
Abstract
Objective:
To assess the in-hospital mortality of acute stroke and determinant factors in a teaching hospital in eastern Ethiopia.
Method:
A retrospective review of medical records of patients admitted to Hiwot Fana Specialized University Hospital was conducted. Adult patients aged 18 years and older with a diagnosis of either ischemic or hemorrhagic stroke were included. Data were analyzed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Multiple logistic regression analysis was used to identify predictors of in-hospital mortality.
Result:
A total of 112 patients with acute stroke were included in the study and 56.0% of them were of hemorrhagic stroke. The mean age was 60.32 years and 61.6% were male. The mean length of hospitalization and the mean time of presentation from symptoms onset were 4.85 days and 33.64 h, respectively. The in-hospital mortality was 36.8% for ischemic stroke and 27% for hemorrhagic stroke. Aspiration pneumonia (35.0%), cerebral edema (17%), and seizure (14.3%) were the most common complications occurring during hospitalization. Atrial fibrillation (adjusted odds ratio = 15.45, 95% confidence interval: 1.089–219.2; p = 0.043) was the independent predictor of in-hospital mortality.
Conclusion:
Hemorrhagic stroke was predominant in the study sample. One-third of patients died in the hospital and the mortality rate was slightly higher in patients with ischemic stroke. Atrial fibrillation was the predominant risk factor for hospital mortality from acute stroke. There is a need to promote cardiovascular health, early recognition, and management of risk factors, and implement coordinated stroke care services to reduce premature death from stroke.
Introduction
A stroke is a neurological deficit resulting from an acute focal injury to the central nervous system. 1 It is the leading cause of death 2 and disability in the world. 3 The majority of stroke-related mortality and disability-adjusted life years occur in low- and middle-income countries (LMICs). 4
Driven by a high prevalence of cardiovascular and metabolic risk factors coupled with limited access to primary and secondary prevention strategies, stroke continues to exert an enormous economic burden in LMICs. A systematic review that assessed the per-annum cost of stroke in LMIC identified that the highest estimated mean direct medical cost was $8424 US dollars in Nigeria and $416 in Senegal. 5 In South Africa, the average per-patient emergency department visit associated cost due to acute stroke ranges from $283,500 to $485,000 per year.6,7 A prolonged hospital stay and severe stroke underlie the highest mean direct medical cost in developing countries. 5
Stroke is a medical emergency and prompt evidence-based treatment has been shown to lower brain damage and associated complications. 8 The success of an intervention relies on the time of presentation from symptom onset, early identification of stroke types, and quick initiation of effective treatment.9–11 However, patients often present at healthcare facilities late and radiographic facilities are either not accessible or not affordable in LMIC.10–14 These issues along with limited trained personnel in stroke management and some lifesaving drugs continue to be a challenge contributing to high stroke burden and poor patient outcomes in many resource-limited countries.
In Ethiopia, a few studies have been conducted on stroke.15–19 However, no study has been conducted in the eastern region where the burden of stroke and cardiovascular disease risk factors could be different from other regions. Hence, this study aimed to assess in-hospital outcomes and associated factors in stroke patients admitted to Hiwot Fana Specialized University Hospital (HFSUH) in eastern Ethiopia
Methods
A retrospective cross-sectional study was conducted among consecutive patients with acute stroke hospitalized between October 2017 and October 2019 at HFSUH to assess in-hospital treatment outcomes of acute stroke and associated factors. HFSUH is a teaching hospital and is the largest referral center providing tertiary care for patients in eastern Ethiopia. The hospital is located in Harari Regional State, Harar Town, 526 KM east of Addis Ababa, the Capital of Ethiopia. The region had six hospitals (four government owned and two private), eight health centers, and 20 health posts. HFSUH provides inpatient and outpatient services for about 5.2 million people residing in the eastern part of the country. The hospital had major wards such as internal medicine, surgery, pediatrics, gynecology, and several clinics including tuberculosis, antiretroviral, ophthalmology, dermatology, and neurology clinic. HFSUH is not the only hospital where stroke cases were managed. The study was conducted at the neurology clinic of the hospital.
Adult patients aged 18 years and older with a diagnosis of either ischemic or hemorrhagic stroke were included. Patients with incomplete medical charts (incomplete treatments and outcomes), stroke-like symptoms, and transient ischemic attack were excluded from the study. The primary outcome of this study was in-hospital mortality from acute stroke. The effect of risk factors for in-hospital mortality such as age, gender, body temperature, alcohol use, and comorbidities such as hypertension, diabetes mellitus, heart diseases, and atrial fibrillation were assessed.
Sample size and sampling technique
All medical charts of adult patients with acute stroke treated at HFSUH during the last 2 years were eligible for the study. Based on the pre-defined eligibility criteria, medical charts of 112 confirmed acute stroke diagnoses (imaging or clinically) were consecutively included in the study.
Data collection
The data were collected using a structured data collection instrument. The content of the tool was reviewed by a senior consultant in internal medicine. The training was provided to data collectors and the tool was pre-tested on 5% of the medical chart. The patient medical chart was reviewed retrospectively and data on sociodemographic factors such as age, sex, education, mode of arrival to the hospital, length of time from symptom onset to admission, presenting symptoms, medical history, laboratory and diagnostic tests, medications given during hospitalization, in-hospital complications, length of hospital stay, discharge medications, and in-hospital treatment outcomes were collected. A formal letter of cooperation was submitted to the hospital administration and the neurology unit but written informed consent was waived by the ethics committee and was not obtained from the study participants as it was a retrospective study.
Statistical analyses
The collected clinical and sociodemographic information was entered and analyzed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were to summarize the characteristics of study participants. Bivariate analysis was done to explore factors associated with in-hospital outcomes and significant variables in bivariate analysis (p ⩽ 0.25) were selected for multivariable regression analysis to identify independent predictors of the in-hospital outcomes. A p value ⩽ 0.05 is considered significant in the multivariable regression analysis.
Result
Sociodemographic and clinical characteristics
Of the total (n = 112) patients included in the study, 56.0% had a hemorrhagic stroke. The mean (standard deviation (SD)) age was 60.32 (SD: 11.36) years and the time of presentation from symptom onset was 33.64 (SD: 15.7) h. The majority of the patients were male (61.6%) and 89.3% had no formal education. In all, 76 (67.9%) patients had hypertension, 42.9% had ischemic heart disease, and 33.9% had diabetes (Table 1). The common presenting symptoms were confusion (n = 43, 38.4%), arm paralysis (n = 59, 52.7%), altered speech (n = 50, 44.6%), headache (n = 47, 42%), and urinary incontinence (n = 88, 78.6%). In all, 25 (22.5%) patients had fecal incontinence, 43.8% had visual field defects, 10.7% had dysphagia, and 7.1% had facial palsy.
Sociodemographic and clinical characteristics of patients with acute stroke hospitalized at HFSUH, Eastern Ethiopia, 2019.

GCS, Glasgow Coma Scale; HFSUH, Hiwot Fana Specialized University Hospital; HIV, human immunodeficiency virus; TIA, transient ischemic attack.
Initial assessment and investigation
The mean (SD) systolic blood pressure and diastolic blood pressure at hospitalization were 152.58 ± 24.52 mmHg and 102.31 ± 22.97 mmHg, respectively. The mean blood glucose at hospitalization was 172.22 ± 96.49 and 28.6% of the patients had elevated blood glucose (>180 mg/dl). 34.8% had low oxygen saturation (<90%) and 39.3% had elevated body temperature (>37.5°C). Baseline imaging (computed tomographic scan) was done for all patients and serum cholesterol was measured in 46 (41.15%) patients. The mean total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglyceride were 178.76 (11.56 mg/dl), 87.35 ± 2.74, 60.69 ± 7.79, and 148.79 ± 22.87, respectively. In all patients, LDL was within optimum values (<100 mg/dl); a significant majority 38.0% of patients had high HDL (>60 mg/dl) and 33.0% had elevated (>150 mg/dl) triglyceride (Table 2).
Initial assessment and investigation in patients with acute stroke hospitalized at HFSUH, Eastern Ethiopia, 2019.

aPTT, activated partial thromboplastin time; CT, computed tomography; °C, degree Celsius; HDL, high-density lipoprotein; HFSUH, Hiwot Fana Specialized University Hospital; LDL, low-density lipoprotein; mg/dl, milligram per deciliter; mmHG, millimeter of mercury; ng/dl, nano gram per deciliter.
In-hospital complications
The most common complication during hospitalization was aspiration pneumonia (35.0%), cerebral edema (17.0%), and seizure (14.3%). Four patients experienced ventricular tachycardia, seven encountered atrial fibrillation, and four experienced intra-cerebral hemorrhage (Table 3).
In-hospital complications by stroke sub-types among patients hospitalized with acute stroke at HFSUH, Eastern Ethiopia, 2019.

HFSUH, Hiwot Fana Specialized University Hospital.
Treatment commenced during hospitalization
As a stroke unit is not available in the hospital, all patients were managed in the general medical wards. Of 49 (43.8%) patients with acute ischemic stroke, no patient received thrombolytic therapy when indicated due to the unavailability of thrombolytics at the hospital. Thus, these patients have been prescribed a loading dose of aspirin (325 mg) followed by a maintenance dose of 81 mg once daily. Of the 49 patients who were prescribed aspirin, 38.75% started within the first 24 h at the emergency department, after intracranial bleeding has been ruled out. Three (2.7%) patients were identified to have a comorbid myocardial infarction and were prescribed a loading dose of clopidogrel (300 mg) followed by a maintenance dose of 75 mg per oral daily.
Prophylaxis for deep vein thrombosis was prescribed for 40 (35.7%) patients, and all of them received unfractionated heparin (5000 mg IM daily). Of 39 (34.80%) patients who indicated oxygen therapy (i.e., O2Sat < 90%), 33% received intra-nasal oxygen. In all, 14 (12.5%) patients received antipyretic therapy (paracetamol 1000 mg every 4 h as required). Ten patients had an indication for prophylactic anticoagulant against coronary heart disease and cerebrovascular accident and thus prescribed prophylactic warfarin. Prophylactic statin (Atorvastatin 40 mg) was prescribed for all patients with ischemic stroke (Table 4).
Treatment commenced during hospitalization among patients with acute stroke admitted at HFSUH, eastern Ethiopia, 2019.

HFSUH, Hiwot Fana Specialized University Hospital.
Of the 112 patients admitted with a diagnosis of stroke, 35 (31.2%) died in the hospital and 77 (68.8%) were discharged after surviving a stroke with some form of disability. Of 35 patients who died during hospitalization, 18 had an ischemic stroke and 17 had a hemorrhagic stroke, there was no significant difference in in-hospital mortality between the two stroke subtypes (36.7% versus 27.0%, p = 0.25). The mean duration of hospital stay was 4.85 ± 3.73 days and 46 (41.1%) patients were hospitalized for 4–7 days. At discharge, 42.0% of patients have been prescribed Aspirin, 44.0% were prescribed Atorvastatin, and 8.04% were prescribed Metoprolol (Table 5).
Discharge medication and length of hospitalization among patients with acute stroke admitted at HFSUH, eastern Ethiopia, 2019.

HFSUH, Hiwot Fana Specialized University Hospital.
Predictors of in-hospital outcomes
In bivariate logistic regression analysis, age ≥65 years, pre-existing diabetes, blood glucose score between 60 and 140, body temperature between 36.5 and 37.5°C, and atrial fibrillation were significantly associated with in-hospital mortality from stroke. However, in multivariable logistic regression analysis, only atrial fibrillation remains the predicting factor of in-hospital mortality from acute stroke (adjusted odds ratio = 15.5, 95% confidence interval: 1.09–219.2; p = 0.043) (Table 6).
Factors associated with in-hospital mortality from acute stroke in hospitalized patients with acute stroke at HFSUH, eastern Ethiopia, 2019.
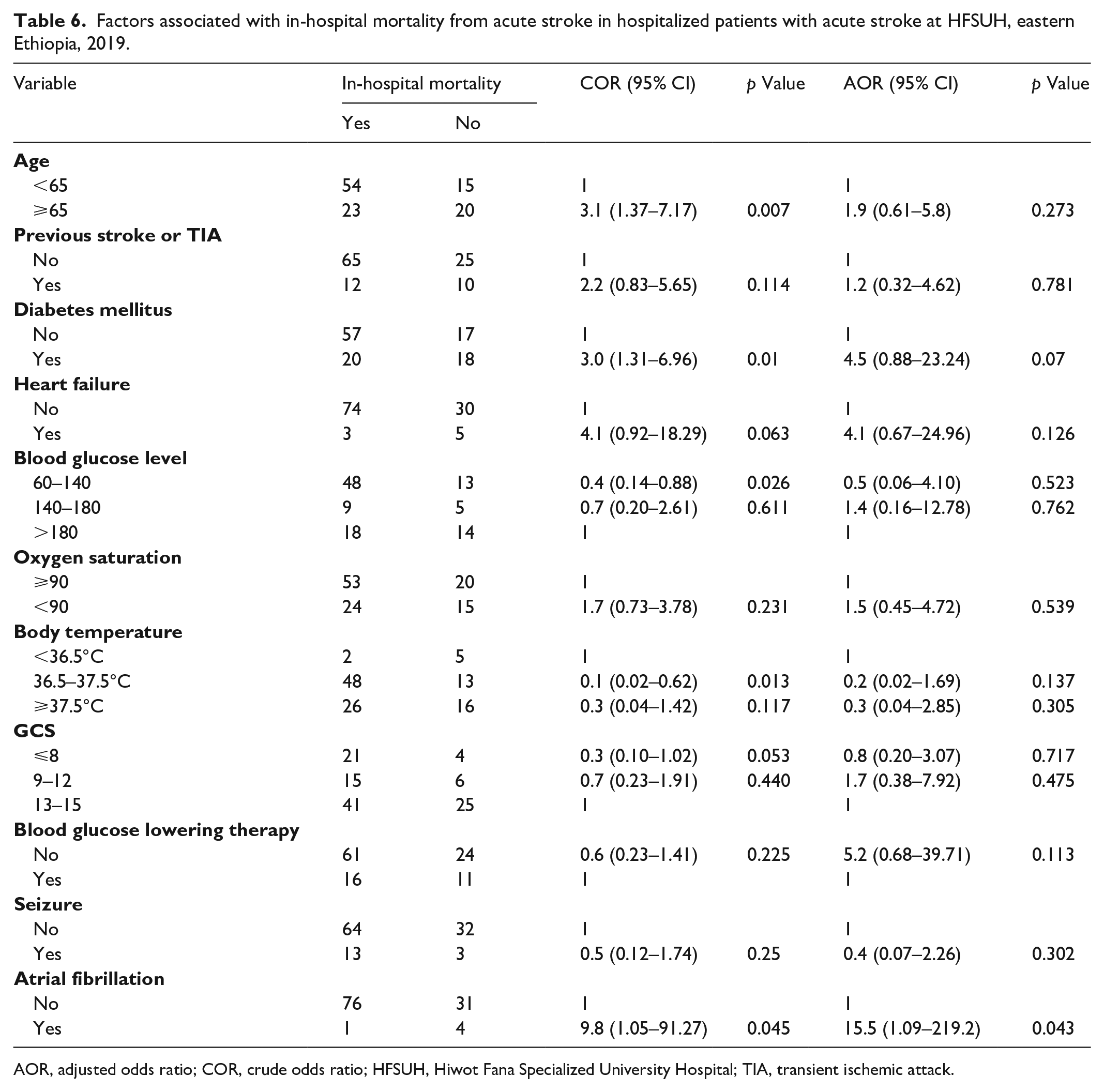
AOR, adjusted odds ratio; COR, crude odds ratio; HFSUH, Hiwot Fana Specialized University Hospital; TIA, transient ischemic attack.
Discussion
This is the first study to assess in-hospital treatment outcomes and determinant factors in patients admitted due to acute stroke in eastern Ethiopia. This study showed that the in-hospital mortality was 31.2% and 51.4% of the patients who died in the hospital were patients with ischemic stroke. It was also found that the proportion of patients who had an acute hemorrhagic stroke was higher when compared with previous studies conducted in other regions in Ethiopia 17 and some African countries.22,23 This difference could be due to the variations in the risk factors for stroke. The in-hospital case-fatality rate in this study was slightly lower than the findings of other studies.18,23 However, it was higher than the case fatality rate reported in the study conducted in Gondar, 16 Palestine (21%), 24 and Germany 25 but comparable with reports of a study conducted in Spain (31%). 26 In our study, the mean length of hospitalization was lower compared to reports from previous studies conducted in Ethiopia.16,19 The variation could be attributed to the differences in clinical characteristics like comorbidity and severity of the disease among study participants.
The average age at presentation was comparable with the findings of studies conducted in some African countries.23,27–29 This is due to the fact our arteries naturally become narrower and harder as we get older. In addition, certain medical conditions that increase the risk of stroke are common in old age. The mean time of presentation from symptom onset was 33.6 (15.7) hours. This was higher than the mean time of presentation reported in the study conducted in the capital, Addis Ababa, but lower than the study conducted in Northern Ethiopia 16 which reported 60.42 h. The discrepancy could be due to the differences in sociodemographic characteristics among study subjects.
Arterial hypertension was the most common modifiable risk factor identified in this study and this was similar to the findings reported in studies conducted in other African countries.23,28,30 In our study, diabetes mellitus was another common modifiable risk factor identified. In line with our result, diabetes was found to be the commonest risk factor in the studies conducted in Ghana 23 and Nigeria. 30 On the other hand, the prevalence of a previous history of stroke was slightly higher among our study participants, when compared with the findings of a study conducted in Addis Ababa, Ethiopia 27 but this was lower than reports from some African countries. 15
The in-hospital mortality from acute stroke was affected by several factors. In this study, comorbid diabetes, blood glucose less than 140 mg/dl, Glasgow comma scale less than 8, and atrial fibrillation were predictors of in-hospital mortality in bivariate logistic regression. However, only atrial fibrillation remains the independent predictor of in-hospital mortality from acute stroke in multivariable logistic regression analyses. This is attributed to stroke patients with atrial fibrillation having cerebrovascular risk factors and more severe stroke with more medical complications such as aspiration pneumonia and heart failure. The embolism and alteration in systemic and cerebral circulation were the proposed underlying mechanism of mortality in acute stroke patients with atrial fibrillation. 31
The management of acute stroke in LMIC is often sub-optimal10,32; and stroke unit care is not available. 10 On top of this, some lifesaving medicines such as thrombolytics are not available 10 and there is a limited number of stroke experts and trained personnel in neurology.14,32 Likewise, similar to many other developing countries, neither stroke unit nor thrombolytics is available for managing stroke patients admitted to hospitals in eastern Ethiopia.
Strength and limitation
This study was the first of its kind to offer insight into in-hospital treatment outcomes of an acute stroke at HFSUH, eastern Ethiopia. Moreover, it sheds light on factors underlying the in-hospital outcomes of study participants at the setup. The study design (being cross-sectional), being limited to a single center, inability to perform power analysis for sample size calculation, inability to assess NIHSS, and the small sample size could be the possible limitation of this study.
Conclusion
Hemorrhagic stroke was predominant in the study sample. One-third of patients died in the hospital and the mortality rate was slightly higher in patients with ischemic stroke. The majority of patients were 65 years old and younger and had at least one risk factor. Atrial fibrillation was the predominant risk factor for hospital mortality from acute stroke. Increased attention to promoting cardiovascular health, early recognition and management of risk factors, and implementing a coordinated stroke care system are needed to reduce premature death due to stroke.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221149537 – Supplemental material for In-hospital treatment outcomes of acute stroke and determinant factors in a teaching hospital in eastern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221149537 for In-hospital treatment outcomes of acute stroke and determinant factors in a teaching hospital in eastern Ethiopia by Fuad Adem, Behar Mohammed and Shambel Nigussie in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge the hospital and workers at the medical record-keeping office for their cooperation.
Authors’ contributions
Fuad Adem was involved in the conception and design of the study, developed data collection tools, supervised data collection, analyzed data, and draft the original document and the manuscript. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
The study was approved by the Institutional Research Ethics Review Committee (IRERC) of Haramaya University.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was waived by the ethics committee (retrospective chart review) and not obtained from the study participants as it was a retrospective study.
Trial registration
Not applicable.
Data availability
The raw data used for this study were included in the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.