
Abstract
This case report emphasizes the complexities involved in dental implant placement within the anterior esthetic zone, focusing on the integration of advanced surgical techniques and meticulous prosthetic design for optimal esthetic and functional results. A 28-year-old male presented with the absence of the upper left central incisor, which had been extracted 5 years prior due to fracture. Clinical and radiographic assessments indicated normal alveolar bone levels; however, the esthetic demands required a specialized approach. The surgical procedure included a papilla preservation flap, immediate implant placement, and bone grafting to prevent peri-implant resorption and achieve an optimal emergence profile. An Osstem implant and resorbable Xenograft were utilized to address the thin labial bone. Over 4 months, successful osseointegration occurred, followed by the placement of a permanent crown. This case illustrates that dental implant restoration in the anterior esthetic zone can effectively address functional and esthetic challenges, leading to high patient satisfaction with the final restoration’s natural appearance.
Introduction
Following tooth extraction, especially in the anterior region, significant alveolar bone resorption is often observed due to the thin labial bone. In modern implantology, the esthetic zone frequently employs a prosthetic-driven approach, where the future crown dictates the implant’s position. The success of this approach heavily depends on the quality of the bone at the implant site. If the labial bone width is less than 2 mm, bone augmentation becomes necessary during implant placement. Studies by Tarnow et al. 1 and Buser et al. 2 have demonstrated that labial bone thickness exceeding 2 mm significantly reduces marginal bone resorption, thereby prolonging implant longevity. Buser et al. 3 further proposed guided bone regeneration (GBR) using bone grafts and membranes as a technique to enhance bone architecture during implant placement. Dental implants not only serve as replacements for missing teeth but also must ensure functional and esthetic success. High success rates have been reported, leading to the widespread adoption of implants in contemporary dental practice.4,5 This article delves into the critical aspects of implantology in the esthetic zone, emphasizing the importance of bone quality and advanced augmentation techniques for achieving long-term success. The integration of cutting-edge research and practical applications in this study offers valuable insights for clinicians aiming to master both the functional and esthetic demands of modern implant dentistry. This paper is poised to make a significant impact in the field, guiding best practices and enhancing patient outcomes.
Case report
A 28-year-old Thai male, single and practicing Buddhism, presented for consultation regarding dental implant placement. The patient had his upper left central incisor extracted 5 years prior due to an irreparable fracture. He reported no systemic conditions, drug allergies, or food allergies. Intraoral examination revealed the presence of 23 teeth, with the absence of the upper left central incisor. The patient currently uses a removable acrylic-based denture. Periodontal probing revealed depths of 2–4 mm generally, with no signs of caries or tooth mobility. Existing restorations were in good condition. There was generalized plaque and staining. The gingiva appeared pale pink overall, with normal gingival margins and papillae. The width of the keratinized gingiva was 4–6 mm. A defect in the anterior ridge of the upper left central incisor was noted. A panoramic radiograph indicated that the alveolar bone levels were within normal limits, and the extraction site demonstrated complete bone healing (Figure 1).

Panoramic radiograph showing the absence of the upper left central incisor with well-healed alveolar bone levels, setting the stage for implant placement.
Dental diagnosis
Treatment planning
During the hygienic phase, comprehensive oral hygiene instructions were provided, followed by full-mouth scaling to remove calculus. Upon re-evaluation, periodontal probing depths were found to be consistently 2–3 mm and plaque levels were significantly reduced from 70% to 10%. Given these improvements, the patient proceeded to the corrective phase, which involved the surgical placement of a dental implant accompanied by bone augmentation and subsequent crown restoration. The treatment plan included the use of a 3.5 mm diameter, 10 mm length Osstem dental implant (Osstem Implant, Co., Ltd., Seoul, Korea) and resorbable Xenograft bone graft material (A-Oss; Osstem Implant, Co., Ltd., Seoul, Korea), which is bovine-derived, with a volume of 0.25 CC.
Treatment procedure
Local anesthesia was administered using 3.4 mm of 4% articaine with 1:100,000 epinephrine, both buccally and palatally around the upper left central incisor. After achieving adequate anesthesia, an incision was made, followed by the elevation of a papilla preservation flap (PPF). The alveolar ridge was found to be wide, with a concavity on the labial aspect. The ridge width was approximately 5 mm bucco-palatally and 10 mm mesio-distally. A surgical stent was used to guide the osteotomy, which was initiated using a First guide drill to a depth of 10 mm. Implant alignment was verified with a parallel pin. Next, a second guide drill was used to further the osteotomy to a depth of 10 mm, followed by the Final drill, which had a diameter of 3.5 mm. After reaching the required depth, a 3.5 mm diameter, 10 mm length implant was placed with an insertion torque of 35 Ncm, achieving good primary stability. A 4.5 mm diameter, 4 mm high healing abutment was then placed to allow for non-submerged healing, ensuring the gingiva would not cover the implant. Due to the bucco-palatal ridge width of approximately 5 mm, the implant placement resulted in thin buccal and palatal bone and a labial concavity, causing the implant threads to be exposed labially. A resorbable Xenograft bone graft material (0.25 CC) was used for bone augmentation without the use of a membrane. The site was sutured with 4-0 Vicryl (Ethicon Inc., Johnson & Johnson Company, Somerville, NJ, USA), and the implant position was confirmed with a panoramic radiograph (Figure 2).

Clinical photographs and panoramic radiograph of the upper left central incisor implant placement: (a) papilla preservation flap with labially exposed implant threads; (b) xenograft bone augmentation at the labial concavity; (c) labial view of implant position; (d) occlusal view of implant position; (e) panoramic radiograph showing the implant placement.
Treatment outcomes
Following the dental implant surgery, no complications were observed, and the patient maintained excellent oral hygiene. The dentist allowed a 4-month healing period for osseointegration to occur, after which the patient was scheduled for impressions to fabricate the permanent crown. A transfer impression coping was used, and periapical radiographs were taken to verify the accuracy of the impression. The final impression was obtained using the double mixed single impression technique, and the model was sent to the laboratory for the fabrication of a permanent fixed prosthesis. This patient utilized the ARUM Pre-milled Abutment Blanks (ARUM Dentistry Co., Ltd. Daejeon, Korea) with anodized titanium to enhance the esthetic qualities by improving color concealment and reducing color reflection. The implant-abutment connection presented in the case features an internal hex with an 11° tapered connection, and it is planned to use an E-max CAD crown for esthetic considerations. The final step involved trying in the permanent crown and verifying the margin fit with a periapical radiograph. The crown was then cemented using permanent cement, and occlusion was checked to ensure light force with no shear forces during lateral or protrusive movements to avoid excessive loading on the crown (Figure 3).
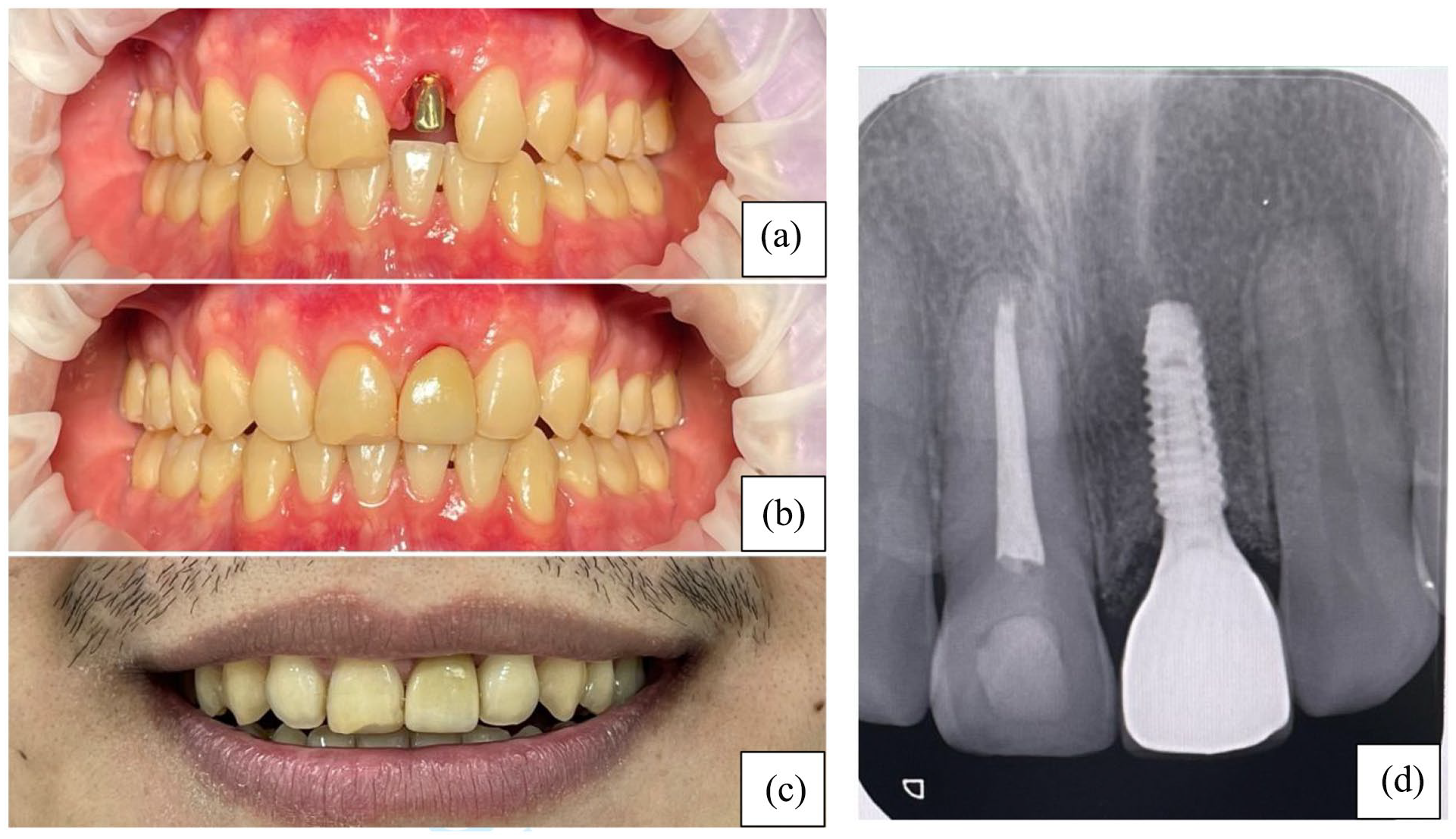
Final placement of the implant-supported crown: (a) position of the casting abutment; (b) permanent crown fixation on the implant; (c) patient’s smile line; (d) periapical radiograph post crown fixation, showing excellent alignment, natural coloration, and harmonious gingival contour with adjacent teeth.
Follow-up appointment
At the 3-month follow-up, the patient exhibited excellent oral health, with probing depths around the implant of 2–3 mm and no signs of gingival inflammation. The alignment and color of the implant-supported crown appeared natural, and the gingival contour harmonized well with the adjacent teeth. Radiographic evaluation showed no bone loss around the implant (Figure 4). The patient was advised on oral hygiene practices and received scaling and polishing. The patient was also instructed to return for regular follow-up and dental implant maintenance every 6 months.

Clinical photographs and periapical radiograph at the 3-month follow-up of the upper left central incisor implant: (a) the implant-supported crown showing natural alignment and color with well-integrated gingival contours; (b) patient’s smile line; (c) periapical radiograph showing no bone loss around the implant.
Discussion
The patient sought dental implant placement to replace a removable denture, presenting a challenging case due to the anterior location, where both functional and aesthetic outcomes are critical. The primary concern was the observed defect in the anterior gingival ridge, which resulted in an unappealing concavity. Additionally, the labial bone was found to be thin, measuring approximately 5 mm bucco-palatally. Combined with a 3.5 mm diameter implant, this resulted in insufficient bone thickness, leading to exposed implant threads on the labial side. This exposure increased the risk of peri-implant bone resorption, gingival recession, and potential peri-implantitis. 8 To address these challenges, I opted for a PPF technique to minimize the risk of the gingival recession on adjacent teeth. 9
Recent studies have introduced the tunnel technique for soft tissue grafting, which has proven to be a minimally invasive method for improving soft tissue thickness around implants. This technique reduces postoperative discomfort and provides excellent soft tissue outcomes, especially when a larger volume of keratinized tissue is required. When combined with the PPF, the tunnel technique can address both soft tissue and aesthetic concerns simultaneously. 10 Moreover, laser-assisted soft tissue surgery has emerged as a promising method for precise incision and reduced healing times. A study from 2023 demonstrated that laser technology when combined with soft tissue grafting, resulted in improved soft tissue outcomes and faster recovery times compared to conventional methods. 11
According to Tarnow et al., it is crucial that the implant be placed at least 1.5 mm away from adjacent natural teeth to prevent interdental bone loss, which could result in a black triangle, complicating oral hygiene and aesthetics. 1 In addition, the implant shoulder was positioned 3–4 mm apical to the cementoenamel junction to prevent vertical bone loss and gingival recession, especially in the esthetic zone. For bone augmentation, I applied a GBR approach using bovine-derived Xenograft without a membrane. The slow resorption of Xenograft provides a stable scaffold for new bone formation, ensuring long-term structural support. However, in recent years, synthetic bone substitutes and bioactive glass have become more widely studied and employed. These materials offer faster resorption rates, improved osteoconductivity, and better integration with host bone.12,13 A recent meta-analysis comparing Xenograft with synthetic bone substitutes indicated that the latter resulted in slightly better bone volume preservation, making them a compelling choice for challenging esthetic zones. 14 Furthermore, hydroxyapatite-coated implants have gained traction in bone augmentation procedures. Studies from 2023 suggest that these coatings enhance osteointegration by improving the interaction between the implant surface and surrounding bone. 15 The implant was restored with a healing abutment to allow non-submerged healing, a method that does not significantly differ in osseointegration outcomes compared to submerged healing.16,17 This approach eliminates the need for a second surgery to replace the cover screw but requires diligent oral hygiene around the healing abutment.
Considering both hard and soft tissue management is crucial for implant success. Adequate keratinized mucosa is essential for resisting inflammation and ensuring long-term implant stability, particularly in the anterior zone. Insufficient soft tissue thickness and non-keratinized mucosa can lead to unsatisfactory gingival contours and a future recession.18–20 Post-surgical healing typically requires 3–4 months for osseointegration, followed by prosthetic restoration with a permanent crown.21,22 Ensuring light occlusal forces is critical to avoid excessive stress on the implant, which could lead to fatigue of the implant components and potential failure. Thus, careful design and selection of the implant system are imperative to minimize occlusal forces.23,24
For anterior implant restorations, particularly in the esthetic zone, meticulous prosthetic design is essential. This involves the careful selection of abutment materials, emergence profiles, and crown types to achieve optimal aesthetic outcomes. In this case, an anodized titanium abutment could have enhanced translucency and better matched natural teeth, avoiding the potential grayish hue of titanium.25,26 Equally important is soft tissue management, where maintaining keratinized tissue and considering techniques such as connective tissue grafting could improve gingival contours and stability.27,28 Long-term success also hinges on patient compliance with oral hygiene and regular follow-ups to detect and manage peri-implant conditions early.29,30 The choice of the Osstem implant system, with its effective surface treatment for osseointegration, was appropriate, though newer laser-treated surfaces might offer additional benefits.31,32 The decision for a delayed loading protocol, allowing 4 months for osseointegration, aligns with evidence suggesting that this approach minimizes the risk of failure in challenging esthetic cases with thin bone and soft tissue profiles.33,34
Furthermore, the integration of advanced technologies in dental implant procedures has significantly improved both aesthetic and functional outcomes. Studies have highlighted innovative approaches to managing peri-implantitis, showcasing evidence-based strategies that enhance long-term success. 35 The application of CAD/CAM technology has revolutionized the fabrication of implant prosthetics, allowing for higher precision and better-fitting restorations. 36 A systematic review comparing immediate and delayed implant placements in the aesthetic zone supports the idea that timely intervention can yield superior results in specific clinical scenarios. 37 However, recent research suggests that in certain cases, immediate loading with appropriate soft tissue management can yield similar or even superior results, especially when combined with osseointegration-enhancing materials such as platelet-rich fibrin. This approach accelerates healing and reduces treatment time, benefiting patients seeking faster restorative solutions. 38
Moreover, recent advancements in implant materials and methods have addressed various challenges in the field, emphasizing the need for continuous innovation in implantology. 39 This growing body of literature underscores the importance of integrating these technologies to optimize patient outcomes and reduce complications associated with traditional implant procedures.40,41 A limitation of this case report is the absence of Cone Beam Computed Tomography (CBCT) imaging, as the author’s affiliated hospital does not have CBCT capabilities. Instead, ridge mapping combined with 2D radiography was used to assess bone thickness, which provided an adequate solution under the circumstances. 42
Future studies could focus on several key areas to enhance dental implantology. Longitudinal research is needed to evaluate the long-term aesthetic outcomes of implants in the anterior esthetic zone, assessing various materials and techniques. Comparative studies should investigate the efficacy of different bone augmentation methods, such as GBR versus grafting, on osseointegration and implant stability. Finally, exploring the integration of advanced imaging techniques such as CBCT could improve treatment planning for complex cases. Patient-centric approaches should examine the influence of patient education on compliance and satisfaction, while also investigating the performance of innovative implant materials and surface treatments.
Recent studies have emphasized the importance of patient education in enhancing compliance with oral hygiene protocols and ensuring regular follow-ups. A 2023 study on patient-centric approaches in implantology found that personalized care and educational interventions led to improved outcomes and reduced peri-implant complications. 43 These studies contribute significantly to refining techniques and improving patient outcomes in dental implantology.
Conclusion
This case report demonstrates the integration of advanced techniques and materials for achieving both functional and esthetic outcomes in the anterior implant zone, leading to high patient satisfaction with the final restoration’s natural appearance.
Clinical significance
This case emphasizes the importance of a comprehensive approach in anterior implant restoration, particularly in challenging esthetic zones. By integrating advanced surgical techniques such as papilla preservation and GBR, alongside meticulous prosthetic design and patient-centric maintenance, clinicians can achieve both functional and aesthetic success. The careful management of soft tissue and the strategic use of implant materials ensure long-term stability, while consistent follow-up care and patient education are critical for maintaining implant health. This holistic strategy not only addresses immediate restorative needs but also supports sustainable outcomes, reinforcing the necessity of precision and diligence in implant dentistry.
Footnotes
Acknowledgements
The authors would like to thank the PhD in Health Sciences Program at the Faculty of Medicine, Mahasarakham University, the dental staff at Fang Hospital, Thailand, and all contributors to this research.
Author contributions
J.J. contributed to the conception and design of the study, performed the clinical procedures, and drafted the manuscript. He was responsible for patient management, data collection, and analysis. R.C. and C.N. provided critical revisions and gave final approval of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.