
Abstract
Background
We compared the outcomes of three fixation techniques for Müller type C2 and C3 distal femoral fractures.
Methods
We retrospectively analyzed patients undergoing internal fixation for Müller type C2 and C3 distal femoral fractures via locking plate (Group A), lateral locking condylar plate and medial contoured reconstruction plate (Group B), and lateral locking condylar plate and anterior reconstruction plate (Group C). Knee joint functional recovery and functional outcomes were evaluated 12 months postoperatively.
Results
Patients included 34 men and 24 women aged 25 to 74 years (mean, 50.3 ± 10.73 years). Operating times were longest in Group B and similar in Groups A and C. Bleeding volume in Group A was smaller than in Group B and similar to that of Group C. Functional outcomes were excellent in 18 (31%) fractures, good in 24 (41%), moderate in 11 (19%), and poor in 5 (9%). Good-to-excellent results were achieved in 56%, 82%, and 83% of patients (Groups A, B, and C, respectively). Groups B and C's outcomes were superior to Group A's outcomes. No significant difference in postoperative complications between the groups existed.
Conclusion
Lateral locking condylar and anterior reconstruction plating was useful for complex type C distal femoral fractures.
Introduction
Distal femoral fractures account for less than 1% 1 of all fractures, and approximately 30%2,3 of femoral fractures occur in the distal femur. Müller type-C femoral fractures occur commonly in young patients sustaining high-energy accidents and older patients with osteoporosis who sustain low-energy fall-related fractures. 1
Operative treatment is considered the standard approach for distal femoral fractures, and conservative management may result in serious complications, such as knee stiffness, inadequate alignment, delayed union or non-union, and prolonged hospitalization and related morbidity. 4 Moreover, the outcomes of surgical fixation are consistently superior to those of conservative management. 5 To achieve better outcomes, three main problems that are commonly observed in Müller type C2 and C3 distal femoral fractures must be addressed. First, it is exhausting to obtain adequate exposure of the articular surface, particularly the medial femoral condyle and in coronal plane fractures. Second, the standard implants used for other types of distal femoral fractures, such as the condylar blade plate and supracondylar nails are not helpful for articular surface reduction and fixation. Third, with medial comminution and a short distal segment, there is a high incidence of loss of fixation and varus collapse. 6 , 7
To address the above issues, various types of internal fixation have been used for distal femoral fractures. In this study, we analyzed the outcomes of three fixation techniques for Müller type C2 and C3 distal femoral fractures.
Materials and methods
Between February 2017 and February 2019, we retrospectively reviewed data for 34 men and 24 women aged 25 to 74 years (mean, 50.3 ± 10.73 years) who underwent internal fixation for Müller type C2 and C3 distal femoral fractures. All patients were diagnosed with type C2 and C3 fractures according to Müller’s 8 classification; 36 patients were type C2, and 22 were type C3. All surgeries were performed by a single surgeon. A locking plating (single incision, Group A), lateral locking condylar plate and medial contoured reconstruction plate (dual incision, Group B), and lateral locking condylar plate and anterior reconstruction plate (single incision, Group C) were used according to implant availability at the time. The mechanisms of injury in Groups A, B, and C, respectively, were as follows: car accident: 13, 8, and 9; bicycle accident: 6, 5, and 7; and fall: 4, 4, and 2.
The repair methods were as follows: Group A (single-incision locking plate group): A 13- to 16-cm incision was made on the lateral side of the knee with the fracture end as the center. The periosteum was then peeled away to reveal the fracture end, the lateral column fracture was repositioned, the medial comminuted fracture was maintained along the line of force, and internal fixation with a locking plate and screws was performed on the lateral side. The procedure for Group B (dual-incision locking plate combined with reconstruction plate) was as follows: As for group A, the lateral column fracture was first repositioned and fixed, and then a 5- to 9-cm medial incision was created to reveal the medial column. The comminuted fracture block was repositioned, and a reconstruction plate was used to fix the medial fracture. In Group C (single-incision locking plate combined with reconstructive plate), a 12- to 15-cm incision was made anterolaterally with the fracture end as the center to reveal the lateral column fracture, the fracture was repositioned with locking plate screw fixation, the medial fracture was repositioned, and the distal femoral fracture was revealed by soft tissue retraction. Anterolaterally, the medial fracture was fixed with an anterolateral reconstruction plate.
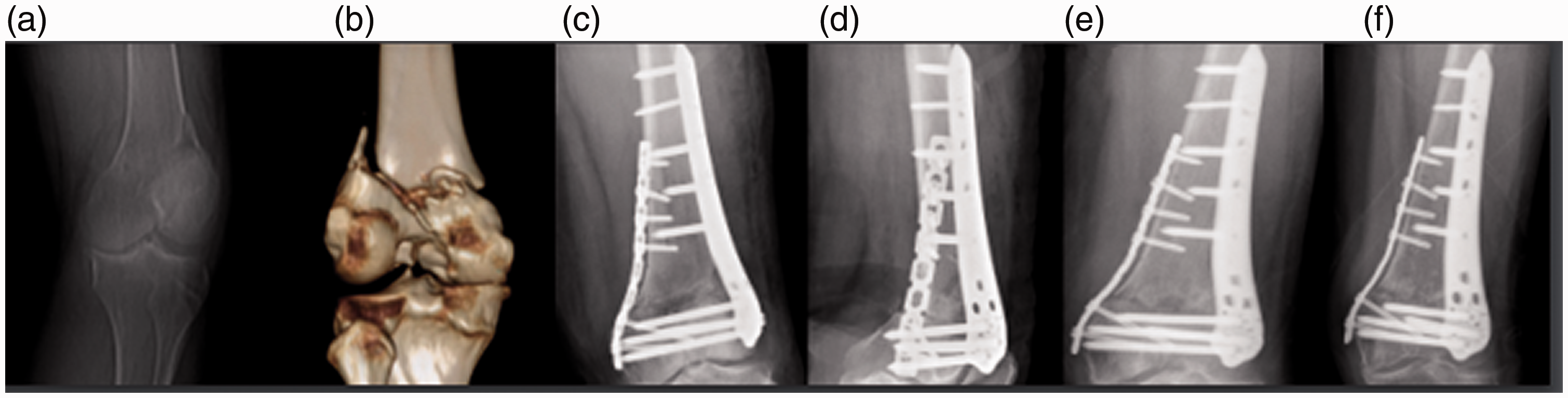
Patients were instructed to start isotonic contractions of the quadriceps, and ankle extension and flexion exercises, 1 to 2 days after surgery. Continuous passive motion (CPM) exercises were started 7 days after surgery, and radiographs were reviewed 4 to 12 weeks postoperatively. Patients were instructed to start partial weight-bearing and then to gradually start full weight-bearing according to the healing status of the fracture, in accordance with radiographic findings. Postoperative outpatient follow-up was performed for 12 months to assess fracture healing and functional recovery. Functional outcome was classified according to Schatzker and Lambert’s criteria 9 (Figure 1, Figure 2, and Figure 3).

The patient was a 70-year-old man with a C2 fracture of the right distal femur caused by a traffic-related injury. (a–d). Six days after the injury, single-incision locking plate combined with reconstructive plate repair was performed for distal femoral internal fixation. (e, f). Healing of the medial and lateral fractures was good on the postoperative radiographs at 6 and 12 months.

The patient was a 64-year-old woman with a C2 fracture of the right distal femur caused by a fall. Five days after the injury, single-incision locking plate cut-and-repeat internal fixation of the distal femur was performed. (a) Preoperative radiographs showing a comminuted fracture of the distal femur with loss of medial and lateral support; (b) Preoperative computed tomography (CT) three-dimensional (3D) reconstruction showing a comminuted fracture of the femoral shaft combined with an intra-articular fracture; (c) Postoperative orthoptic radiographs showing good fracture repositioning; (d, e) Six and 12 months after surgery, the fractures have healed well.
The patient was a 67-year-old woman with a C3 fracture of the left distal femur caused by a traffic-accident-related injury. Double-incision locking plate combined with reconstructive plate cut-and-repeat internal fixation of the distal femur was performed 7 days after the injury. (a) Preoperative radiograph showing a comminuted fracture of the distal femur with loss of medial and lateral support; (b) Preoperative computed tomography (CT) three-dimensional (3D) reconstruction showing a comminuted fracture of the femoral shaft combined with an intra-articular comminuted fracture; (c, d) Postoperative frontal and lateral radiographs showing good fracture reduction; (e, f) Postoperative radiographs at 6 and 12 months, respectively, showing good fracture healing.
The study was approved by the ethics committee of Cangzhou Hospital of Integrated Traditional Chinese Medicine and Western Medicine. Verbal informed consent was obtained from all participants in the study prior to surgery.
Data were analyzed using PASW® 18 (SPSS Inc., Chicago, IL, USA). Kruskal–Wallis analysis of variance (ANOVA) was used to compare age, length of hospital stay (LOS), operating time, and bleeding volume between the three groups. To detect significant differences between the groups, the Chi-square and Fisher’s exact test were used to assess gender and functional outcomes; P < 0.05 was considered statistically significant.
Results
The patients’ general data are summarized in Table 1. There were 14 men and 9 women in Group A (n = 23), with a mean age of 49.4 ± 13.0 years, and a mean LOS of 15.3 ± 1.8 days. In Group B (n = 17), there were 11 men and 6 women, with a mean age of 54.6 ± 13.1 years and a mean LOS of 16.5 ± 2.3 days. In Group C (n = 18), there were 9 men and 9 women, with a mean age of 47.2 ± 12.3 years and a mean LOS of 14.7 ± 1.5 days. There was no significant difference between the three groups regarding the mechanism of injury. The mean operating time was 96.2 ± 17.1 minutes, 114.2 ± 18.3 minutes, and 101.7 ± 17.0 minutes in Groups A, B, and C, respectively. The mean bleeding volume was 239.0 ± 51.1 mL, 293.0 ± 55.2 mL, and 255.2 ± 51.1 mL in Groups A, B and C, respectively (Table 1).
Comparison of the three fixation techniques.
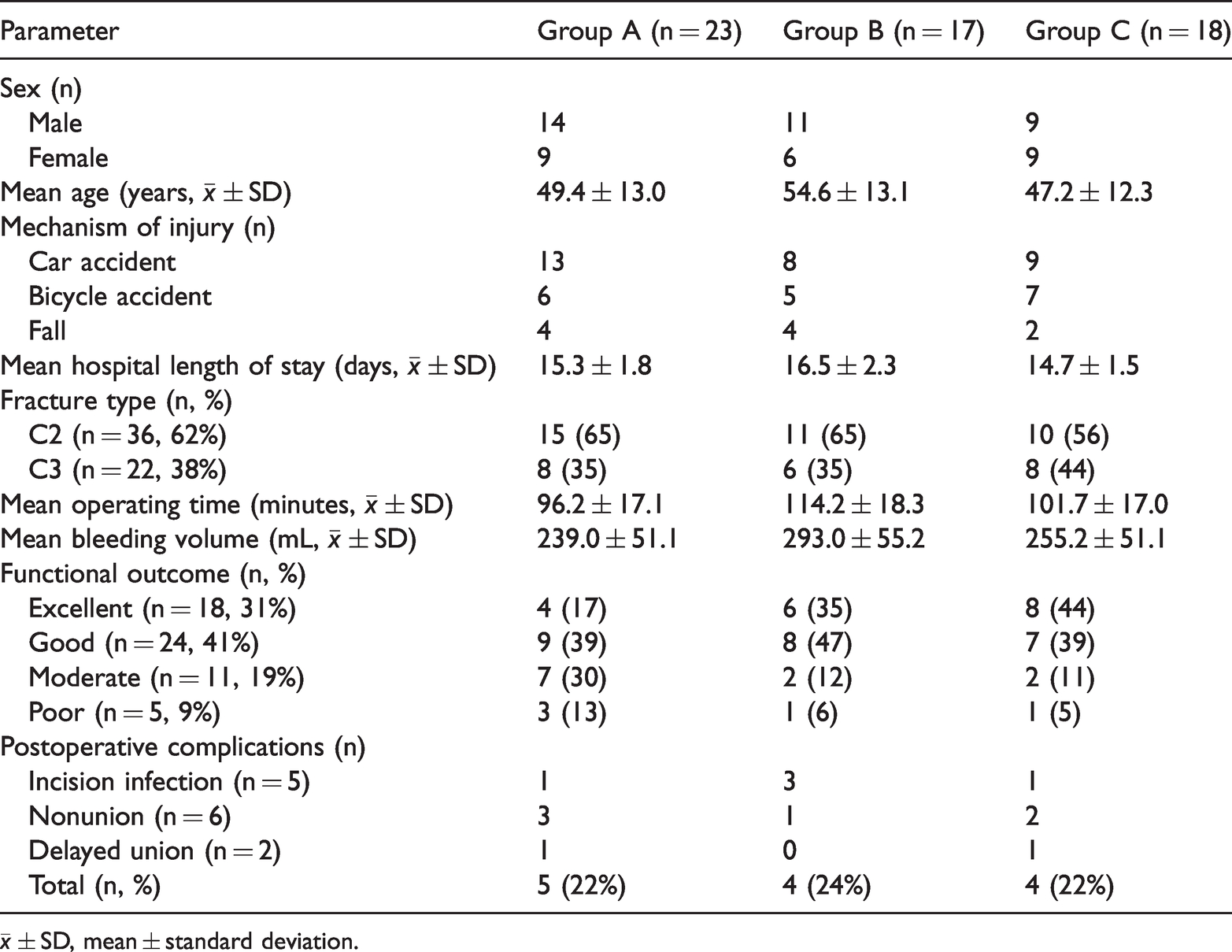
There was no significant difference in the patients’ general characteristics, such as sex and age, and LOS between the three groups. Operating time in Group A was not significantly different vs Group C, but shorter than in Group C (P = 0.002). Operating time in group B was longer than in Groups A and C, and significantly longer than in Group C (P = 0.039). Bleeding volume differed significantly between Groups A and B (P = 0.002); however, there was no difference between Groups A and C. Bleeding volume in Group B was significantly higher than in Group C (P = 0.037), while there was no significant difference between Groups A and C (Table 1).
Functional outcomes were excellent in 18 (31%) of the fractures, good in 24 (41%), moderate in 11 (19%), and poor in 5 (9%). Good-to-excellent results were achieved in 56%, 82%, and 83% of the patients in Groups A, B, and C, respectively. Outcomes in patients in Groups B and C were superior to those in Group A (P < 0.001), with no significant difference between Groups B and C. There was no significant difference in the rate of postoperative complications between the groups (Table 1).
Discussion
In this study, we investigated three fixation techniques for Müller type C2 and C3 distal femoral fractures, which are a challenging problem for orthopedic surgeons. The introduction of the Arbeitsgemeinschaft Osteosynthesefragen/Association for the Study of Internal Fixation (AO/ASIF) guidelines and the development of modern fixation devices have changed the treatment of distal femoral fractures 10 owing to the superior results using anterograde intramedullary nailing, 11 retrograde intramedullary nailing, 10 blade plates, 12 dynamic compression plates, 13 and locking compression plates. 14 Nevertheless, there are still many failures related to poor bone quality and the increased load on this distal part of the lower limb. Double plating may decrease the lever arm acting on the femoral axis, thereby decreasing the load applied on the fracture site. However, computed tomography angiography studies have demonstrated that this area is supplied by two vessels, the medial superior genicular artery and the third perforating artery to the vastus medialis muscle. 15 Potential vascular injury to the distal part of the medial thigh and femur are possible during double plating. Therefore, in this study, we used a single-incision double-plate approach to the distolateral femur to reduce the risk of vascular damage, which increases intraoperative blood loss and affects postoperative fracture healing.
Müller type C2 and C3 distal femoral fractures are intra-articular fractures, for which joint reconstruction is the first step. The knee must remain free and mobile at the surgical site; exposing the epiphyseal fracture lines is obtained with the knee bent, especially regarding the frontal lines.16,17 Stabilization on the frontal plane is generally not difficult, whereas sagittal plane stability with rotation of the condyles is much more difficult.10,18 A lateral incision at the distal end of the femur sufficiently exposes only lateral fractures, whereas exposure of medial fractures is insufficient. 19 Displaced medial comminuted fractures cannot be well reduced or are difficult to reduce, resulting in the lack of medial cortical bone support. 20 Therefore, another reconstruction plate is frequently added to increase fracture stability. Placing a lateral locking condylar plate and a medial contoured reconstruction plate requires both lateral and medial incisions. This approach requires larger surgical exposure to achieve proper placement and leads to extensive soft tissue trauma and higher infection rates.
Using a single incision to place a lateral locking condylar plate and anterior reconstruction plate reduces surgical exposure and soft tissue trauma, and medial fractures can be stabilized. This approach has the advantages of a locking plating (Single incision), and a lateral locking condylar plate and medial contoured reconstruction plate (Dual incision). Compared with a locking plating (Single incision), in this study, the operation time was similar but shorter in the lateral locking condylar plate and medial contoured reconstruction plate group (Dual incision; Group B). We saw similar but significantly less intraoperative blood loss in Group B. Furthermore, the postoperative recovery of knee joint function in patients undergoing a single-incision approach was similar to that of that in Group B, and superior to that in patients receiving a locking plating only (Single incision; Groups A and C).
There are certain limitations in this retrospective study, including the relatively small sample sizes. Additionally, there are few published articles for the dual-incision approach used in this study, and its clinical value must be explored further. We discussed only the intraoperative and postoperative healing of patients who underwent the single-incision, double-plate surgical approach, and we did not perform a mechanical analysis of this surgical approach. The mechanical stability of this surgical approach remains to be verified, but we clearly saw its advantages by comparing this approach with the two other surgical approaches.
Conclusion
Despite the small number of cases in this study, we demonstrated that the lateral locking condylar plate and anterior reconstruction plate (Single incision) approach is a useful alternative approach for complex Müller type C2 and C3 distal femoral fractures.