
Abstract
The objective of this case report is to present the use of tenting screw bone augmentation technique for the rehabilitation of narrow horizontally deficient mandibular ridges and to evaluate the feasibility and outcomes of this approach in achieving sufficient bone volume for successful implant placement and Osseointegration. A 34-year-old woman with no significant medical history presented with bilaterally missing teeth in the lower arch. A comprehensive treatment plan was developed through assessment and Cone Beam Computed Tomography (CBCT) imaging to evaluate the ridge dimensions and plan the treatment accordingly accurately. The tenting screw technique, utilizing autogenous/autologous+allograft materials, was chosen for horizontal ridge augmentation. Bone augmentations were performed simultaneously bilaterally using tenting screws. After a 20-week healing period, CBCT scans revealed favorable bone regeneration with adequate width for successful implant placements. This case report demonstrates the potential of tenting screw bone augmentation in effectively rehabilitating mandibular ridges and achieving optimal dental implant outcomes. Further research is needed to validate these findings and assess the long-term stability and success of this technique.
Introduction
Dental implant rehabilitation of partially or completely edentulous patients with a resorbed mandible presents significant challenges for both the prosthodontist and surgeon. Common problems include insufficient retention of the lower denture, intolerance to mucosal loading, pain, difficulties with eating and speech, loss of soft-tissue support, and altered facial appearance.1,2
An osseous ridge augmentation course is frequently required for reliable implant therapy in cases with low bone volume. Sufficient bone volume is essential for endo-osseous dental implants to successfully osseo-integrate and be retained over the long term.1,2 The tenting screw technique, along with its modifications such as cortical autogenous and tenting screw, has been advocated for initial reconstruction and subsequent regeneration of maxillofacial defects. Studies have shown the effectiveness of these techniques in augmenting bone.3,4
Although autogenous bone grafts are considered the best materials for augmentation, iliac bone grafts, in particular, are subject to significant resorption.5–10 Currently, bone augmentation can be achieved using various biomaterials. 11 These materials can be categorized according to their source of origin and intended recipient, including allogeneic bone grafts or allografts (obtained from a genetically distinct individual of the same species), xenogeneic bone grafts or xenografts (obtained from a different species), and alloplastic bone substitutes (materials created synthetically). 12 Autogenous bone graft or autograft refers to bone originating from the same patient and can be harvested from intra-oral sites (symphysis, retromolar pad area, anterior mandibular ramus, tori, exostoses) or extra-oral sites (iliac bone, the calvarium, and the tibia). 13
The choice of the autogenous donor site for bone grafts depends on the quantity of bone required at the recipient site and the biological qualities of the donor’s bone. The quantity of bone needed is the primary factor in selecting the donor site. 14 For ridge augmentation in totally edentulous patients with extensive bone resorption, an extra-oral donor site like the posterior iliac crest is often used to produce large volumes of bone. In contrast, intraoral donor sites like the mandibular symphysis are suitable for partially edentulous patients with smaller bone defects, as they can provide modest bone volumes. 15
Depending on the indication and the required amount of graft, autogenous bone may be employed in a variety of ways, including in the form of particles (either alone or combined with a bone-substitute material), encased in titanium meshes, screws, or membranes, or as a block graft. 15 Cone Beam Computed Tomography (CBCT) is the preferred radiographic assessment method for reliable evaluation before and after augmentation treatments. It is important to discuss alternatives to augmentation surgery, such as the use of tilted or angulated implants, narrow implants, zygomatic implants, short implants, or non-implant-supported prostheses, which may eliminate the need for augmentation, with the patient.16,17
By employing the tenting screw technique, the prosthodontist and surgeon aimed to address the challenges posed by the resorbed mandibular ridge. This technique offered a predictable and reliable method for ridge reconstruction, which was crucial for successful dental implant placement. Tenting screw technique provided the necessary bone augmentation and stabilization required to support the dental implants and restore the patient’s oral function and aesthetics. Therefore, based on the reported effectiveness of tenting screw technique in augmenting bone and the advantages of autogenous bone grafts, it was deemed a suitable approach for the presented case of a partially resorbed mandibular ridge.
Case report
A 34-year-old woman with no significant medical history presented at a dental clinic for a comprehensive prosthodontic consultation. Her chief complaint was the desire to replace her missing lower molars bilaterally to restore both esthetics and function. The patient denied any history of tobacco, pan, betel nut, or drug use, and had no known allergies to drugs or materials. She had lost teeth 36, 37, 46, and 47 in her early twenties due to caries and did not undergo any socket preservation procedures at the time of extractions.
During the consultation, the patient was presented with different restoration options for replacing her missing teeth, including a removable partial denture or implant-supported fixed restoration. She expressed a preference for fixed prosthetics using dental implants rather than a removable partial denture. To further assess the bone quality and quantity, a CBCT scan was recommended.
Upon clinical examination, it was observed that the patient had a narrow ridge bilaterally, with some vertical atrophy on the left side. An orthopantomogram revealed missing teeth 36, 37, 46, and 47 (Figure 1). The CBCT scan showed that the ridges were too narrow for implant placement, measuring 4.2 mm on the right and 2.4 mm on the left side at the crestal part of the alveolar bone in the lower posterior mandible (Figure 2(a) and 2(b)).
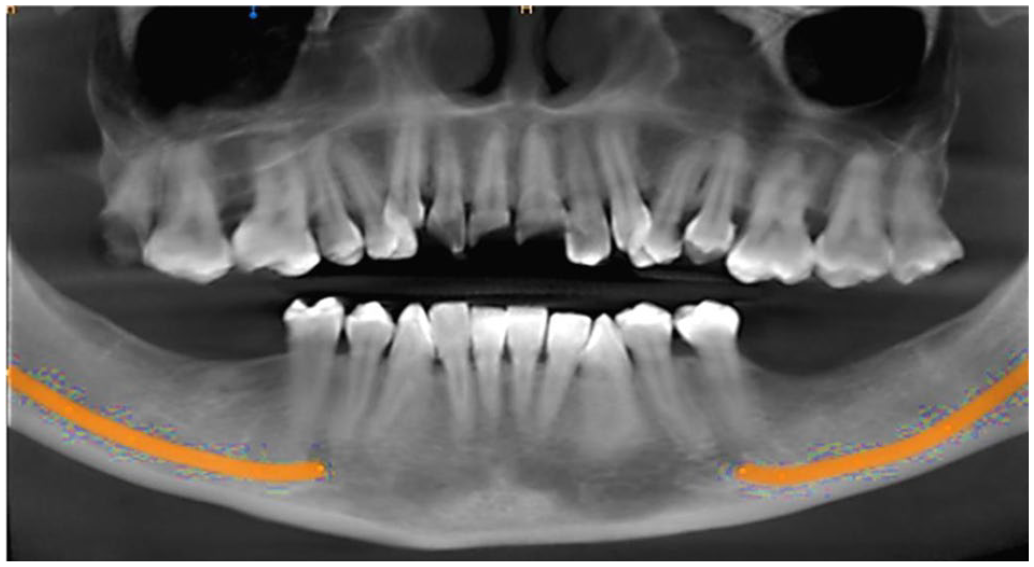
Pre-operative panoramic view.

(a) Preoperative Cone Beam Computed Tomography (CBCT) cross-section right side first molar region with 4.2 mm width. (b) Preoperative CBCT cross section left side first molar region with 2.4 mm width.
Based on a thorough assessment of the patient’s chief complaints, dental history, and clinical and CBCT examinations, guided bone regeneration (GBR) with tenting screws was determined to be the appropriate treatment approach. Autograft and allograft materials were planned for use bilaterally. The patient was provided with written informed consent for the proposed treatment.
Presurgical management
After the initial surgical and prosthodontic consultation, the patient underwent phase I periodontal therapy as part of the treatment plan. This phase included oral hygiene instructions and prophylaxis to improve the patient’s overall oral health. The goal of this phase was to establish a healthy periodontal environment before proceeding with surgical treatment.
Following the phase I therapy, a 6-week periodontal re-evaluation was conducted to assess the patient’s progress. The re-evaluation showed significant improvements in the patient’s oral hygiene, indicating that she had diligently followed the oral hygiene instructions provided. The overall periodontal health had improved, and it was determined that the patient was ready to move forward with the surgical phase of the treatment plan.
The successful completion of phase I periodontal therapy ensured that the patient’s oral health was optimized, creating a favorable environment for the upcoming surgical procedures. This preparatory phase played a crucial role in ensuring the long-term success of the planned implant-supported fixed restoration. With the patient’s improved oral hygiene and periodontal health, the subsequent surgical treatment could proceed with a reduced risk of complications and better overall outcomes.
Surgical procedure and postoperative instructions
One gram of co-amoxiclav was used to pre-medicate the patient, 18 and 30 s of preoperative chlorhexidine rinse was given before the procedure. Following the administration of local anesthesia, the surgical operation started with the creation of an incision on the left side of the mandible at the surgical site, running from the distal papilla of the first premolar up to the anterior border of the ramus. A full-thickness mucoperiosteal flap was elevated to expose the underlying tissues.
Using a fissure bur, a cortical osteotomy to harvest cortical bone of size 12 mm by 8 mm from the donor site (ramus/buccal shelf) was done, as depicted in Figures 3 and 4. The block was removed with the help of chisels. To minimize bleeding at the donor site, a gelatin sponge was applied. A horizontal ridge augmentation was performed by securing the block bone with a 1.5 × 10 mm tenting screw. The spaces within the augmentation were filled with 0.2cc of allograft material (Renew Oss tm, 80% cortical 20% cancellous mixture with particle size 0.2 mm to 1 mm), and a resorbable collagen membrane (Lyoplant (Braum tm) bovine collagen) was placed over the augmentation site. 19 The surgical site was then sutured without tension with 4-0 polypropylene (Prolene) sutures after periosteal release.

3D Cone Beam Computed Tomography of left side after buccal bone block harvest (marked with yellow color arrowheads).

Cross section of left side Cone Beam Computed Tomography after buccal bone block harvest (marked with yellow color arrowheads).
On the right side, an incision was made at the surgical site similarly, after the administration of local anesthesia. A cortico-cancellous bone graft was harvested from the ramal/buccal shelf area of the mandible, as depicted in Figures 5 and 6, which was then ground using the bone mill. A full-thickness flap was reflected, and a 2 × 9 mm tenting screw was inserted. A mixture of 1cc cortico-cancellous bone chips autograft and 1cc particulate cortico-cancellous allograft was placed at the augmentation site. 19 A resorbable collagen membrane (Lyoplant (Braum tm) bovine collagen) was then applied and fixated with resorbable polygalactin (Vicryl 4-0) sutures, and the surgical site was sutured with 4-0 polypropylene (Prolene) without tension. Saline solution and 0.12% chlorhexidine rinse were used to irrigate the site.

3D Cone Beam Computed Tomography of right side after buccal bone block harvest (marked with black color arrowheads).

Cross section of right side Cone Beam Computed Tomography after buccal bone block harvest (marked with yellow color arrowheads).
The patient was instructed to use an extraoral cold pack sporadically for the first 24 h after surgery to lessen edema. The patient was administered 400 mg of ibuprofen every 6 h for pain relief, 1 g of co-amoxiclav twice a day for 7 days, and a 0.12% chlorhexidine rinse for 30 s twice daily for 14 days. Detailed postoperative instructions were given, which included avoiding mastication for 6 to 8 weeks and brushing or exerting pressure on the surgical region for 4 weeks.
Follow-up appointments
The patient underwent regular follow-up appointments at 1, 2, 4, 6 (for suture removal), 8, 12, 16, and 20 weeks postoperatively. Bone exposure was seen on the block graft (left side) in the 8th week. The exposed bone (2 mm) was removed with SS round bur and mucosa left to heal. Complete coverage was seen on the 12th week. After the 20-week follow-up, a second CBCT scan was taken to assess the outcome of the GBR procedure (Figure 7). To allow accurate reproducibility of measurements on the CBCT, the upper first molar mesio-palatal cusp tip was taken as an anteroposterior reference point. Upon interpretation of the CBCT images, it was determined that the GBR had successfully provided sufficient horizontal ridge augmentation. In this case, it was attempted to alter the width of the ridge (reduction or gain) not the height of the ridge. However, the superior part of the inferior alveolar canal was taken as a reference for height in this case.

Post-operative panoramic view.
On the right side, the ridge exhibited a width of 9.0 mm, as depicted in (Figure 8(a)). On the left side, the GBR resulted in a ridge width of 7.7 mm, as shown in (Figure 8(b)). Based on these measurements, it was concluded that the ridge dimensions were suitable for proceeding with implant placement.

(a) Post-operative Cone Beam Computed Tomography (CBCT) cross-section right first molar region with 9.00 mm width. (b) Post-operative CBCT cross-section left first molar region with 7.7 mm width.
Subsequently, the tenting screws that had been used during the GBR procedure were removed once the healing period was completed at 20 weeks. After a period of 1 week from screw removal, 2 implants (Megagen AnyOne, South Korea) with standard diameters of 4.5 mm and 4 mm and heights of 8.5 and 10 mm were successfully placed on the right in the 46 and 47 places (Figure 9), while 2 implants (Megagen AnyOne, South Korea) of diameter 4.5 mm and height of 10 mm were placed on the left side (Figure 10).

Implant placement on the right side of lower arch.

Implant placement on the left side of lower arch.
The successful GBR procedure, as evidenced by the favorable ridge dimensions on the CBCT scans, provided a solid foundation for the subsequent implant placement. This outcome was crucial in ensuring the long-term stability and success of the implant-supported fixed restoration. The step-by-step approach taken in this case, including the GBR and subsequent implant placement, contributed to achieving the patient’s desired esthetics and functional restoration.
Discussion
In the past, a variety of grafting methods have been suggested to accomplish a reliable and successful restoration of alveolar defects. 20 The tenting screw approach is one such method that has been researched in several of studies.4,21,22 A tent-pole effect was applied in a study by Rocchietta et al., 23 and it was discovered that autogenous block grafts produced statistically larger bone volume in the enhanced region than autogenous particle grafts.
Non-autogenous bone grafts can be just as successful and advantageous as autogenous bone grafts, according to the scientific literature on bone augmentation. Based on these preliminary findings,24–27 it is possible that new types of particulate bone grafts might be employed as an alternative to autogenous block bone grafts. The fact that these concentrates are made from autologous sources may be responsible for the lack of clinical problems and the beneficial effects on wound healing. 28 These results suggest that in terms of bone regeneration and wound healing, non-autogenous bone grafts can offer comparable advantages and results.
The tenting screw approach has been extensively studied and documented in the literature as an effective technique for enhancing soft and hard tissues in extensively resorbed edentulous sites. This method involves strategically placing one or more tenting screws on the buccal side of the ridge to achieve horizontal augmentation, with the screw heads positioned based on the desired amount of augmentation and distance from the cortical bone. Once the tenting screws are in place, bone graft material is applied to cover the screw shanks, followed by the application of a barrier membrane. The tenting screws provide a rigid “tenting effect” that promotes graft stability and maintains its dimensions, reducing the impact of external pressure during healing. Numerous studies have reported favorable outcomes and efficacy of the screw-tenting approach, highlighting its ability to achieve augmentation and facilitate successful implant placement. By incorporating this technique, clinicians can effectively address bone deficiencies, improve ridge dimensions, and create a favorable environment for dental implant placement.3,21,29
This case study highlights the importance of meticulous therapy planning, including clinical assessment and CBCT imaging, to accurately analyze the patient’s condition and quantify ridge dimensions for effective treatment planning. The use of autologous bone blocks in combination with allograft materials provides the advantage of utilizing the patient’s own bone as a scaffold for new bone production, while the allograft materials aid in the regeneration process. The successful bone regeneration observed in the follow-up CBCT scan demonstrates the effectiveness of this combination in increasing bone volume and stability.
In our case report, the use of the tenting screw technique with titanium screws resulted in a mean horizontal bone gain of approximately 5 ± 0.2 mm, consistent with previous literature on guided regeneration procedures using resorbable membranes for thin ridges. 30 This technique, combined with the use of particulate material and resorbable collagen membranes, provides a predictable approach with easy manipulation and fewer complications.31,32 The tenting screw technique has been shown to effectively increase the horizontal ridge dimension and facilitate subsequent implant placement while reducing graft material resorption.32,33 Overdrafting the desired horizontal gain above the screw head is advisable to compensate for graft material resorption. 34
Studies comparing different horizontal bone ridge augmentation strategies have found that the tenting screw technique when compared to titanium-reinforced membranes, results in fewer complications such as wound dehiscence, membrane exposure, and graft loss. 34 Resorbable membranes used in conjunction with tenting screws have shown lower infection rates and better wound-healing outcomes. 21 The technique has also demonstrated cost-effectiveness and prevention of graft migration, particularly in cases with flat ridges. 35
To ensure successful outcomes, flap advancement was carefully performed to achieve primary closure without tension, adhering to the “PASS” principle by Wang and Boyapati. 35 These findings highlight the advantages of the tenting screw technique, including its ability to enhance bone dimensions, reduce complications, and provide a stable framework for bone regeneration in preparation for implant placement.
As with any case report, it is important to recognize the limitations and potential variations that may exist when applying the findings to a broader population. Patient characteristics, anatomical variations, and surgical techniques can differ among individuals and settings, limiting the generalizability of the results. This case report represents a single patient case, which restricts the ability to draw definitive conclusions about the overall efficacy of the bone augmentation technique.
To further validate the findings and establish the reproducibility of the technique, larger sample sizes, and comparative analysis studies are needed. Long-term follow-up is essential to assess the stability and success of the implants, including factors such as implant survival, osseointegration, and potential complications that may arise over time. In a randomized controlled trial by Cucchi et al., 36 it was highlighted that early exposure or infection of bone regeneration procedures can increase the risk of failure, emphasizing the importance of long-term evaluation.
It is worth noting that successful horizontal and vertical bone regeneration using both resorbable and non-resorbable membranes has been reported by Merli et al. 37 although challenges may still arise. In this case, implant-supported prostheses were successfully used for the rehabilitation of the patient, and extensive bone remodeling and firm bone enclosure around each implant were observed after months of follow-up. It is recommended that clinicians exercise caution when applying the findings from this case report to other patients. Further research, including well-designed clinical trials with long-term follow-up, is needed to provide more robust evidence and guide clinical decision-making.
Conclusion
Tenting screw bone augmentation using autogenous/autologous+allograft presents a comprehensive and effective approach to address narrow ridges and vertical deficiencies in the mandibular region. This technique offers several advantages, including prevention of the soft tissue and periosteum from collapsing over the created space and protecting the particulate graft from resorption, high predictability, minimal invasiveness, cost-effectiveness, shorter healing time, and reduced patient morbidity. However, the suitability of this approach should be carefully assessed based on the unique characteristics of each case, patient factors, and the clinician’s expertise. By considering these factors and implementing evidence-based techniques, clinicians can achieve successful tenting screw bone augmentation and optimize dental implant outcomes in challenging cases. Nonetheless, further studies with longer follow-up periods and larger sample sizes are needed to confirm and validate these findings to establish the long-term efficacy and success of this approach.
Footnotes
Acknowledgements
The authors want to take this opportunity to express their appreciation to the research development and review cell of Altamash Institute of Dental Medicine Karachi, Pakistan, for guidance and support in this study. The author’s team is also grateful to the Yerevan State Medical University after Mkhitar Heratsi, Yerevan, Armenia, for supporting this project.
Author contributions
S.M.A.S. N.A. and A.H. contributed to the concept and critically reviewed the article; NA.A. A.Y. M.J.L A.H. and S.M.A.S. writing case report; S.M.A.S. and A.Y. M.J.L. and N.A. contributed to the concept and collected the patient information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.