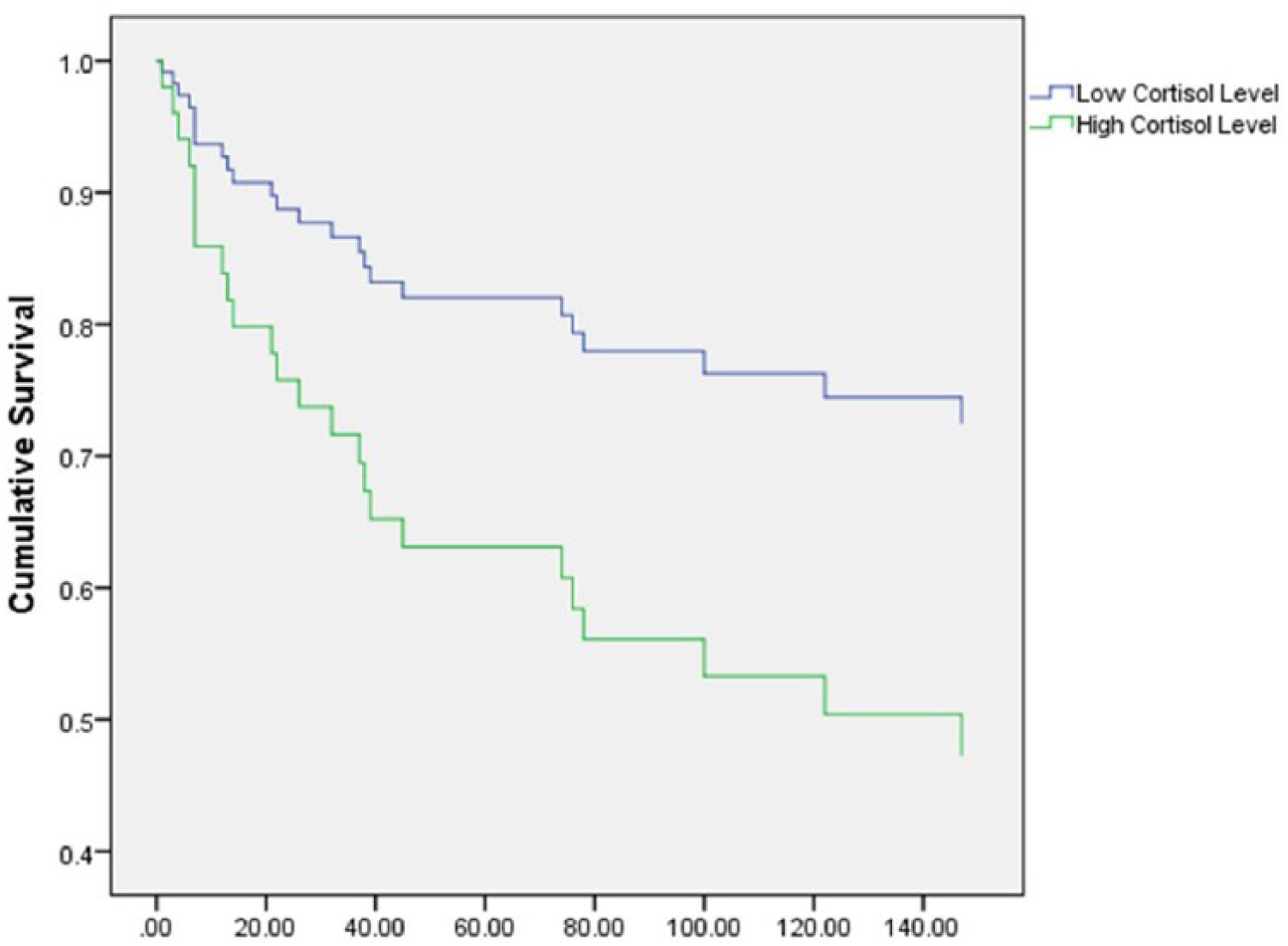
Event-free survival according to salivary cortisol level.
Adjusted Cox proportional hazards regression model of variables associated with cardiac event-free survival (salivary cortisol model).
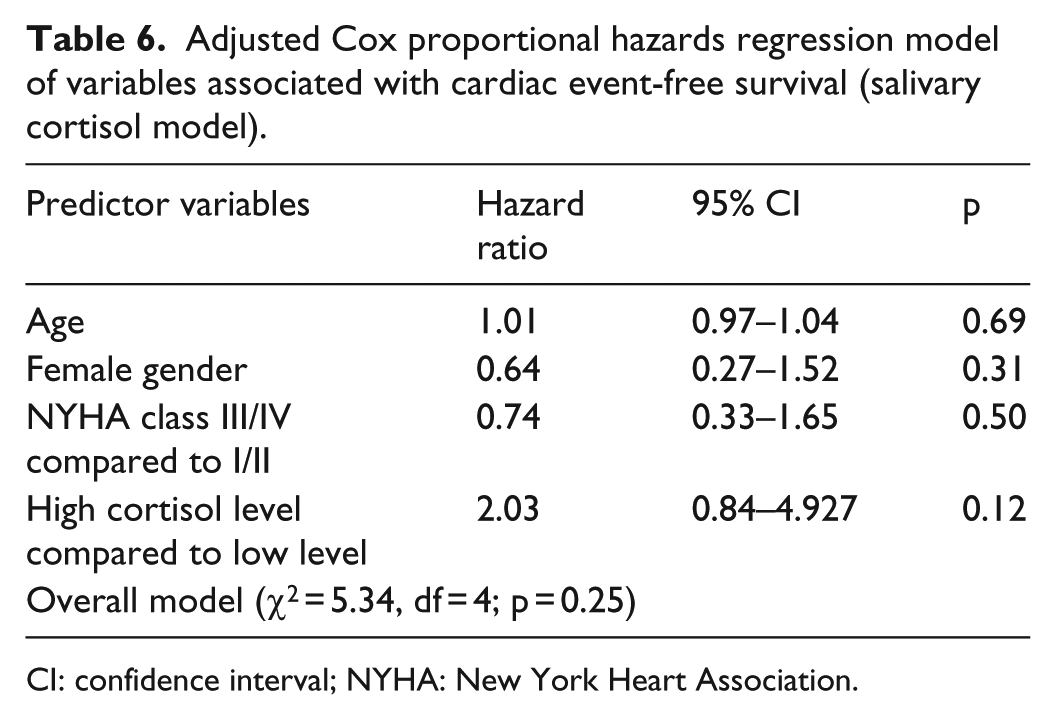
CI: confidence interval; NYHA: New York Heart Association.
Discussion
Psychosocial factors such as depression, anxiety, and lack of social support are associated with poor health outcomes in adults with HF.11,52 Clinicians and researchers commonly suggest that patients with HF have high levels of stress and that these levels of stress might contribute to poor outcomes. 53 To the best of our knowledge, this is the first study to investigate stress and associated cortisol level as predictors of cardiac morbidity and all-cause mortality in patients with HF. Based on our literature review and the scientific background related to HF, stress, and morbidity and mortality, we hypothesized that stress and salivary cortisol would be a predictor of 6-month cardiac event-free survival. We also hypothesized a significant association between stress level and salivary cortisol level. None of these hypotheses were supported expect that salivary cortisol was a significant predictor of 6-month cardiac event-free survival in the unadjusted model only. Our findings suggest that stress level was not associated with cardiac rehospitalization and mortality among HF patients.
Our hypotheses were based on the physiological mechanisms whereby stress may affect the progression of cardiovascular disease in general. Stress is thought to involve the hypothalamic–pituitary–adrenocortical (HPA). Much of the research on animals and humans suggests that psychological factors can influence the HPA axis, which controls the release of cortisol, a glucocorticoid that is secreted by the adrenal cortex to support and control physiological functions. 54 Over the past decades, many investigators have concluded that physical and psychological stressors are capable of activating the HPA axis and increasing cortisol level in the blood stream. 54 Through cortisol, the HPA supports physiological functions and regulates other systems. However, prolonged elevation in cortisol due to frequent stress is associated with many negative biological effects such as suppression of the immune system, damage to hippocampal neurons, and development and progression of chronic diseases like diabetes and hypertension.34,55 In HF, cortisol may contribute to the progression of cardiac damage by acting as a mineralocorticoid receptor (MR) agonist in the cardiac muscle where cortisol mimics the physiological and pathophysiological effects of aldosterone.56–59 Given these data, it is crucial to determine whether the stressors that are associated with HF activate the cortisol system and contribute to the onset or exacerbation of certain health outcomes.
Although there is evidence suggesting a relationship between stress and poor outcomes in cardiac patients without HF, the overall picture presented by the literature is one of conflicting findings. 60 Stress, variably defined as psychological, psychosocial, and mental stress, has been shown to predict mortality and morbidity in patients with cardiovascular diseases.61–63 Others, with large sample sizes, have found no association between stress level and increased admission rates related to cardiovascular disease. 64 In fact, some of these investigators demonstrated an inverse relationship between stress and all-cause mortality, as well as cardiac mortality. 64 Other investigators have demonstrated a difference between men and women in the prediction of mortality by stress in hospitalized medical patients.50,51 Stress in male patients predicted all-cause mortality; however, no association was found between stress and mortality among women.65,66 Investigators explained those results by stating that men are more vulnerable to stress than women. In addition, they expressed concerns that use of the two-question short version of the perceived stress scale did not capture some aspects of the stress phenomena.65,66
Our neutral finding about the relationship between stress and outcomes may be related to our small sample size, yet other investigators with very large sample sizes have similarly failed to find an association. 64 Although patients in our sample had a higher stress level compared to other populations,39,51 the average score on the stress instrument was only moderately high. Thus, it may be that patients in this sample did not experience a stress level high enough to demonstrate the hypothesized relationship. Another potential explanation for our finding is that the instrument did not adequately capture stress. We used the 4-item perceived stress scale, which has been demonstrated to be valid and reliable; nonetheless, the full instrument may have provided more complete information about stress level than the short version.39,51,67 The 6-month follow-up period may have been too short to capture the effect of stress on the health outcomes in patients with HF. Another possible explanation is that there is no relationship between stress level and outcomes in patients with HF. This explanation is supported by the number of investigations in which no relationship has been found in patients with a variety of health conditions.64,68,69 A final possible explanation is that there is an indirect association of stress with outcomes that is mediated through another construct such as coping.
We found no association between stress level and salivary cortisol level. Our findings are consistent with a study of breast cancer patients that showed no significant relationship between stress and salivary cortisol level. 70 Our study was similar to this study of breast cancer patients in that medically ill individuals with conditions that may be stressful were studied. In a literature review 71 designed to evaluate salivary cortisol as a biomarker of self-reported mental stress in field studies of healthy adults, the authors examined 14 studies published in medium or high quality journals. Results from eight studies demonstrated no association between self-reported mental stress and cortisol response: in four studies, there was a positive association, and in two studies a negative association. 71 They concluded that in healthy adults, there were insufficient data to support a relationship and postulated that the association, if present, might only be evident in those with extremely high levels of stress. There are no other reviews more relevant to our sample of HF patients, but the suggestion that patients may need to experience very high levels of stress for the association to become evident is valid to our sample.
Our finding showed an association between salivary cortisol level and all-cause mortality in patients with HF in the unadjusted model which is consistent with those of Yamaji et al. 72 who found that serum cortisol levels were a predictor of cardiac events patients with chronic HF. However, in the adjusted model, that association was no longer significant. Similarly, others have found no such relationship between cortisol and acute coronary events among patients with acute coronary syndrome. 73 The investigators relate their negative results to the interruption in cortisol rhythms during hospitalization, and this explanation may be relevant to our sample.
Study strengths and limitations
Strengths of our study include use of valid and reliable instruments to measure stress, salivary cortisol, and other covariates. Furthermore, we investigated multiple associations in this study that will form a foundation for future research in the field who are interested in stress and its effect on health outcomes in patients with HF.
The sample size of our study was a limitation that may have hindered our ability to demonstrate potential associations. As previously noted, however, a failure to find these associations has been noted in several studies with much larger sample sizes. The use of the 4-item perceived stress scale may limit the amount of information that we are able to collect related to stress; however, we used strict protocols and reliable and valid instruments for patients with HF.47,74–76
Conclusion
Our findings suggest that there is no relationship between stress level, as measured using the 4-item Perceived Stress Scale, and cardiac rehospitalization and all-cause death in patients with HF. Our findings also suggest that in the setting of HF, a condition that produces high levels of background physiological stress, there is no association between self-reported stress and salivary cortisol. Before these findings can be accepted, future studies among HF patients with higher levels of stress and in larger sample sizes must be conducted.
Footnotes
Acknowledgements
All the authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Declaration of conflicting interests
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Nursing Research or the National Institutes of Health. Financial sponsors played no role in the design, execution, analysis, and interpretation of data or writing of the study.
Funding
This work was supported by the National Institutes of Health, National Institute of Nursing Research (NIH, NINR P20 Center funding 5P20NR010679; NIH, NINR 1 R01 NR009280 (Terry Lennie, PI) and R01 NR008567 (Debra Moser, PI)), and K23 NR013480.