
Abstract
Yolk sac tumors (YSTs) of the ovary are the second most common primitive germ cell tumors accounting for 20% of malignant ovarian germ cell tumors. They are derived from primitive germ cells of the embryonic gonad and can undergo germinomatous or embryonic differentiation. They commonly affect women in the reproductive age group but have a favorable prognosis due to chemosensitivity. This is a case of pure YST of ovary in a nulliparous 25-year-old woman with a past history of endometriotic cysts.
Introduction
Yolk sac tumors (YSTs) of the ovary are primitive germ cell tumors commonly occurring in the second and third decades of life. These tumors account for 20% of malignant ovarian germ cell tumors and are the second most common germ cell neoplasm after dysgerminoma.1,2 YSTs are often associated with elevated serum alpha fetoprotein (AFP) and clinically present as abdominal enlargement or pain. These tumors usually have a favorable prognosis due to chemosensitivity, the challenge being ensuring disease control without compromising fertility in adolescent and young women. Here, we report a case of pure yolk sac ovarian tumor in a 25-year-old woman who presented with lower abdominal pain with a past history of endometriotic cysts.
Case history
A 25-year-old nulliparous woman, wanting to conceive, presented with lower abdominal and back pain since 2 weeks, not associated with menses. The pain increased after passing urine, but there were no symptoms of urinary tract infection. She also complained of nausea since 2 weeks and one episode of fever 1 day prior. She gave history of regular menstrual cycles with history of passage of clots, dysmenorrhea, and heavy menstrual bleeding. She had a history of bilateral endometriotic ovarian cysts since 2 years for which she took progesterone for 1 year.
A contrast-enhanced computed tomography scan of the abdomen and pelvis revealed a relatively well-defined heterogeneously enhancing lesion epicentered in the left adnexa measuring 9.4 × 8.5 × 6.8 cm3. The left ovary could not be visualized separately. Anteriorly, fat planes were maintained with the rectus muscle; however, posteriorly and left superolaterally there was focal loss of fat planes with the adjacent sigmoid colon and distal descending colon as shown in Figure 1.
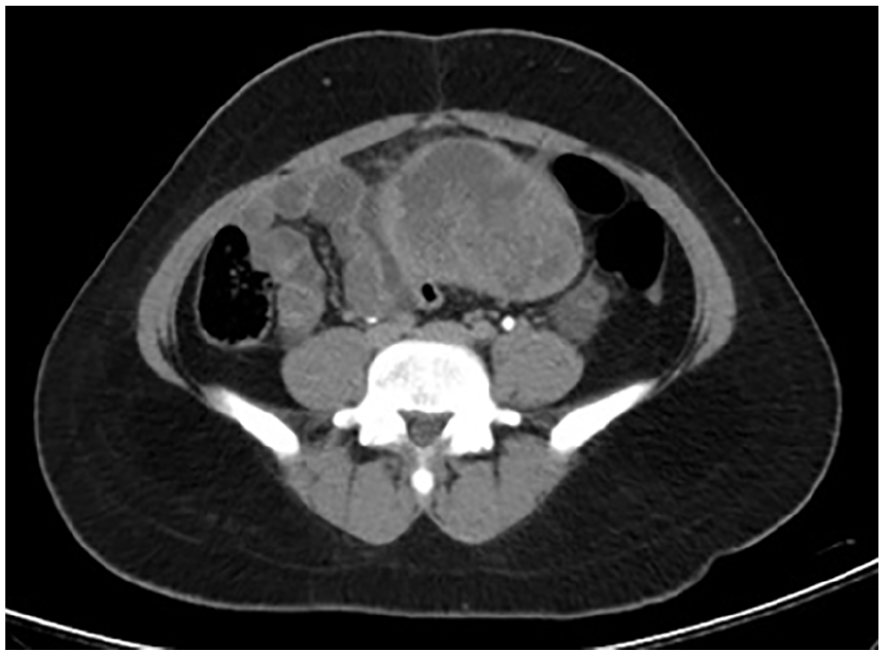
Contrast-enhanced computed tomography scan showing a left adnexal lesion.
Serum biochemical investigations revealed elevated lactate dehydrogenase levels of 548 U/L (normally 125–220 U/L), mildly elevated Ca 125 levels of 48.3 U/mL (normally less than 35 U/mL) and AFP levels of >60,500 ng/mL (normally 0–8.5 ng/mL in non-pregnant women). Thus, a clinical diagnosis of germ cell tumor of the left ovary was made and the patient underwent a fertility sparing surgery involving right ovary cryopreservation along with left (unilateral) adnexectomy with infracolic omentectomy.
On gross pathologic examination, the left adnexectomy specimen weighed 431 g and the left ovary measured 11.5 × 11.0 × 6.0 cm3. The external surface was smooth and bosselated with an intact capsule. Cut section revealed a yellow white solid-cystic tumor (predominantly solid) showing areas of hemorrhage and necrosis as shown in Figure 2.

Cut section of left ovary.
Microscopically, the tumor showed a microcystic pattern and endodermal sinus pattern with Schiller–Duval bodies and scattered tumor cells showing hyaline globules (Figure 3). The omentum was unremarkable. A provisional diagnosis of YST with the possibility of mixed germ cell components was given. Extensive sectioning was done. Immuno histochemistry was performed for CD117, CD30, and AFP out of which only AFP was positive (Figure 3 insert), thus, confirming a diagnosis of pure YST and ruling out other mixed germ cell components. The tumor was staged as Ia since the tumor was limited to one ovary with an intact capsule along with absence of tumor on the surface of the ovary and negative peritoneal washings.

Schiller-Duval body (H&E 10× magnification). Insert shows AFP IHC staining at 20× magnification.
Postoperatively (day 26 post-op), the AFP levels were still elevated (13,668 ng/mL) and so the patient was planned for three cycles of adjuvant chemotherapy with bleomycin, etoposide, and cisplatin (BEP) regimen at 21-day intervals over the next 3 months. Prior to initiating chemotherapy, serum AFP levels were 3996 ng/mL and subsequently decreased to 1110 ng/mL after the first cycle. Two cycles of chemotherapy have been administered so far, and the patient has no further complaints.
Discussion
Ovarian germinal neoplasms tend to occur in younger aged women and are diagnosed at earlier stages of the disease. These tumors are associated with the presence of specific tumor markers that permit diagnosis with quasi-certainty even before histological confirmation, thus allowing for fertility sparing surgeries rather than radical ones. 3
Malignant ovarian germ cell tumors constitute around 3%–5% of all ovarian malignancies.4,5 YSTs of the ovary previously referred to as endodermal sinus tumors, are rare and highly malignant ovarian germ cell tumors occurring primarily in children and young women, representing about 1% of all ovarian malignancies and 20% of malignant ovarian germ cell tumors. 6 Among all subtypes of germ cell tumors, YSTs are highly malignant and have the worse prognosis. 6 Since these tumors primarily affect women of child bearing ages, fertility preservation becomes an important challenge in the treatment of these tumors. Therefore, accurate diagnosis, staging and treatment of these tumors becomes imperative. 6
YST was first described in 1939 with a proposed mesonephroid origin. However, around 20 years later, these tumors were reclassified and designated as endodermal sinus tumors with an embryological origin. Later on, because of the similarity of these tumors with extraembryonal yolk sac and vitelline structures, they were named YSTs. 7
Clinically, the most common symptom is abdominal pain. Other symptoms include presence of an abdominal or pelvic mass with abdominal enlargement. Few patients can present with endocrine manifestations as a direct consequence of hormone secretion by the tumor. The duration of symptoms on average ranges from 2 to 4 weeks. 6
Serum AFP is a useful biomarker for the diagnosis and management of YSTs which is also used to check for complete remission or recurrence. Decreasing ration of serum AFP postoperatively is an effective indicator in determining whether or not residual disease remains after surgery. An increased CA-125 is also not infrequent in YSTs. 6
These tumors are derived from primitive germ cells of the embryonic gonad and can undergo germinomatous or embryonic differentiation. 6 Around 75% of cases have chromosome 12 abnormality, mostly isochrome 12p. 1 A retrospective study carried out by Hodroj et al. in collaboration with EURACAN and EORTC SPECTA also found potentially targetable oncogenic mutations in 33.3% of all patients in KRAS, KIT, and ARID1A. 8
Grossly, YSTs tend to be unilateral with an average size of 15 cm showing solid cystic areas on cut section with a friable, hemorrhagic, and necrotic appearance.
Microscopically, YSTs show multiple patterns, most common of which is reticular/microcystic pattern. Other patterns include endodermal sinus pattern (with Schiller–Duval bodies), papillary pattern, solid pattern, festoon pattern, and glandular pattern. Less commonly encountered patterns include polyvesicular-vitelline, parital, mesenchyme-like, and hepatoid patterns.1,9 The tumor cells usually exhibit atypia of varying degree with clear cytoplasm and hyaline globules. Immunohistochemical studies show positivity for SALL4, AFP, LIN28, glypican-3, and ZBTB16. Cases with intestinal type pattern can show positivity for CDX2, while those with hepatoid pattern and foregut/respiratory pattern show positivity for Hep Par-1 and TTF1, respectively. 1
The standard treatment of malignant ovarian germ cell tumors is fertility preserving surgery and three to four cycles of combination chemotherapy with BEP. Cisplatin containing chemotherapy is a prognostic factor in which BEP regimen is more effective than others. Currently, standard therapy involves three courses of BEP, while four courses are recommended in cases of bulky residual surgery postoperatively. 10
As per a study conducted by De La Motte Rouge et al., it was shown that a high cure rate is achievable even in patients presenting with advanced disease even though the prognosis is worse as compared to early stage tumors. Compared with other regimens, BEP appears to be the best option for active first-line therapy for primary, metastatic, or recurrent disease. 7
Prognostically, tumors of stages I or II have a 5-year survival rate of >95%, whereas for stages III and IV, the survival rates drop to 70% and 50%, respectively. Other reported prognostic factors include the presence of residual tumor, ascites, cisplatin containing chemotherapy in advanced cases, BEP therapy, AFP half-life, and time to serum AFP normalization.10–12
To conclude, since YST primarily affect women of child bearing ages, accurate diagnosis, staging, and treatment of these tumors becomes imperative in view of fertility preservation which in some cases can be a challenge.
Footnotes
Acknowledgements
The authors thank all the physicians, pathology technicians, and staff who have worked very hard to take care of this patient.
Authors’ note
On behalf of all the contributors, I will act as guarantor and will correspond with the journal from this point onward.
Author contributions
All authors contributed to conceptualization, writing, and critical review of this case report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The photographs are completely unidentified and personal details are not mentioned in the text. The authors are accountable for all aspects of the work and for ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Our institution does not require ethical approval for reporting case reports.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.