
Abstract
New surgical techniques using narrow, tilted implants positioned through a magneto-dynamic tool in guided surgery for a Toronto restoration. A 69-year-old woman wanted fixed rehabilitation to replace her removable complete dentures. A cone-beam computed tomography showed significant bone resorption in both the maxillary and mandibular regions. The plan was to load the entire upper arch with six implants immediately, while removable partial dentures were recommended for the lower jaw. The guided surgery project was aligned with the new dentures, and the laboratory created a printed cast with dental implant analogues in planned positions. A metal-reinforced denture was constructed, and surgery was performed to place six narrow implants using the magneto-dynamic instrument. The denture was directly screwed onto multi-unit abutments. Final rehabilitation was completed after 6 months. Narrow implants can be a good option for fixed, full-arch rehabilitations. Further research is needed to confirm these findings on a larger scale.
Keywords
Introduction
The World Health Organization considers edentulism (total tooth loss), a physical disability1,2 Most edentulous patients can chew their food with complete dentures, but over time, the lower and upper jaw becomes resorbed, and bone has been reduced to retain the dentures.
This makes it more challenging to retain the denture, which causes problems for the denture-wearer, such as difficulties in eating and speaking, which may lead to a change in lifestyle, as those affected become embarrassed to socialise and live with others. 3
The dental literature is awash with papers showing significant improvements in quality of life in edentulous patients with dental implants placed in their jaw to secure their dentures. 4
However, this treatment is costly for individual patients and health services worldwide. For this reason, a new approach has been tried to reduce the cost.5,6 Furthermore, surgery to place implants is invasive, 7 which could be a barrier to treatment even when provided free of charge.8,9 Edentulous patients are often older people (over 65 years) and may have significant bone resorption in their jaw and complex medical histories, affecting their suitability for implant treatment.
For all these reasons, the request for less invasive treatment will increase in contemporary daily dentistry practice. All over the world, lots of edentulous patients search for fixed dentures, but lots of them want fast and less invasive procedures.6,10–14 Recently, many minimally invasive techniques have been developed to achieve better results in oral surgery, for example, piezoelectric and magneto-dynamic surgery15–20 or fewer implants to retain fixed rehabilitations.21,22 Clinicians all over the world are searching for reliable solutions to treat edentulous patients with reduced bone volumes trying to optimise the implant’s macro and micromorphology and analysing the behaviour of peri-implant tissue.6,9,23–30 Guided bone regeneration (GBR) is a reliable and validated solution,31–34 but it is invasive and has extended treatment times.
For this reason, some clinicians started to study the reliability of alternative solutions.12,13 To address these challenges, there is a growing demand for less invasive, cost-effective treatment options that provide faster results. Minimally invasive techniques, such as piezoelectric and magneto-dynamic surgery, have been developed to optimise oral surgery outcomes. Additionally, clinicians are exploring alternative solutions for edentulous patients with reduced bone volumes, aiming to improve implant macro and micromorphology and analyse peri-implant tissue behaviour. While GBR is a reliable option, it is invasive and time-consuming, prompting researchers to study alternative approaches.
This case report aims to validate the applicability and reliability of this alternative approach compared to conventional techniques. The use of narrow implants and magneto-dynamic tools aims to reduce surgical trauma, enhance bone expansion and achieve better bone quantity and quality around the implants. This study contributes to the growing evidence of less invasive dentistry approaches for edentulous patients with challenging clinical conditions. This case report presents an alternative solution to validate its applicability and reliability compared with traditional techniques.
In particular, will a case in which the surgeon, to perform six implants retained full arch rehabilitation, chose narrow implants to avoid doing GBR procedures, and magneto-dynamic tool with guided surgery to reduce the trauma and timing to obtain a bone expansion and osteocondensation to have better bone quantity and quality around implants.
Case
Patient information
A 69-year-old female patient comes to the dental office requesting a fixed rehabilitation to replace her removable complete dentures. She lost all her upper anterior teeth in a horse accident that determined a sizeable alveolar bone loss. A thorough anamnesis was performed and showed no contraindications to oral surgery. The patient reported no drugs taking.
The patient reported a dental history of several extractions due to decay and fracture problems.
Written informed consent was obtained from the patient for her anonymised information to be published in this article.
Clinical findings
At the physical examination clinician, a total loss of upper teeth was reported (Figure 1), which were replaced with complete dentures and the maintenance of anterior lower teeth (from 3.3 to 4.3). The patient lost occlusal vertical dimension and certainly needs full mouth rehabilitation. No Temporomandibular disorder or muscular symptoms were found.

Pre-op upper arch situation.
The residual lower teeth appeared in good periodontal conditions.
Diagnostic assessment
The surgeon prescribed a cone-beam computed tomography exam (Figure 2) that showed remarkable bone resorption in both the maxillary and mandibular areas, not due to pathologies linked with degenerative diseases.35–38

Pre-op cone-beam computed tomography.
The treatment plan provided an entire arch, immediate loading rehabilitation, six implants retained in the upper jaw and removable partial dentures in the lower jaw. According to the patient, the surgeon used narrow implants in the residual bone combined with a magneto-dynamic tool (Magnetic Mallet – Osseotouch, Gallarate, Varese, Italy) to avoid GBR procedures. The Magnetic Mallet is used both to implement standard surgical protocols and more advanced ones, where preserving the bone allows the procedure to be significantly simplified: extractions, maxillary sinus lifts, split crest, bone modelling and osseodensification. With the crown remover handpiece, removing cemented bridges and crowns with unthinkable speed and ease is possible compared to traditional methods (Figures 3 and 4). The magneto-dynamic mallet, used in dental implant site preparations, operates using electromagnetic technology. It generates controlled, precise impacts through a magnet-driven mechanism. This tool allows for the forceful yet accurate manipulation of the surgical site, facilitating osteotome insertion into the bone. Unlike traditional methods, which rely on manual force, the magneto-dynamic mallet delivers consistent and targeted impacts, resulting in less bone trauma and more efficient implant site preparation. This technology balances the need for forceful intervention and the delicacy required in dental surgeries.

Magnetic Mallet Osseotouch (Magnetic Mallet – Osseotouch, Gallarate, Varese, Italy).

Magnetic Mallet Osseotouch bone addensation working scheme.
Thanks to guided surgery software, dental implant insertion has been planned (RealGuidePro, 3DIEMME, Como, Italy). The dental laboratory has been able to provide a surgical implant guide (Figure 5).

Preliminary cast, the surgical guide and immediate provisional prosthesis.
Therapeutic interventions
The first has taken an alginate impression to make an individualised tray for the second impression. When the second date has been taken over a polysulfide impression (Plastic, 3M, St. Paul, MN, USA), the dental laboratory prepared an occlusion check on which a facial bow was recorded.
On the third date, the patient was submitted to an aesthetic try-in of new complete dentures that would be the definitive shape of the immediate loading dentures.
In this phase, the surgeon and laboratory matched the guided surgery project with new dentures, and the laboratory built a printed cast with dental implant analogues inserted in the planned positions.
A metal-reinforced denture was built on this cast, keeping open holes in the position of the planned implant to fix the situation after surgery.
On the fourth date, surgery has been performed. Six fixtures have been inserted using a magneto-dynamic tool (Osseotouch–Gallarate, Varese, Italy) on site 17 (4.10 × 10 Outlink SP, Sweden&Martina, Padova, Italy), 14 (3 × 11.5 Slim Outlink 2, Sweden&Martina, Padova, Italy), 12 (3 × 11.5 Slim Outlink 2, Sweden&Martina, Padova, Italy), 22 (3 × 10 Slim Outlink 2, Sweden&Martina, Padova, Italy), 25 (3 × 11.5 Slim Outlink 2, Sweden&Martina, Padova, Italy) and 27 (4.10 × 8.5 Outlink SP, Sweden&Martina, Padova, Italy). According to the literature, the insertion torque of every fixture was about 50 N/cm to perform the immediate loading technique (Figures 6–9). 19

Surgical guide in situ.
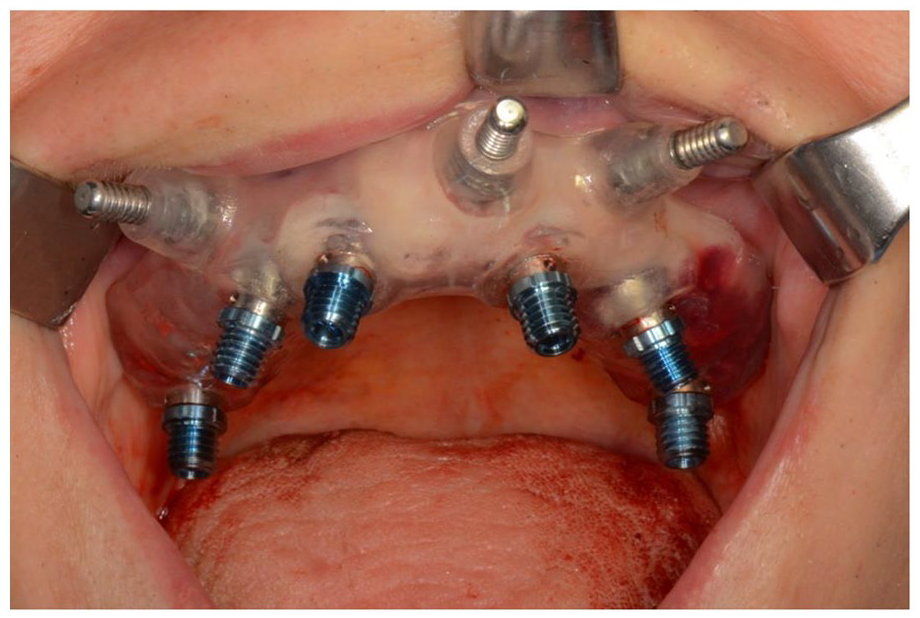
Implants insertion with a surgical guide.
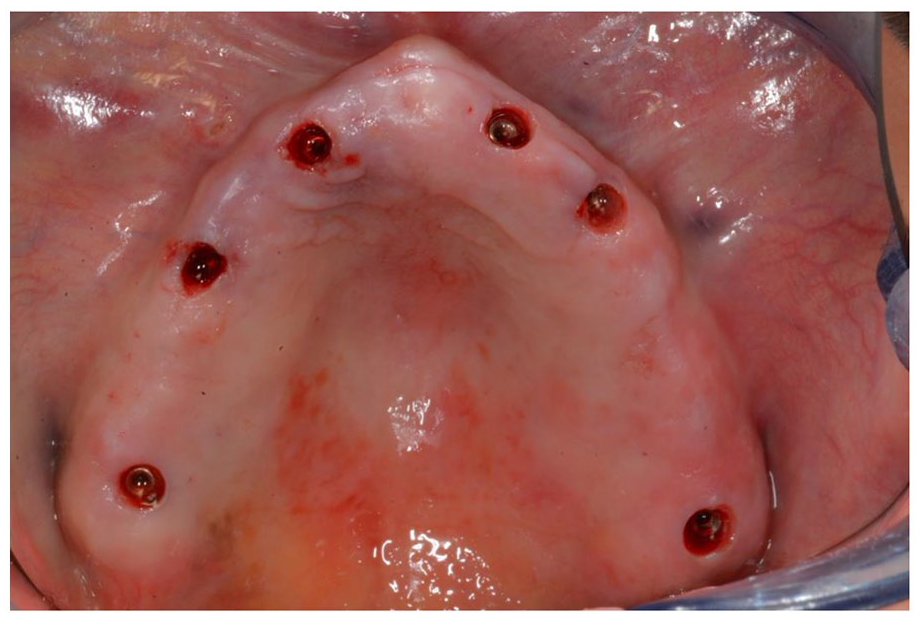
Post-op appears the arch situation.

Open tray impression coping.
Immediately after surgery, the provisional denture was placed and screwed on three tilted and three straight Multi-Unit Abutments (Sweden & Martina, Padova, Italy) to avoid the problem of retrievability with the cement fixation (Figure 10). 39

Final intraoral situation.
The patient has been subjected to monthly recall to check occlusion and hygienic maintenance.
After 6 months, rehabilitation was finalised. A polyether impression on dental implants has been taken, and a final denture has been built with reinforced metal frameworks13,34 and acrylic resin coating, copying the provisional denture’s shape. The final restoration so has been carried out with an acrylic-metal reinforced, screwed prosthesis (Toronto Bridge type; Figures 11–13).

Definitive Toronto Bridge.

Final extraoral situation.

Final intraoral situation.
Follow-up and outcomes
The patient has been inserted in a 4-monthly recall programme with occlusion check and correct hygienic follow-up.40,41 The patient refers to good chewing and speaking capability. The absence of spontaneous or induced symptoms and the state of the peri-implant tissues justify a good state of dental implants from an objective examination point of view (Figure 14).

Postoperative orthopantomography (12 months).
Discussion
This case report presents a successful alternative approach for rehabilitating a 69-year-old female patient with post-traumatic edentulism. The patient had experienced significant bone resorption due to a horse accident, leading to the loss of her anterior teeth and a large amount of alveolar bone. Traditional implant placement techniques, such as GBR or sinus lift procedures, were avoided to minimise invasiveness and reduce treatment time. Instead, narrow implants were combined with magneto-dynamic surgery and guided surgery techniques. The use of narrow implants in full arch rehabilitation has emerged as a potential therapeutic option for edentulous patients with reduced bone volumes. By utilising narrow implants, clinicians can overcome the limitations of inadequate bone volume and avoid more invasive bone regeneration procedures. The results of this case report support the idea that narrow implants can be a valid alternative to conventional implants in such clinical conditions. In addition to using narrow implants, the implementation of magneto-dynamic surgery with a magnetic mallet instrument offers several advantages. This innovative technique allows for bone expansion and osteocondensation, enhancing the quantity and quality of bone around the implants without more aggressive procedures. The magnetic mallet instrument has been shown to reduce surgical trauma. It can be used in oral bone surgeries, including dental extraction, split ridge procedures, sinus lifts and implant site preparations. While limited observational clinical studies have investigated the efficacy of this instrumentation, further comprehensive research is needed to validate its effectiveness.32–35 The integration of guided surgery techniques also played a crucial role in the successful outcome of this case. Computer-guided surgery has become a gold standard in full arch rehabilitation, enabling prosthodontically guided implant insertion and optimising operative and laboratory timing in immediate loading techniques. Guided surgery offers less invasive and painless surgical access, making it an attractive option for clinicians and patients. Despite the favourable outcomes observed in this case report, it is essential to acknowledge its limitations. As a single case report, generalisability to a larger population is limited. Further comprehensive studies involving a larger sample size and long-term follow-up are necessary to validate the effectiveness and reliability of the presented technique. Additionally, the success of any treatment plan is highly dependent on the individual patient’s systemic and local factors, which should be carefully assessed before considering narrow implants and magneto-dynamic surgery as treatment options.39–41
Within the scope of this case report, narrow implants combined with magneto-dynamic surgery and guided surgery techniques offer a viable alternative to conventional implants for full arch rehabilitations in patients with disadvantageous clinical conditions and without systemic or local limitations. These approaches provide the potential for reduced invasiveness, shorter treatment times and improved patient comfort. However, further research is needed to substantiate these findings and establish this treatment modality’s long-term success and reliability. In 2003, Malo et al. 34 showed that fixed rehabilitations should be performed using only four implants in the mandible. This concept opened a new paradigm in this kind of rehabilitation, performed with many long implants (six or eight). It was extended 2 years to maxillary rehabilitation of the entire arch. 35
This therapeutic option also started to overcome the problem of reduced bone volumes. Only four implants had less necessity of residual bone volumes. In the following years, this concept was emphasised using tilted implants. All these solutions gave patients a valid, cheaper and faster alternative to GBR techniques. 41
Researchers worldwide have started to study all possible solutions to minimise the invasiveness of oral surgery. Another evolution was the introduction of short and narrow implants that could be used in vertical or horizontal bone defects, avoiding regeneration techniques in mandibular and maxillary rehabilitations.42,43 Using a prosthesis screwed with a flange also helps to rehabilitate the hard and soft tissues lost by the patient as well as the dental and functional masticatory component. This also has an important impact from an aesthetic point of view of the face and on the support of the peri-oral tissues. Some studies suggest the transformation of a removable prosthesis into an implant-supported one can help all patients with benefits in chewing ability, aesthetics and satisfaction. Implant-supported rehabilitation can be used in place of replacing RPDs (removable partial dentures) with a higher quality of life in all aspects of patients’ lives.44–46 The use of narrow implants in full arch rehabilitation could be a new therapeutic possibility to give edentulous patients a chance to have fixed dentures that are cheaper, faster and painless. At the same time, using magneto-dynamic tools can reduce the trauma of surgery by enlarging the bone’s horizontal thickness without more aggressive procedures (split crest, GBR). The magnetic-dynamic technique has been recently introduced in oral bone surgery, such as dental extraction, split range, sinus lift and implant site preparation. Only one in vivo research, exploring clinical, radiological, histological and biological analyses, showed the effects of mallet instrumentation on the bone-implant site preparation compared to the drilling technique. 47
Antonelli et al., 48 in their in vitro study, assessed the initial stability of various implant designs using magneto-dynamic and traditional osteotomy in low-density bone, finding the magneto-dynamic technique more effective for higher primary stability. Bennardo et al. 49 conducted a systematic review to evaluate the effectiveness of the magnetic mallet in oral and implant surgery, suggesting the need for more extensive randomised controlled trials. Schierano et al., 50 in their pilot study in animals using magnetic mallet technology for dental implant sites, showed effectiveness in implant site preparation, particularly in poor bone quality cases. Bruschi et al., 51 in a retrospective study, analysed flapless trans-crestal maxillary sinus floor elevation with simultaneous dental implant placement, finding it safe and effective with low morbidity.
Toti et al. 52 introduced a mathematical method to estimate the correct pose of a blade implant from a two-dimensional radiograph, establishing its potential in standardised implant projections. Crespi et al. 53 assessed bone volume changes in maxillary molar regions after delayed implant placement, with CT scans showing successful outcomes at 3-year follow-up. Crespi et al. 54 studied the survival rate of immediate loading implants placed after the split-crest technique, showing a high success rate at a 2-year follow-up. Another study of the same research group 55 reported on electrical mallet use in osteotome-assisted sinus floor elevation with implants in fresh sockets, finding it efficient and accurate for such procedures. Crespi et al. 56 compared hand mallet versus electrical mallet in split-crest procedures, concluding the electrical mallet provided clinical advantages. Crespi et al. 57 conducted a clinical study comparing electrical versus hand mallets in maxillary bone condensing for immediately loaded implants, favouring the electrical mallet for clinical advantages.
At the same time, a more comprehensive clinical study will be necessary to validate this technique.
Another important consideration should be made about digital techniques; it has been developed in many fields, and in the last 10 years, computer-guided surgery has been designed and now should be considered a gold standard in full arch rehabilitation due to the possibility of projecting prosthodontic guided implants insertion, optimising operative and lab timing in immediate loading techniques.19,34 Guided surgery also provides less invasive and painless surgical access.7,21 The magneto-dynamic mallet in dental implant site preparations offers precise and less invasive techniques that preserve bone and reduce patient discomfort. Still, it requires specialised training, may be more costly, and might not be suitable for all types of bone densities or dental procedures.
Conclusions
In conclusion, this case report presents a promising approach for rehabilitating patients with post-traumatic edentulism using narrow implants, magneto-dynamic surgery and guided surgery techniques. Narrow implants offer a valuable alternative to conventional implants when dealing with reduced bone volumes, avoiding more invasive procedures. Integrating magneto-dynamic surgery with a magnetic mallet instrument facilitates bone expansion and osteocondensation, enhancing the bone quantity and quality around the implants. Guided surgery techniques contribute to precise implant placement and improved operative and laboratory timing. While the results of this case report are encouraging, it is essential to acknowledge the limitations. The findings are based on a single case report and may not generalise to a larger population.
Further studies with larger sample sizes and long-term follow-up are necessary to validate the efficacy and reliability of this approach. Before considering narrow implants and magneto-dynamic surgery as treatment options, it is crucial to take into account individual, systemic and local patient factors. In summary, narrow implants combined with magneto-dynamic surgery and guided surgery techniques show promise for full arch rehabilitation in patients with unfavourable clinical conditions without significant systemic or local limitations. These approaches offer the potential for reduced invasiveness, shorter treatment times and improved patient comfort. However, further research is needed to confirm these findings and establish this treatment modality’s long-term success and reliability.
Footnotes
Author contributions
L.F. and A.H.: Editing, reviewing, supervision; G.C.: Project Administration; N.S.: Formal analysis; F.M.M. and F.A.M.: Methodology and data collection; J.C.: Data collection and interpretation; D.B.: Writing original manuscript and methodology. All authors read and agreed on the manuscript.
Data statement
Data are available on request to Prof. Baldi.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Informed consent was obtained from all subjects involved in the study. Written, educated permission has been obtained from the patient for her anonymised information to be published in this article.