
Abstract
Background:
Delirium is still a common complication among older adults. Established multifactorial interventional programs focus on intrahospital management. Except general recommendations as maintaining vital parameters, prehospital management stays unacknowledged. There is a contrast between insufficient prehospital pain management and analgesics possibly contributing to delirium.
Objectives:
Our aim was to evaluate current practice of prehospital management in terms of pain management and transport. Secondary aim was to evaluate if medication administered by Emergency Medical Services influences the incidence of perioperative delirium in patients ⩾ 70 years.
Methods:
A retrospective analysis of 137 patients was performed in 2020 to 2021. The analysis is based on screened patients within a prospective observational cohort study investigating postoperative delirium incidence in a study cohort of patients ⩾ 70 years who received surgical treatment due to proximal femur fracture at a geriatric level I trauma center. The data were blinded for further analysis of prehospital protocols. We evaluated basic demographic data, parameters included in the current documentation protocol and recorded measures including administration of medication.
Results:
Mean age of the study collective was 86.9 (SD ± 6.8) years with 66% being female. Documentation frequency decreased following initial assessment. No correlation between pain level, administration of medication and the occurrence of perioperative delirium was found. More than half presented with pain ⩾4/10 NRS. Overall analgesia was initiated in only 10% in the entire cohort, mostly by emergency physicians. We saw a correlation between preexisting dementia and preoperative delirium and a slightly higher rate of delirium in patients with suspected dehydration.
Conclusions:
Prehospital pain management and documentation is still insufficient in older patients. If any correlation between different types of prehospital analgesia and perioperative delirium is to be found we first need to implement a sufficient standard of care regarding pain management. Fluid substitution can be useful if the individual state of dehydration is evaluated.
Keywords
Introduction
The ongoing research about the occurrence and the consequences of perioperative delirium has been spanning over five decades and has been known even longer. 1 Delirium is still a common acute complication, which negatively impacts the morbidity and mortality among older people > 65 years.2–4 The incidence of perioperative delirium in patients with proximal femur fractures has been described from 13% to 50%.5–7
The focus of previous research has been on recognizing risk factors and establishing multifactorial interventional programs.3,6 Known risk factors are inter alia higher age, low BMI, preexisting cognitive dysfunction, polypharmacy, delay between admission and surgery, and nonsufficient pain relief.3,5,6,8 The spotlight of interventional programs focused on measures within the hospital. Some of the mentioned aspects are a continuous pain relief with paracetamol as first-line analgesic in combination with opioids, correction of sensory deficit, early surgery, treatment of postoperative complications with, for example, transfusions and continuous fluid management.6,7,9–11
Prehospital management however is not usually acknowledged, and although the undertreatment of pain is frequently leading to perioperative delirium, it is mostly discussed after admittance at the Emergency Department. 12 As for prehospital recommendations, there are a few and overall general recommendations such as supplemental oxygen if needed, fluid supplementation, maintenance of normotension and normothermia as well as avoiding delay in transportation. 6
The number of elderly patients managed by Emergency Medical Services (EMS) constantly rises, with patients > 65 years old accounting for half of all dispatches. 13 The EMS is faced with changed challenges regarding geriatric patients and subsequently with the possible influence on the incidence of intrahospital delirium.12,14,15 Some medications administered in the prehospital setting, such as sedatives and especially analgesics have the potential to contribute to the occurrence of delirium in geriatric populations.16–18 At the same time only a few patients with musculoskeletal injuries receive prehospital analgesia, with only 10% of patients with hip fractures receiving pain medication.19,20
What we thus see in current literature is insufficient pain management as known risk factor for delirium incidence standing in contrast to administered medication possibly contributing to postoperative delirium.16,19,21,22
In this context, our aim was to evaluate if the current practice of prehospital pain management in a cohort of patients > 70 years and to evaluate if the prehospital administration of medications and specifically analgesics correlates with the incidence of delirium in a geriatric study population with a proximal femur fracture.
Methods
Study design
We performed a retrospective analysis of 160 patients between July 2020 and December 2021. The data were accessed from July 13, 2023, until February 25, 2024.
This study was approved by the ethics committee of the Hannover Medical School (9037_BO_S_2020) and was conducted in accordance with the Declaration of Helsinki. Informed consent to participate in this study was obtained in written form from all participants or their proxy/Legally Authorized Representative in advance.
The analysis is based on screened patients within a prospective observational cohort study investigating postoperative delirium incidence in a study cohort of older patients ⩾70 years of age who received surgical treatment due to proximal femur fracture at a geriatric level I trauma center. 23 The exclusion criteria of the primary study (no sensory aid devices, preexisting dementia, perioperative stroke, and preoperative delirium) did not apply for the retrospective analysis. The pseudonymized data for the retrospective analysis was screened for available preoperative assessment, and the data were then blinded and underwent further analysis of the prehospital protocols. After prehospital data collection, the delirium-prevalence data were brought together with the prehospital data for correlation analysis. The prevalence of preoperative and postoperative delirium was assessed through the 3-Minute Diagnostic Interview for Confusion.24,25 The preoperative assessment was done shortly after admission in the emergency department, the postoperative assessment was done twice daily for the first three postoperative days. Further data such as fracture type (femoral neck, intertrochanteric, subtrochanteric) is available from the parent cohort study; however, as fracture morphology does not affect prehospital assessment or management, nor does it constitute a prehospital exposure, it was not included in the present analysis.
Included were 160 patients, after exclusion of 23 patients without prehospital documentation protocols, due to intrahospital falls or interhospital transfer, 137 data sets remained. A STROBE flow diagram summarizing the patient screening and selection process is provided in Supplementary Figure 1. The prehospital analysis was based on the handwritten prehospital documentation protocols (MIND 6.1).26,27 Included parameters were basic demographic data (age and sex), date of admission including time of day. In line with standard EMS documentation practice, all clinical parameters were recorded within the ABCDE framework; therefore, reporting ABCDE completeness reflects the overall quality of prehospital documentation in this cohort. Based on the protocols we included following items at arrival on scene, arrival at hospital and in the emergency department:
A (Airway) B (Breathing) C (Circulation) D (Disability) E (Environment) Evaluation
Vital parameters: systolic and diastolic blood pressure, heart rate, arrythmia, peripheral oxygen saturation, breathing rate, temperature
Extended parameters: Blood glucose level, Glasgow Coma Scale, psychiatric or neurological disorders, pain level, dementia, pupil evaluation, skin condition
Measures: supplemental oxygen, peripheral intravenous catheters, positioning during transport, other
Medication: analgesia, sedation, Other
Suspected dehydration was defined as reduced skin turgor observed by EMS personnel during the physical examination. Preexisting dementia was recorded when noted in EMS documentation based on information available at the scene, including medical records, medication lists, or reports from family members or nursing home staff.
It was noted if the prehospital management was performed by paramedics or with the assistance of an emergency physician on scene. According to the regional EMS standards in 2021 paramedics were authorized to administer nalbuphine and esketamine independently, whereas opioids such as fentanyl or morphine required an emergency physician.
All data were collected using MS Excel (Version 16 for MAC, Microsoft Corporation, Redmond, WA, USA). It was not appropriate or possible to involve patients or the public in the design, conduct, reporting, or dissemination plans of our research.
Statistical analysis
The statistical analysis was done using SPSS Statistics 28.0 (SPSS Inc., IBM, Chicago, IL, USA). We performed the analysis with descriptive statistics (minimum, maximum, and mean ± standard deviation), frequencies as well as cross tabulation. We used Chi 2 -based crosstabulation with Phi and Cramer’s V coefficient for nominal data and Eta for categorial and quantitative data. Categorial variables were expressed as numerical quantity and percentage. Prehospital predictors were evaluated using logistic regression whenever model convergence was achievable. Variables with insufficient cell size or quasi-complete separation (e.g., analgesia administration, medication type) could not be reliably modeled and were therefore analyzed using univariable methods (bivariate Pearson’s correlation) only. Pain intensity was assessed using Spearman’s rank correlation due to its ordinal scale properties. A p-value < 0.05 was considered statistically significant, and a p-value < 0.01 was considered highly significant. Preoperative and postoperative delirium were analyzed as two separate outcomes, and all statistical analyses related to delirium were performed independently. Descriptive statistics refer to the full study cohort.
Results
The total number of assessed patients with prehospital data was 137. The demographic distribution of the patient collective was skewed towards female patients with 66.4%, only one-third (33.6%) were male. Median age of the collective was 86.9 (SD 6–8, range 72–104) years. Half (53.3%) of patients were in in their 80s. One-third was over 90 years old with 3.5% over 100 years. Only 12.5% were younger than 80. A total of 20.4% (n = 28) presented with known dementia.
A total of 89.8% (n = 123 of the study collective was managed by paramedics, 10.2% (n = 14) were attended by an emergency physician’s vehicle. 73.7 % (n = 101) had a suspected fracture of the hip or pelvis (see Table 1).
Basic demographic data, pain at arrival on scene and emergency department (ED), suspected diagnosis and incidence of delirium.

Abbreviation: ED, Emergency Department; EMS, emergency medical service; SD, standard deviation; A, at arrival on scene; T, arrival at the ED; NRS, numerical rating scale.
For recorded vital parameters as well as specific function-based evaluation, please see Tables 2 and 3.
Vital parameters taken at arrival and upon arrival at the ED.
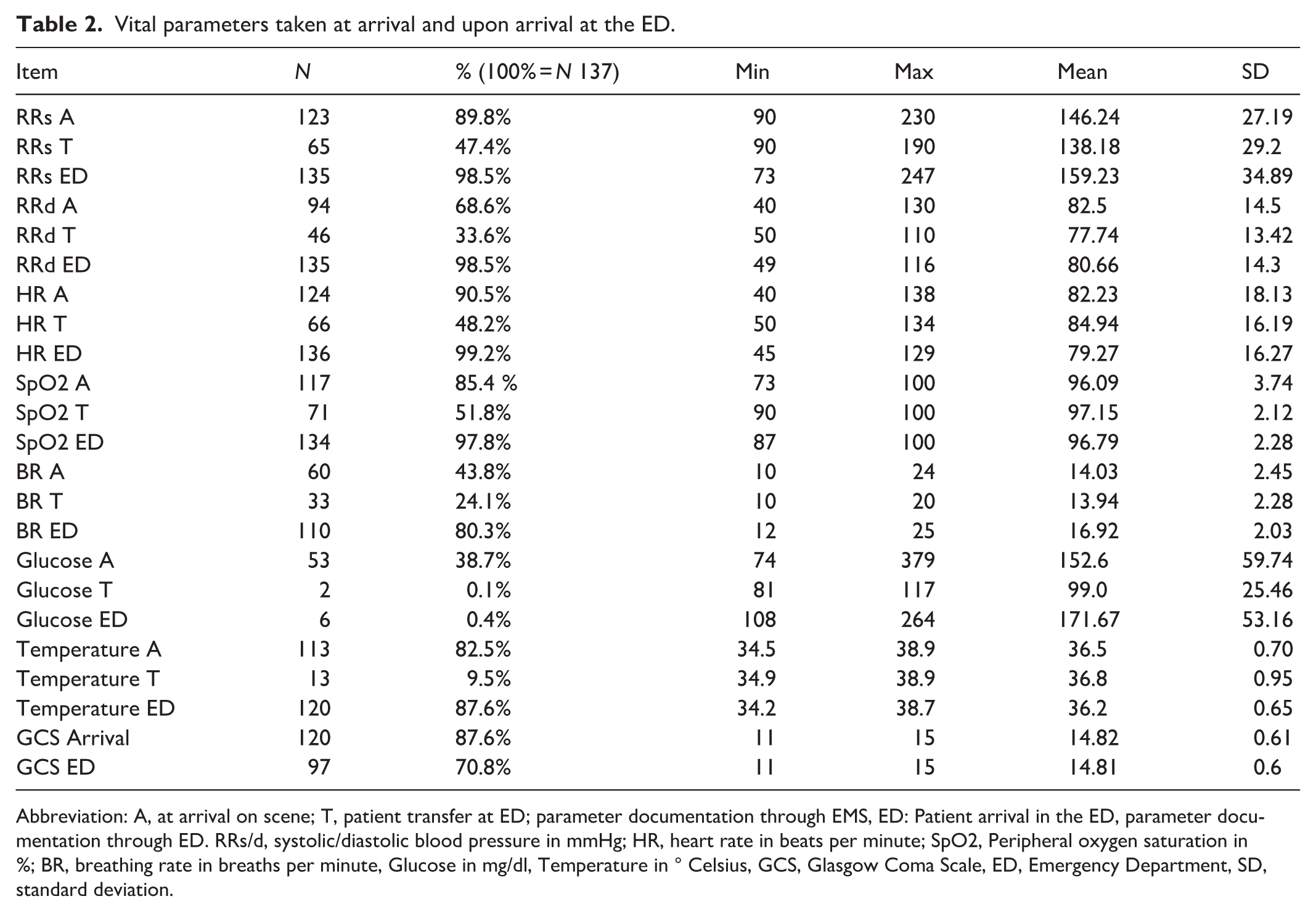
Abbreviation: A, at arrival on scene; T, patient transfer at ED; parameter documentation through EMS, ED: Patient arrival in the ED, parameter documentation through ED. RRs/d, systolic/diastolic blood pressure in mmHg; HR, heart rate in beats per minute; SpO2, Peripheral oxygen saturation in %; BR, breathing rate in breaths per minute, Glucose in mg/dl, Temperature in ° Celsius, GCS, Glasgow Coma Scale, ED, Emergency Department, SD, standard deviation.
Specific evaluation using the A/B/C/D-scheme (Airway, Breathing, Circulation, Disability incl. Pupil Evaluation), as well as body system-oriented evaluation (Neurological, Psychiatric, Skin, based on the MIND documentation protocols).

The frequency of recorded parameters declined after initial assessment. While blood pressure, heart rate, and peripheral oxygen saturation was recorded in over 89% of cases at arrival, it was documented in less than half of the cases a second time. Temperature was recorded in over 80% at arrival and decreased in documentation to less than 10% at transfer in the ED. Blood glucose was only measured in one-third of the cases.
Initial pain scores on arrival was recorded in 70.1% and ranged from 0 to 10 with an average of 5.48/10 on the Numerical Rating Scale (NRS). 24.9% presented with a pain level of 4–6/10 NRS. A total of 18.1% presented with pain <3/10 NRS and 27.1 % presented with pain >7/10 NRS. The pain at the time of patient transfer in the ED was recorded only in 55.5% and had an average of 4.74/10 NRS with each 21% <3/10 NRS and 4–6/10 NRS. Pain >7/10 NRS was seen in 11.4 % (see Table 1). Among the 54 patients presenting with moderate-to-severe pain (NRS ⩾ 4), only 4 (7.4%) received prehospital analgesia.
Medication was administered in only 13.1%, always intravenous. Medication for pain was given in 10.9% of patients. A peripheral intravenous catheter was used in 22.6% of all patients. Out of 101 patients with a suspected fracture only 13 received analgesia. A contusion was never treated with pain medication. The most-used analgesic agent was fentanyl with 60%. Esketamine was second (20%). Morphine and metamizole were cumulatively used in 20% of all analgesia. Sedation with midazolam was scarcely applied (3.6%) and only once together with esketamine. When analgesia was administered it was in 80% of the cases by an emergency physician and only in 20% by paramedics. Initial pain scores were significantly higher in patients managed with emergency physician involvement compared with those treated solely by paramedics (median NRS 8 [IQR 3] vs. 5 [IQR 4]; Mann–Whitney U = 161, p = 0.004). If analgesia was used emergency physicians clearly preferred the use of fentanyl and/or esketamine. Paramedics chose metamizole, nalbuphine was never used.
As for other performed measures such as oxygen supplementation, maintenance of body temperature, and transport position please see Table 4.
Administered medication and other performed measures by EMS as documented.

Abbreviation: EMS, emergency medical services; A, arrival; T, transfer; ED, emergency department.
No significant associations were found between vital parameters and either pre-or postoperative delirium. The administration of drugs and specifically analgesia showed no significant correlation with the occurrence of perioperative delirium in any univariable analysis. Attempts to include these variables in multivariable logistic regression were not feasible (see Table 5). Pain intensity at first medical contact showed a small but statistically significant positive correlation with preoperative delirium (ρ = 0.23, p = 0.024), but no association with postoperative delirium (ρ = −0.003, p = 0.978). Prehospital involvement of the emergency physician was not associated with the incidence of delirium.
Correlation between the administration of medication, preexisting dementia, and perioperative delirium.

R = Pearson’s coefficient.
A p-value < 0.05 was considered statistically significant, and a value <0.01 was considered highly significant.
The only clinically meaningful predictor identified was preexisting dementia, which was significantly associated with preoperative delirium (OR 2.80, 95% CI [1.17, 6.75], p = 0.021), but not with postoperative delirium (OR 0.93, [0.37, 2.30], p = 0.867). See Table 6.
Association of prehospital variables with preoperative and postoperative delirium.

Abbreviation: CI, confidence interval; OR, odds ratio; EPV, Emergency Physician Vehicle.
Spearman’s rho reported for ordinal pain scale (0–10).
Regression analysis for sedation and post-op delirium, as well as medication/analgesia for pre- and postoperative delirium was not possible; estimates are therefore not reported.
Reduced skin turgor did not reach statistical significance, but the descriptive pattern is notable; among patients with reduced skin turgor, 34% presented with preoperative delirium and 65% with postoperative delirium, compared with 24% and 50%, respectively, in patients without signs of dehydration.
Discussion
In our retrospective analysis, we evaluated the possible influence of administered medication on perioperative delirium in older patients with proximal femur fractures. The demographic distribution of our study cohort is consistent with the epidemiology of proximal femur fractures and with the baseline characteristics in studies referring to perioperative delirium. A predominantly female collective is typical.6,28
Despite that out of the patients where pain level was recorded, 67.7% presented with pain ⩾4/10 NRS, analgesia was administered only 10.9% of the cases. Sadly, this is congruent with previous literature older than a decade which described that only one in 10 patients with proximal femur fractures received analgesia through EMS. 19 Our study does not differ from other observations that although patients report having moderate or even severe pain, there isn’t a sufficient prehospital pain reduction in older people with musculoskeletal injuries.20–22 When we look at dominant risk factors for perioperative delirium, adequate pain management is always valued of utter importance.5–7,12 A possible way to address this problem was found in the prehospital administration of regional fascia iliaca bloc through paramedics. Paramedics were able to show in randomized controlled trials to decrease pain levels without impacting the scene times.29–33 However, it needs critical judgment since noninterventional pain relief is not yet sufficiently implemented in standard care. In addition, 80% of analgesic administration was done through an emergency physician, who was present only 10% of all cases. Thus, the given competencies of paramedics including the legal administration of analgesic agents like nalbuphine was not used. In addition, in 4% of the cases, a backboard or scoop stretcher was used for transport with a clear recommendation of avoiding those tools for patient transport. 34 Especially many factors of prehospital trauma management due to stressful circumstances, immobilization and inadequate pain management can increase the incidence of delirium.12,35
In the cases where analgesia was used, we did not find a correlation to the occurrence of delirium. It is important to note that the studies that described the effect of “DRIDS” it was mostly in relation to polypharmacy and regular intake of those substance groups preadmission to the hospital. 17 The classification of “DRIDS,” delirium-risk increasing drugs includes medication with an effect on the central nervous system, such as sedatives or analgesic, especially opioids and causes up to 39% of delirium cases.16–18 For analgesic treatment usually paracetamol is primarily recommended with the addition of geriatric-specific dosed opioids if needed to achieve adequate pain relief.6,7,35
While it is recommended within multimodal prevention programs to supplement 3 to 4l/min oxygen in the ambulance until 2 days postoperatively and to keep normotensive blood pressure, we could not see any correlation between initial vital parameters and peripheral oxygen saturation or oxygen supplementation.6,7 These results do need to be interpreted with caution since oxygen was supplemented in only 6.6% of the cases and the frequency of recorded parameters declined after initial assessment. Most vital parameters were documented in less than half of the patients for a second time. Other recommendations focus on general hydration through intravenous supplementation of at least one liter in the ambulance due to dehydration being one possible underlying cause for delirium.6,7,11,35 Consistent with this recommendation we saw a higher rate of perioperative delirium in patients with poor skin turgor and thus suspected dehydration. We think that an individual-based approach of fluid substitution at scene is important, which takes pre-existing medical conditions into account, as well as on scene evaluation of signs of possible dehydration.
Strengths of the study were a frequent number of cases with proximal femur fractures in a level I trauma center, data in line with previous literature, as well as no expected bias through archived protocols. Limitations of the study were the retrospective analysis of a prospective study design. As this was a retrospective observational study including all consecutive eligible patients during the predefined study period, no a priori sample size calculation was performed. The final sample size was determined by the number of cases with complete prehospital documentation. Missingness in prehospital variables—particularly repeat vital signs, temperature, and pain scores at transfer—is inherent to real-world prehospital workflows and not missing at random. Because such missingness is structurally determined rather than random, multiple imputation or sensitivity analyses were not appropriate. A statistical limitation was that several prehospital variables (e.g., administration of analgesia) showed very small cell counts and quasi-complete separation, which prevented stable estimation in multivariable logistic regression models. These constraints reflect the real-world frequency of certain prehospital interventions and should be considered when interpreting the effect sizes. Given that only 4 of 54 patients with moderate-to-severe pain received any analgesia, statistical power to detect an association between analgesia and delirium was extremely limited. The observed lack of statistical significance therefore reflects insufficient exposure rather than evidence of no effect, and should not be interpreted as proof that prehospital analgesia has no impact on delirium risk.
Operational metrics such as scene time and transport duration were not available in the dataset and do not reliably reflect analgesia administration due to the multifactorial nature of prehospital workflow. As with all observational studies, residual confounding cannot be fully excluded, particularly for the relationship between medication use and delirium. These associations were examined in detail in the parent cohort study.
Conclusion
The EMS encounter different challenges when dealing with older populations, so do the older adults. And while we did not find a correlation between prehospital measures and perioperative delirium, we did see that prehospital analgesia and documentation is still very insufficient. Fluid substitution can be useful if the individual state of dehydration is evaluated. The limitation of the study is also a result in itself—If any correlation between different types of prehospital analgesia and perioperative delirium is to be found, we first need to implement a sufficient standard of care regarding pain management.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251408226 – Supplemental material for Prehospital pain management in older adults with proximal Femur fractures: current practices and implications for delirium prevention
Supplemental material, sj-docx-1-smo-10.1177_20503121251408226 for Prehospital pain management in older adults with proximal Femur fractures: current practices and implications for delirium prevention by Vesta Brauckmann, Jan Busse, Alexander Ranker, Manfred Gogol, Gökmen Aktas, Torben Riecke and Christian Macke in SAGE Open Medicine
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
This study was approved by the ethics committee of the Hannover Medical School (9037_BO_S_2020) and was conducted in accordance with the Declaration of Helsinki.
Consent to participate
Informed consent to participate in this study was obtained in written form from all participants or their proxy/Legally Authorized Representative in advance.
Author contributions
V.B., C.M., and M.G. conceived of the presented idea. J.B., A.R., and M.G. developed and conducted the parent study in terms of the assessment of perioperative delirium. V.B., T.R., and G.A. collected the retrospective data. V.B. and G.A. verified the analytical methods. V.B. wrote the manuscript with support and revision by all authors. All authors discussed the results and contributed to the final manuscript. C.M. supervised the project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Clinical trial number
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.