
Abstract
Oral teratoma is a congenital neoplastic lesion with an incidence of 2%–9% of all teratomas. It comprises variable amounts of all three germ cell layers. The lesion is graded on histology depending upon the presence of immature components. The most common sites of presentation are the sacrococcygeal area and head and neck with slight female predominance. Our report is based on a case that was received for histopathological evaluation. It consisted of a 20-week fetus with a huge mass protruding from oral orifice measuring 10.8 × 6.7 cm. Histological examination of the tumor revealed immature teratoma—oropharynx.
Introduction
Oral teratoma or epignathus is a congenital neoplastic lesion comprising variable amounts of all three germ cell layers; ectoderm, endoderm, and mesoderm. 1 These lesions are graded on histology depending upon the presence of immature components, usually in the form of neuroepithelial tissue.1,2 Most common sites of presentation are sacrococcygeal and head and neck2,3 with slight female predominance. 2 The risk of mortality rises if diagnosed in the fetal or neonatal period which is purely related to the site of the lesion and compromise of various other important functions. However, recent advancements in prenatal imaging and techniques provide us with a great opportunity for diagnosis and assessment of potential risks associated. The incidence of a congenital oral teratoma (epignathus) is 2%–9% of all teratomas. 3
Case report
We report an interesting case of a male fetus which was initially discovered on radiology (ultrasonographic) at 20 weeks with facial characteristics that were not clearly discernible. A huge lump protruding from face measuring 10.8 × 6.7 cm was observed. On further radiological examination, it was ascertained that the lump was originating from mouth. Fetus and other products of conception were sent to the histopathology department for determination of exact underlying disease. Gross examination revealed a gray to tan white, firm, and multilobulated lesion with measurements stated above (Figure 1). Serial slicing of the lesion showed gray white surface with cystic spaces. It originated from soft palate in the midline. Histological examination of the tumor revealed a lesion which comprised varying proportions of bone, skin adnexa, hair, and glandular tissue. Immature component was identified in the form of neural tissue (Figures 2–4). The case was signed off as immature teratoma—oropharynx.

Gross picture showing a 20-week fetus with large oral immature teratoma.
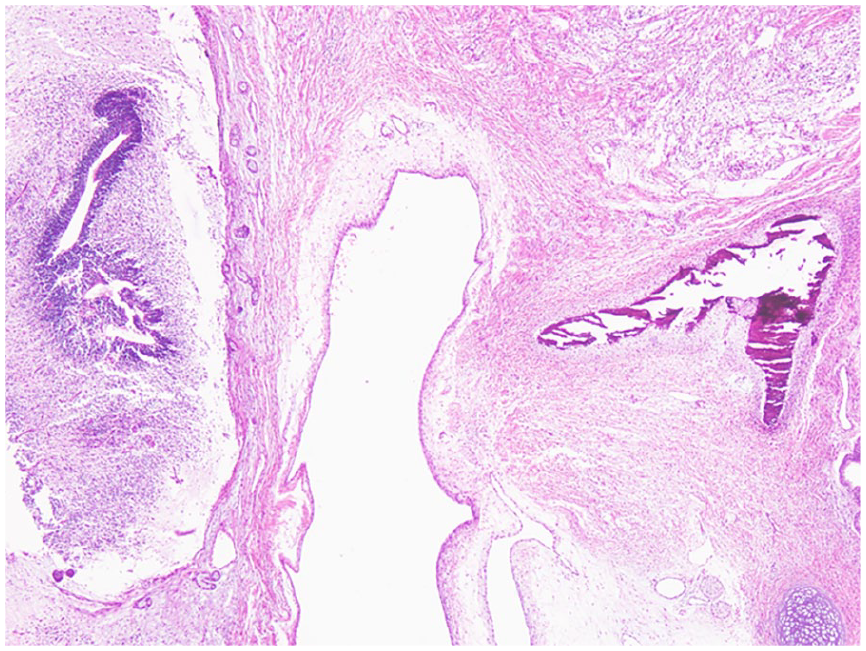
Immature teratoma exhibiting various components as immature neural tissue, colonic epithelium, and bone.

Photomicrograph showing various components of immature teratoma.
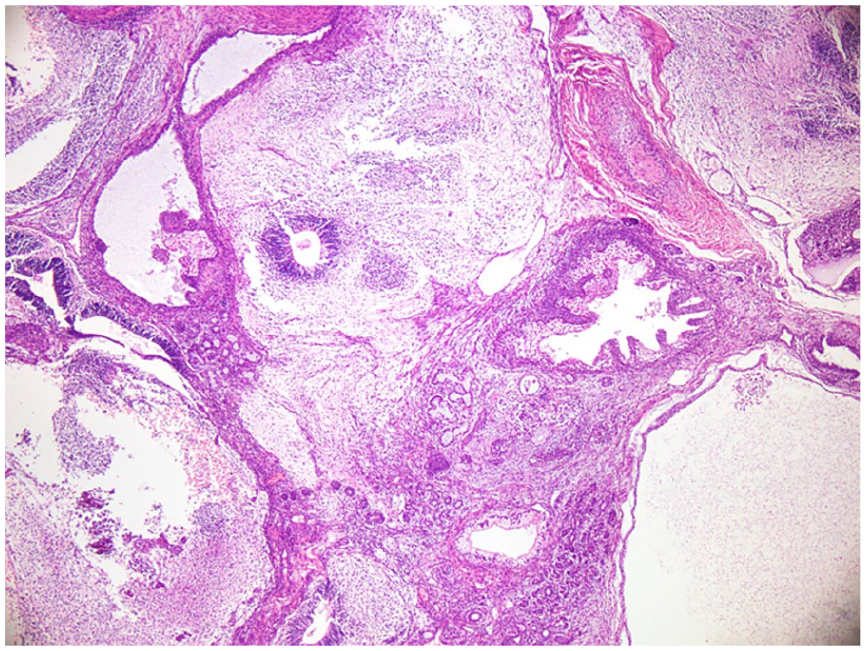
Immature teratoma exhibiting glands, cystic components, and immature neural tissue.
Discussion
Teratomas are tumors consisting of multiple tissue types that are not natural to the site of their origin. 4 The occurrence of a congenital oral teratoma (epignathus) is 2%–9% of all teratomas. 3 Fetal teratomas are rare, with a reported frequency of 1:4000 live births.4,5 Depending on the presence or absence of immature components, these can be benign or malignant.1,4,6 Minor female predominance has been observed. 4 The sacrococcygeal area of the fetus or infant is usually involved.6,7 Common sites of involvement for mature teratomas in head and neck region are maxillary antrum, nasal cavity or nasopharynx, and thyroid gland. These lesions manifest as facial deformities during radiological examinations.4,8,9 Teratomas of the palate are rare. 3
Teratomas are germ cell tumors that are made up of varying quantities of all three germ cell tissues. Their grading is histology based.2,8 Skin, skin appendages, bone, hair, smooth and skeletal muscle, cartilage, respiratory, and gastrointestinal epithelium are frequently encountered.3,4,7 Immature components, like their counterparts in the gonads or extragonadal regions, are typically in the form of immature neural tissue.1,2,4,10 Rarely other somatic malignancies have also been reported originating within these lesions. 10
The pathogenesis of teratoma is unresolved however there are multiple proposed theories. One of the suggested theories is that these tumors are derived from sequestered pluripotent stem cells, isolated during embryologic development. Still, another proposal1–16 is that these tumors could be derived from embryonic tissue foci that originally failed to migrate appropriately during development.2,5 The precise distribution according to anatomical sites is not fully coherent due to limited data. However, oral cavity, oropharynx, nasopharyngeal, foramen cecum, ear, nasal septum, skull base, parotid gland, and thyroid gland have been frequently reported.2,3
Prenatal diagnostic analysis is especially difficult. Ultrasonographic (USG) diagnosis is found to be perfect in detection even in the initial stages,2,7,9,12,13 as was obvious in our case also. Most cases continue to occur in the second and third trimesters or we can also assume that these lesions grow later in pregnancy.
On USG with an anterior or bidirectional plane, an organoid face mass with a solid and cystic component is usually found.2,12,13 As the mass protrudes from the fetus face or specifically mouth, it can cause hyperextension of the head depending upon the size of the tumor. Magnetic resonance imaging has also been a valued diagnostic necessity, allowing for a better understanding of the location, size, and interaction with nearby structures. Prenatal increases in alpha-fetoprotein concentrations have shown strong association. 2 In head and neck teratomas, fetal karyotyping can play a valuable tool in assessment of outcome. Fetoscopy is another new current approach that may be employed to analyze the whole lesion. Exclusion of intracranial extension is a significant part of preoperative management.2,9
Teratomas that develop in fetal phase are frequently accompanied by polyhydramnios.2,4,8,14 After birth, depending upon the size and location of the tumor, it can pose feeding and respiratory challenges. 4 Added associations are cleft palate, cystic hygroma, multifocal teratomas, bifid tongues and nostrils, Dandy-Walker deformity, ventricular septal defect, pulmonary hypoplasia, and nerve palsy. Head and neck teratomas are usually benign and have a better prognosis after complete resection. However, failure to diagnose or removal poses complications during delivery and further difficulties in neonatal period. 4
Differential diagnoses include cleft lip and palate, hemangioma, cystic hygroma, branchial cleft cyst, congenital goiter, lingual thyroid tumors, cervical neuroblastoma, soft tissue sarcoma, anterior encephalomyelocele, dermoid cyst, and heterotopic gastrointestinal cyst. The presence of bone, skin adnexa, hair, glandular tissue, and immature neural tissue in our case brings us to the diagnosis of immature teratoma. Although vascular component, multiple cystic areas, thyroid tissue and gastric tissue (as mentioned in the differential diagnosis entities) can be present separately in so many other conditions; however, the combined presence of all the elements together, as mentioned above, successfully rules out any other possibility.
Small benign teratomas have an excellent prognosis, and recurrence is uncommon. However, larger lesion poses difficulties for complete excision. Being at an important location main challenges are poor fetal swallowing, airway obstruction, and feeding difficulties at birth. Delayed diagnosis and treatment also increase the likelihood of malignant transformation. Only potential alternatives are endotracheal tube installation and tracheostomy. To enhance the chances of survival, intrapartum intubation (ex utero intrapartum treatment procedure) or resection of the tumor at the time of the cesarean section, before cutting the umbilical cord (operation on placental support) has improved benefits. However, despite all efforts, survival rates are low. 15
Conclusion
Few clinical assumptions that can be made, teratomas are rare congenital tumors with complex etiology. Prenatal diagnosis is possible in early pregnancy which can aid in risk stratification and options for treatments. Having said this, it is important to mention here that there was no antenatal history available in our case. There was no information on the mode of delivery, actions taken at birth, and any other tests if performed during pregnancy. This is crucial, as having this data during in utero phase can identify potential candidates who can be benefited by available medical or surgical options. All teratomas should have a prenatal karyotype and a thorough search for related anomalies.
The prenatal diagnosis of head and neck teratoma carries a serious threat. Most of such diagnosed antenatal cases suffer fetal demise or emergency surgery. After birth, these fetuses have airway obstruction and feeding difficulties. These complications could be averted by early detection and safe treatment in utero.
Footnotes
Acknowledgements
We acknowledge all the staff of the histopathology department for their support.
Author contributions
S.A. concept; design; definition of intellectual content; literature search; data acquisition; data analysis; manuscript preparation; manuscript editing; manuscript review; guarantor. H.F.S. literature search; manuscript preparation; manuscript editing; manuscript review; guarantor. S.A. concept; definition of intellectual content; literature search; data analysis; manuscript preparation; manuscript editing; manuscript review; guarantor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series
Ethical committee
The case report did not require review from ethical committee.
Consent
The consent was waivered as reporting a case does not pose risk to the subject and the patient information is kept confidential.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Grant number
The case report has no grants.