
Abstract
Due to anatomical limitations, the posterior region often lacks sufficient alveolar bone height for conventional implants. Bone augmentation techniques have drawbacks, while short implants offer a minimally invasive option. This case report details a 48-year-old male patient who received short implants in the posterior region. After 7 years of functional loading, the implants remained stable with no loss or mechanical complications. The clinical outcomes were closely associated with the implant design, Morse taper connection, and occlusal adjustment of the restoration. However, short dental implants necessitate rational utilization and design, along with regular follow-up visits and occlusal evaluations. The present case aims to provide supplementary evidence for the long-term clinical application of short dental implants in bone-deficient posterior regions.
Keywords
Introduction
The posterior region often has insufficient alveolar bone height for conventional implant placement due to anatomical limitations such as the maxillary sinus and mandibular nerve canal. Various bone augmentation techniques (e.g., the sausage technique, block bone grafting, and ridge splitting) or procedures like inferior alveolar nerve transposition and distraction osteogenesis are commonly used to address bone height deficiency. However, these techniques have significant drawbacks: they often prolong the treatment period, increase surgical costs, and require a high level of technical precision. Moreover, postoperative complications are frequent, with unpredictable outcomes in some cases. 1 With a deeper understanding of implant restorations, short implants have emerged as a more minimally invasive and predictable clinical option. Placing short implants in sites with insufficient bone height can avoid complex surgical procedures, shorten the surgical period, reduce costs, expand the indications for implant restoration, minimize postoperative complications, and enhance patient satisfaction.2–4 Fernandes et al. 5 confirmed in their long-term follow-up study that short implants (6.0–8.5 mm) demonstrated comparable survival and success rates to standard-length implants over an average follow-up period of 74.08 months. Reports from the 2018 ITI Implant Conference indicate that short and conventional implants exhibit similar survival rates within the first 5 years. By contrast, after more than 5 years of loading, the survival rate of short implants declines significantly, reflecting a gradual decrease over time. 6 There are few reports on short implants under long-term loading (>5 years), especially regarding narrow-neck short implants in the posterior region. This study reports a case where short implants were used in the posterior region, with the unique feature of a crown-to-implant (C/I) ratio of ~2–3:1 for the implant-supported restoration and the use of a narrow-neck short implant in the right mandibular posterior region, demonstrated stable osseointegration and no mechanical complications after 7 years of functional loading.
Case presentation
This study was conducted in accordance with the ethical guidelines of the World Medical Association as outlined in the 2013 Declaration of Helsinki.
A 48-year-old male patient requested implant restoration for missing posterior teeth. He had been missing bilateral posterior teeth for over a decade with no specific medical conditions. Intraoral examination revealed the absence of teeth 16, 17, 46, 47, 23, 24, 25, 26, 27, and 37. The right mandibular posterior region exhibited significant buccolingual collapse of the alveolar ridge. Meanwhile, the remaining teeth presented varying degrees of wedge-shaped defects and gingival hygiene issues, including generalized grade III dental calculus. Radiographic examination showed significant alveolar ridge resorption, with a bone height of ~6–8 mm in the posterior region (Figure 1(a) and (b)). The preliminary diagnosis was partial edentulism.
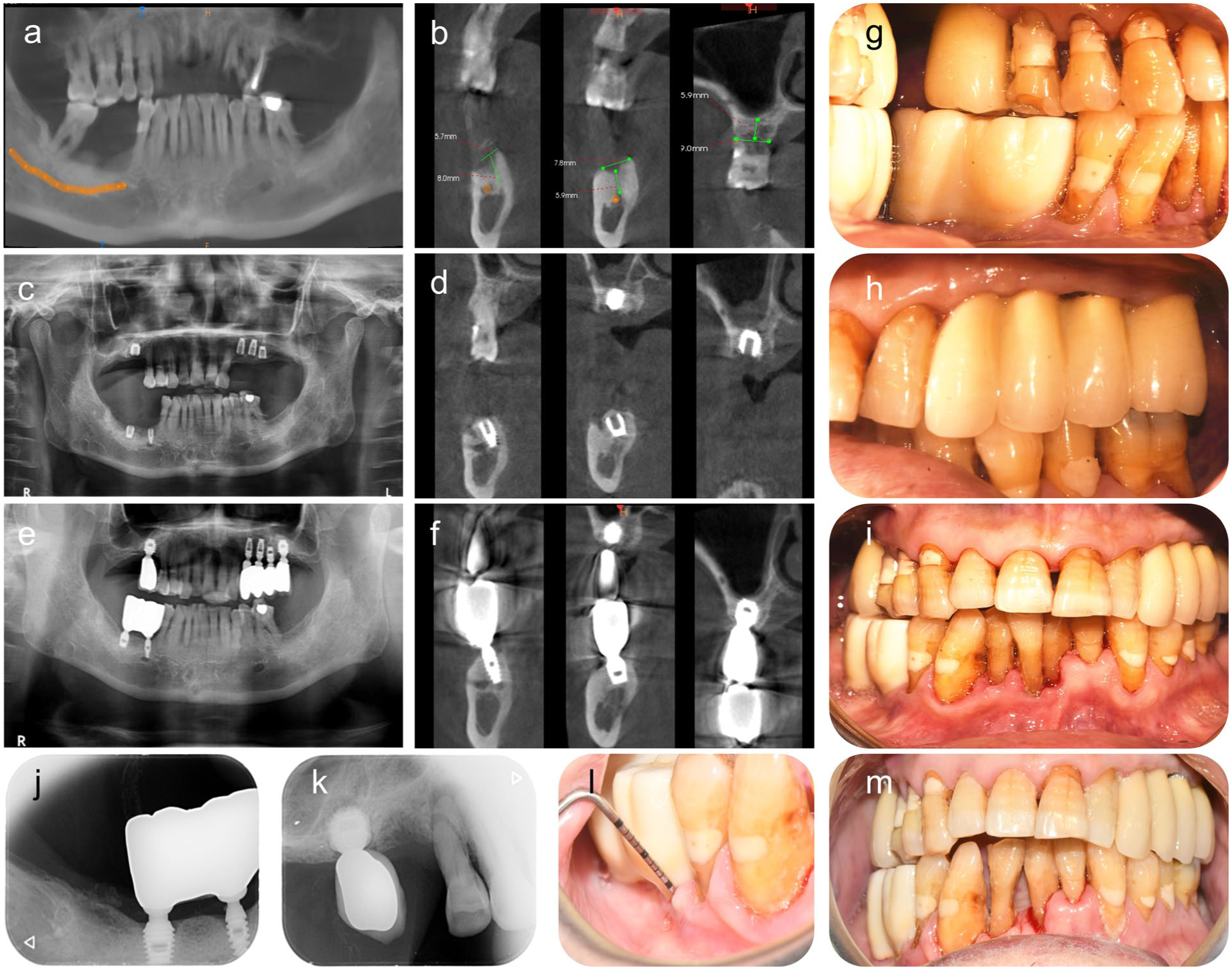
(a, b) Preoperative Cone Beam Computed Tomography(CBCT) images. (c, d) Postoperative radiographs. (e, f) Radiographs at 7-year follow-up. (g–i) Final restoration. (j–m) Periapical radiographs and intraoral photographs at 7-year follow-up.
The patient received preoperative pharmacological prophylaxis with ibuprofen sustained-release capsules (0.3 g, one tablet) and dexamethasone acetate tablets (3 mg, four tablets) administered orally 30 min prior to surgery. Oral antisepsis was performed using 0.12% chlorhexidine gluconate mouthwash, with two rinses of ~10 mL each, lasting 30–60 s/rinse and involving vigorous gargling. The oral and maxillofacial region was prepped with 0.5% iodophor, extending superiorly from the orbital rim to the upper neck and laterally to the anterior auricular border. A sterile surgical drape was applied, and local anesthesia was delivered via infiltration of articaine hydrochloride with epinephrine (1:100,000) at the surgical sites.
Six locking taper implants (Bicon LLC, Boston, MA, USA) were placed with subcrestal positioning of 1–2 mm and buried healing. The implant dimensions and anatomical positions were as follows: tooth 16 (6.0 × 6.0 mm), tooth 23 (4.0 × 8.0 mm), tooth 24 (4.0 × 8.0 mm), tooth 25 (4.5 × 8.0 mm), tooth 46 (3.5 × 8.0 mm), and tooth 47 (4.5 × 6.0 mm; Figure 1(a)). Postoperative panoramic radiographs confirmed optimal mesiodistal and axial alignment, with implant apices positioned in close proximity to the mandibular nerve canal and maxillary sinus floor (Figure 1(c) and (d)). Hemostasis was achieved by applying sterile gauze for 30 min. For the first 72 h postoperatively, the wound was irrigated alternately with 3% hydrogen peroxide and sterile normal saline to prevent infection every day.
Postoperative medication included metronidazole tablets for 7 days for antimicrobial prophylaxis, dexamethasone acetate tablets for 2 days for edema control, and 0.12% chlorhexidine mouthwash for 7 days for biofilm suppression. Sutures were removed at 7 days postoperatively, and the patient reported no pain, swelling, or functional disturbance.
Due to satisfactory surgical outcomes and personal financial considerations, a second implant (6.0 × 6.0 mm) was placed at tooth 26 on March 9, 2018. Following a 4-month osseointegration period, a second-stage surgical exposure was performed. After 2–4 weeks of gingival contouring, implant-level impressions were taken, and a splinted, non-anatomical zirconia prosthesis was fabricated and delivered. Teeth 23–26 and 46–47 received splinted crown restorations, and tooth 16 received a single crown restoration. Final restoration was completed on October 25, 2018, with occlusal adjustment confirming the absence of lateral interferences (Figure 1(g)–(i)). The patient was instructed to avoid mastication of hard or sticky foods to preserve prosthetic integrity. Seven-year follow-up revealed no implant failure, no mechanical complications, and favorable radiographic findings. The patient reported high satisfaction with masticatory function.
Discussion
The implants demonstrated excellent long-term stability at the 7-year follow-up, with no implant failure or mechanical complications. Mild gingival erythema was observed at select sites; however, probing depths remained within healthy limits. This indicates preserved peri-implant tissue integrity (Figure 1(f)–(i)). This clinical success stems from the system’s unique biomechanical design. The implants, made of high-strength Ti-6Al-4V alloy, incorporate deep, large threads and a fin-like surface. Consequently, the osseointegration surface area increases by over 30% compared to conventional implants of similar dimensions. The inter-fin spaces facilitate the formation of Haversian bone, enabling optimal load distribution across the surrounding alveolar bone under functional occlusion. 7 Although the probing depth in this case remained within the healthy range, a long-term study 8 indicated a significant negative correlation between keratinized mucosal width and probing depth, suggesting that adequate keratinized mucosal width positively contributes to peri-implant soft tissue health. The design of the patient’s connected splinted crowns is now considered unsatisfactory. Creating self-cleansing pathways would likely be more favorable to the peri-implant tissues. The changes in marginal bone levels observed over the 7-year period are consistent with recent research findings. 8 The abutment, also constructed from Ti-6Al-4V, integrates with the implant via a precision Morse taper connection, ensuring rigid, stress-conductive fixation without micro-movement. 9 Morse taper connection provides superior bone preservation compared to external hex implants. 8 In the mandibular region, where bone width at tooth 46 was limited, a narrow-neck short implant (3.5 × 8.0 mm) was placed with 1 mm of buccal and lingual bone preservation, yielding a C/I ratio of 2.2:1. Given the experience with the C/I ratio of natural teeth, one of the early concerns about short implants was the C/I ratio. However, studies have shown that the C/I ratio of implants has a relatively high tolerance. A prospective 5-year follow-up study compared the failure rate, any complications, marginal bone loss, and success rate of short implants with different C/I ratios. The results showed that a higher C/I ratio did not affect the survival rate, and the use of short implants can be considered advantageous and entirely reasonable.4,10 In this case, a splinted crown restoration was employed, which may have exerted a positive impact on stress distribution. Studies have demonstrated that the stress levels around implants with splinted crown restorations are significantly lower than those around single implants.11,12
Reducing the occlusal surface, flattening the cusp inclination, and minimizing off-axis loading contribute to more favorable load distribution and potential success of implant treatment. Although the C/I ratio does not seem to be of great importance, considering the potential negative effects of a high C/I ratio and narrow short implants, non-anatomical cusps were used in this case to restore function while reducing lateral loading. Axial forces are more conducive to the long-term stability of the implants. Patient compliance with instructions is also crucial for long-term success. The patient had severe periodontitis and underwent scaling and root planing during the first 3 years of follow-up after restoration. The patient was lost to follow-up for 4 years due to personal reasons, but returned for examination in 2025 and showed poor oral hygiene. Therefore, strengthening oral hygiene education and strict regular periodontal treatment are necessary (Supplemental Material).
Conclusion
This case report demonstrates satisfactory clinical outcomes. The locking taper implant may represent a treatment option for the posterior tooth region that combines minimal invasiveness with long-term efficacy. With rational design, it can effectively address cases of insufficient bone mass in the posterior tooth area.
Supplemental Material
sj-pdf-1-sco-10.1177_2050313X261436128 – Supplemental material for Long-term functional outcome of short implants in the posterior region with a follow-up of 7 years: A case report
Supplemental material, sj-pdf-1-sco-10.1177_2050313X261436128 for Long-term functional outcome of short implants in the posterior region with a follow-up of 7 years: A case report by Xun Xia, Chang-Qi Hu, Jiang-Qin Huang and Hong-Wu Wei in SAGE Open Medical Case Reports
Supplemental Material
sj-pdf-2-sco-10.1177_2050313X261436128 – Supplemental material for Long-term functional outcome of short implants in the posterior region with a follow-up of 7 years: A case report
Supplemental material, sj-pdf-2-sco-10.1177_2050313X261436128 for Long-term functional outcome of short implants in the posterior region with a follow-up of 7 years: A case report by Xun Xia, Chang-Qi Hu, Jiang-Qin Huang and Hong-Wu Wei in SAGE Open Medical Case Reports
Footnotes
Consent for publication
The patient has provided informed written consent for the use of their photographs and medical information to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.