
Abstract
Morgagni hernia is a rare congenital diaphragmatic hernia associated with the minor retro-xiphoid region between the sternal and costal attachments. The bilateral and complicated Morgagni hernia occurred exceptionally rarely, at a rate of 4% and 6.5%. An 81-year-old woman with occasional constipation went to the emergency department for epigastric pain and vomiting 3 days before. She could no longer pass gas that caused abdominal distention. Clinical examination and ultrasound showed partial bowel obstruction, an unspecified cause. She received nil per os, nasogastric decompression. The abdominal and chest computed tomography Scan showed the bilateral diaphragmatic hernia, and the dilated loops of the cecum and ascending colon were 7 cm. She required an emergency operation to resolve the etiology of bowel obstruction. The midline incision was chosen to release the hernia contents and repair the posterior sternal defects with Polypropylene mesh. An abdominal approach can solve a bilateral incarcerated Morgagni hernia.
Introduction
Morgagni hernia (MH) is a rare type of congenital diaphragmatic hernia (CDH) associated with the minor retro-xiphoid region between the sternal and costal attachments of the diaphragm with a prevalence of 1.5%–7% of this defect. The shape of the foramen of MH is a sternocostal triangle. 1 The MH is also referred to as the space of Larrey, named in honor of Napoleon’s surgeon, known as parasternal hernia, anterior diaphragmatic hernia, retrosternal hernia, substernal, or subcostosternal. However, the most common term is Morgagni hernia.1–3 The MH occurred extremely rarely on both sides, with an incidence of 4%. 4 Besides, the MH with complications due to obstruction or perforation also appeared lower, at a rate of 6.5%. 5 MH patients are more common in females and adults older than 50.4,5
Although MH is a congenital disability, it is usually diagnosed in adults due to non-specific symptoms. 2 About 30%–35% of cases have no symptoms. Signs of the patients are unspecific and range from dyspnea or cyanosis and cough to upper abdominal or chest pain and defecating disorders in approximately 30%–45.5%.5,6 Computed tomography is the most significant technology supporting the diagnosis.7,8 Some authors preferred the abdominal approach. 9 The problem of choosing the treatment of laparoscopic or open surgery is controversial, and the benefit of mesh augmentation in MH repair is unclear yet.4,5 However, surgical repair might be indicated to prevent and treat strangulated patients. 5
We present a bilateral MH case with bowel obstruction.
Case presentation
An 81-year-old woman (BMI = 24.4) with a history of occasional constipation, without any remarkable diseases, went to the emergency department due to epigastric pain and vomiting 3 days before. The patient’s complete blood count test was within normal ranges, and the Blood Urea Nitrogen level was at 14.2 mmol/l, and creatinine was at 114 umol/l. The symptoms were increasingly severe day by day. Besides, the patient could no longer pass gas that causes abdominal distention. The patient had a distended abdomen and increased bowel sounds on clinical examination. Ultrasound shows a dilated small intestine and ascending colon. The patient was diagnosed with partial bowel obstruction, an unspecified cause. She received non-operative treatment as nil per os, nasogastric decompression, and intravenous supplementation with fluids and electrolytes before getting the colorectal endoscopy and computer tomography (CT) Scan. After 24 h of follow-up, the patient didn’t gradually improve with those symptoms. She was assigned a CT Scan of the abdomen and chest with intravenous contrast. The CT Scan showed the bilateral diaphragmatic hernia with the diaphragm discontinuity irregularity bilaterally behind the sternum and the hernia neck measurements of 3 and 2.5 cm, respectively; the dilated loops of the cecum and ascending colon were 7 cm, and the small bowel loops were dilated over 3.5 cm. The middle transverse colon and colon distally were of the average diameter.
We performed an emergency operation to resolve the etiology of bowel obstruction. The “Midline incision” was selected due to the patient’s conditions, bilateral hernia, and bowel obstruction. Intraoperatively, we systematically examined the abdominal cavity. Intestinal obstruction with small bowel loops dilated over 4 cm and an ascending colon over 6 cm. The patient had a bilateral MH, which contains a greater omentum (Figure 1a). The greater omentum was incarcerated in the right foramen of the MH, pulling the transverse colon toward the diaphragm. This part of the transverse colon was raised high and constricted as a dilated bowel obstruction transitional point (Figure 2a). These hernia contents were pulled back into the abdominal cavity, releasing obstruction through the transitional zone. The bowel loops in the peritoneum didn’t have any adhesions. The next step was to seek the abnormal parts in the distal colorectum, but it was well. The right and left defects were 4 and 3.5 cm in diameter, respectively (Figure 1b). Hence, we decided to close the posterior sternal regions with Polypropylene mesh. The meshes overlap for the hernia necks of 1–2 cm was then fixed by polypropylene interrupted suture (Figure 2b). The patient was discharged within 3 days after surgery. There was no complication such as pneumonia, fluid collection, or recurrence during a 1-year follow-up.

(a) The blue arrow showed a great omentum image trapped in the bilateral Morgagni hernia (MH). (b) The orange arrow revealed the bilateral side of the MH.
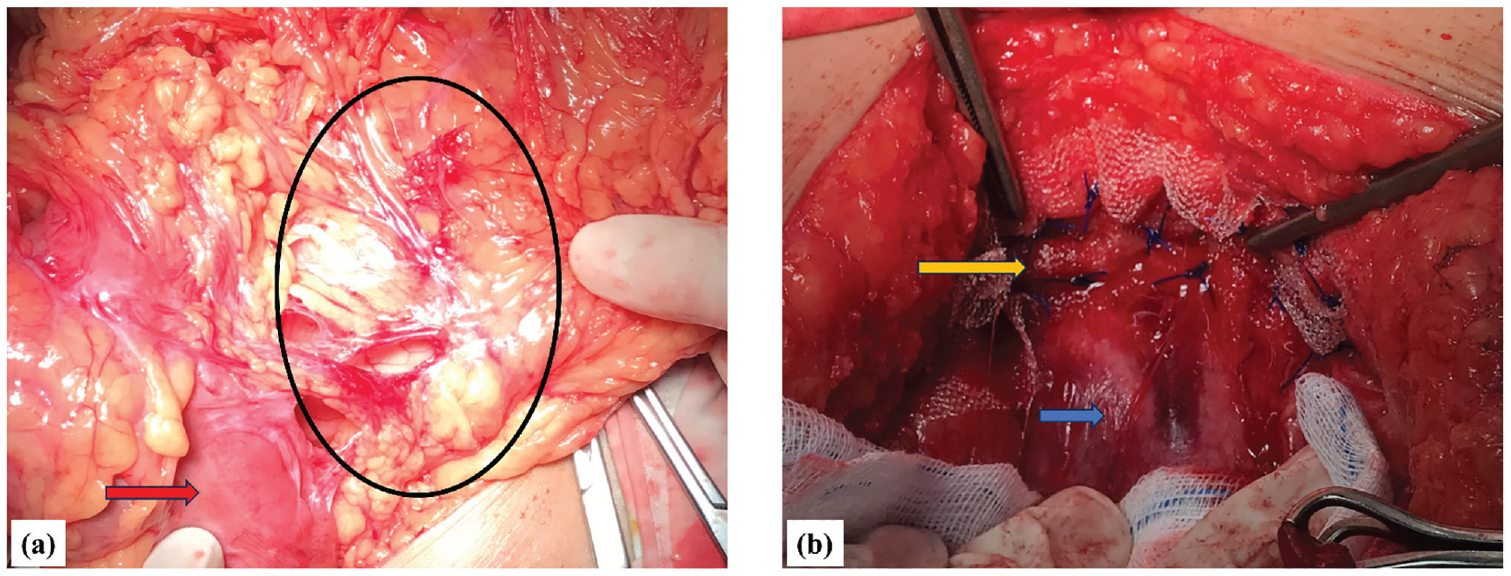
(a) The black oval showed the visceral content was incarcerated in the Morgagni hernia, and the red arrow was the transverse colon (b) The orange arrow was Mesh’s placement on both sides fixed, and the blue arrow revealed the parietal peritoneum. The shooting angle of this figure 2b is similar to that of 1b, with the image of Mesh covering two diaphragmatic hernias.
Discussion
The embryologically original diaphragm has four structures: the septum transversum, two paired pleuroperitoneal laminae form the central tendon with connective tissue scaffold, and the dorsal mesentery. Many theories have been described as the etiology of diaphragmatic anomalies. These theories believe the viscera of the abdomen migrates to the thorax, and the presence of viscera in the thoracic cavity leads to pulmonary hypoplasia and diaphragmatic defect. The lack of fusion of one or more of these structures can cause a variety of diaphragmatic anomalies. Significantly, the lack of fusion of the pleuroperitoneal laminae anteriorly guides to a defect in the costosternal trigones comprehended as the foramen of Morgagni. This triangular space results from a small hole of musculature on either side of the xiphoid process and the level of the 7th costosternal junction.1,10,11
The MH is often detected on the right side because the pericardial sac and the heart cover the left defect. Bilateral hernias have also been described rarely.1,3
Approximately 15%–20% of CDH cases are associated with a genetic cause, including chromosomal abnormalities, copy number variants, and sequence variants, while 80% remain unknown.12,13 Mutations, particularly CDH-associated chromosomal regions or genes, are incompletely penetrant, pleiotropic, and variable expressivity between affected individuals. 14
Federico et al. 1 believed that MH patients are usually asymptomatic. Unfortunately, Horton et al. 4 have reported that only 28% of patients were asymptomatic in 295 patient data. Signs were collected, including the following types: bowel obstruction, pulmonary symptoms, pain, pressure, dysphasia, bleeding, gastroesophageal reflux disease, and others such as fatigue, indigestion, and hypertension. Furthermore, in the results of Oppelt et al. 6 and Iso et al., 5 upper abdominal pain and respiratory or gastrointestinal symptoms may occur at approximately 30%–45.5%, whereas the asymptomatic rate was 27.3%–32.3%. Because of the rare disease, the small number of patients, and the retrospective study design, the evaluation of symptoms of these studies is affected. Hence, these above appointments differed.1,5,6 The symptoms associated with the contents of the hernia sac, such as bowel obstruction relating to contents with the small or large intestine, discomfort or reflux signs relating to contents with stomach, and abdominal pain relating to contents with omentum, while pulmonary complication might be relating to the hernia size. The collected symptoms were unspecifically similar. Therefore, the relationship between manifestation and hernia size has been controversial in recent literature.4,6 Missing the diagnosis can lead to severe complications such as incarceration or strangulation with necrosis of contents blocked in the hernia, although rare, similar to our presentation. 7
Chest X-ray appearance depends on the contents in the MH, which is the most common imaging to diagnose this type of CDH. However, the accurate diagnosis of radiographs in an MH can sometimes be mistaken when MH coexists with another diaphragmatic hernia.1,6 The hernia contents may be found in radiographs depending on herniated viscera but are usually missed. 15 Contrast examination as barium enemas may confirm the diagnosis when a visceral herniation exists. 1 Diagnosis may be omitted because of different presentations on a chest X-ray. An accurate diagnosis can be considered by CT or magnetic resonance imaging (MRI) with a non-invasive method.1,6 Minneci et al. showed that 83% of patients were correctly diagnosed with foramen of MH. CT and MRI were helpful for MH diagnosis with hernia containing a small size of foramen due to its degree of tissue characterization.6,8 Both CT and MRI can provide images in the coronal, sagittal, and axial planes. Therefore, a surgeon can avoid an unnecessary thoracotomy to diagnose the mediastinal fatty mass. 8
Surgical treatment is recommended in MH patients at the time of diagnosis. These complications may be life-threatening, such as incarceration, strangulation, volvulus, or obstruction of the sac contents.1,6,9 Therefore, the repair of whole MHs prevents the risk of complications, even in asymptomatic patients.
The choice of surgical approach is still debated according to the operative technique in MHs. Some authors support the transthoracic, 1 the transabdominal, 7 or the thoracoabdominal approach.7,9 Others select the video-assisted laparoscopic technique.16,17 The transabdominal approach is advocated to understand better bilateral hernias, complications, or intraabdominal pathologies.1,6 However, laparoscopic transabdominal repair has been increasingly described as safe and feasible. This approach significantly reduces the length of postoperative hospitalization1,2 as well as a trans-xiphoid hand-assisted video thoracoscopy approach. 16 Besides, almost all authors advocate minimally invasive surgery through the abdomen, with many advantages in recent years. Hence, laparoscopic transabdominal surgery is standard management.4,2,6 We recommend the transabdominal approach in MH patients, especially in complicated or bilateral cases. Reducing hernia contents, repairing the hernia sac, and resolving complications are easy. Our case was approached with laparotomy instead of laparoscopy because of abdominal distension and medical treatment failure, and the laparoscopic approach would put the patient at high risk of complications due to difficulties in technique and prolonged operative time in the elderly patient. Therefore, we chose the option of laparotomy to solve the cause of intestinal obstruction and repair two sites of the sternocostal space hernia.
Horton et al. 4 showed that 41% of patients with MHs have predisposing conditions associated with intraabdominal pressure, including pregnancy, obesity, chronic constipation, and chronic cough. These conditions increase the risk of hernia recurrence. Hence, surgeons should carefully decide on the method of sac repair. Primary closure, mesh interposition, or a combination of both were discussed.4,15 Venuta et al. suggested primary closure when the defects were smaller than 3 cm in diameter, whereas Thoman et al. advised <20–30 cm2 to avoid tension. 1 Due to the author’s judgments, the mesh must achieve at least a 1.5–2.5 cm overlap margin between the edge of the defect and the mesh.1,2
The evidence bases concerning prevalence, clinical symptoms, diagnosis, and treatment were present from single case reports and small retrospective cases. Nowadays, an increasing number of authors advocate the laparoscopic transabdominal approach. The advantages are shorter hospital stays, similar recurrent rates, and a lower complication rate. 18
Conclusions
Bilateral incarcerated MH is extremely rare in a CDH that can cause severe consequences. Many surgeons advocated the transabdominal approach because it provided a better overview of bilateral hernias and complications. Nowadays, laparoscopic transabdominal surgery is the standard for resolving this disease, with many advantages and a low recurrence rate.
Footnotes
Acknowledgements
Not Applicable.
Authors’ contributions
M.T.N. Data collection, conception, and design of the article, draft, and approval of the final version; A.V.P. Conception and design of the article, revisions, and approval of the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.