
Abstract
Evisceration of bowel through the stoma is a rare complication and only few cases have been reported. Although most cases occur in the context of long-standing parastomal hernias, early evisceration may also occur causing significant morbidity to patients. The reported patient is a 53-year-old male with bronchial asthma who was diagnosed to have metastatic colonic cancer underwent a trephine loop ileostomy for intestinal obstruction. On post-operative Day 7, he developed small bowel evisceration through the ileostomy site. The patient underwent an emergency laparotomy and found to have non-viable prolapsed small bowel segment at the stoma site. Furthermore, there were extensive peritoneal deposits and large para aortic lymph node mass and ascites compromising the peritoneal space. Resection of non-viable small bowel and ileostomy refashioning was carried out. The patient was managed in the intensive care unit and he gained function of the ileostomy on post-operative Day 2. On Day 5, he died due to subsequent pneumonia and worsening acute respiratory distress syndrome. Early parastomal evisceration is an extremely infrequent life-threatening complication that requires urgent treatment. Disseminated cancer, bowel obstruction, poor nutritional status, ascites and exacerbation of bronchial asthma were additional risk factors in our patient.
Introduction
Ostomy creation is associated with varying degree of early and long-term complications, approximately ranging from 20% to 70%. 1 Some of the common early complications include ischaemia, gangrene, retraction, obstruction and skin irritation. Other long-term complications include prolapse, stenosis and parastomal hernia. 1 These complications are associated with physical and psychological morbidity with significant impact on quality of life.2–4
Evisceration of bowel through the stoma is a rare complication and only few cases have been reported so far. 5 Although most occur in the context of long-standing parastomal hernias, early evisceration can also occur resulting in significant morbidity to patients. 5 We report a patient with metastatic colonic cancer who underwent a decompressing loop ileostomy for intestinal obstruction and subsequently had an early parastomal evisceration of small bowel. We also aimed to discuss the previously reported similar cases of early parastomal eviscerations.
Case presentation
A 53-year-old Sri Lankan male with bronchial asthma presented to the surgical clinic for further evaluation of anaemia and left supraclavicular lymphadenopathy. Apart from loss of appetite and loss of weight, he also had dyspeptic symptoms with intermittent colicky abdominal pain. On clinical examination; he had left-sided level-II lymphadenopathy, abdominal distension with a large para-aortic mass in epigastric and umbilical region and ascites. His ultrasound scan of the neck was in favour of metastatic lymphadenpopathy. Fine needle aspiration cytology (FNAC) of the lymph node mass confirmed an adenocarcinoma. His abdominal contrast-enhanced computed tomography (CECT) showed a malignant growth of the hepatic flexure with extensive mesenteric and para-aortic lymphadenopathy and ascites (Figure 1). During bowel preparation for colonoscopy, he developed features of intestinal obstruction and therefore, emergency trephine loop ileostomy was created. Intra-operatively, difficulty due to limited mobility of the small intestine was encountered.

Malignant growth of the hepatic flexure (yellow arrow) with extensive mesenteric and para-aortic lymphadenopathy.
His post-operative recovery was uneventful until post-op Day 7, where he developed acute onset pain at stoma site and found to have small bowel evisceration through the ileostomy site (Figure 2). The patient underwent an emergency laparotomy and found to have non-viable prolapsed small-bowel segment at the stoma site. Furthermore, there were extensive peritoneal deposits, large para aortic lymph node mass and ascites compromising the peritoneal space. Resection of non-viable small-bowel and ileostomy refashioning was carried out. The patient was managed in the intensive care unit (ICU), and he gained function of the ileostomy on post-operative Day 2. Unfortunately, he died on post-op Day 5 due to subsequent pneumonia and worsening acute respiratory distress syndrome (ARDS).
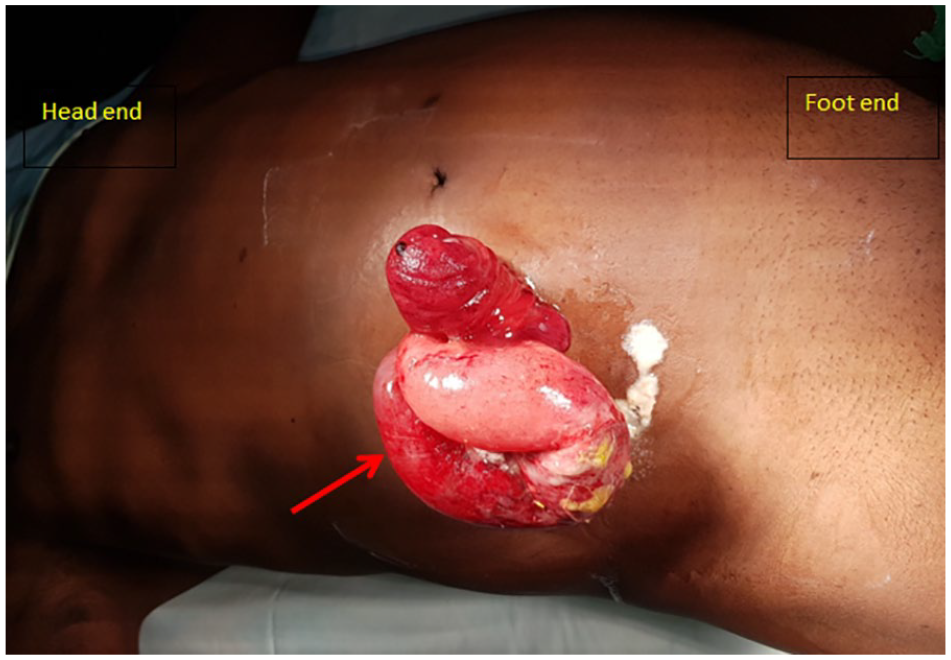
Small-bowel evisceration through the ileostomy site (red arrow).
Discussion and conclusion
Parastomal evisceration is a rare complication of ostomy creation, and less than 20 cases have been reported worldwide. 5 Although it is rare, it is associated with significant morbidity and mortality due to the risk of strangulation of prolapsed intestine. 6 This can occur in early post-operative period or as a late complication. Several aetiological factors have been postulated. 7 Conditions which increase the intra-abdominal pressure may predispose to stomal prolapse, parastomal hernia and may lead to evisceration. Previous reported cases of late parastomal evisceration were associated with parastomal hernias or other long-standing stoma-related complications. 5 Parastomal eviscerations have been report in the context of both temporary and permanent stomas as well as ileostomies and colostomies. Parastomal evisceration during the early post-operative period may be related to the surgical technique and other factors such as patient condition and the stage of the disease
A literature survey was performed, and previously reported cases of early parasomal evisceration are summarized in Table 1.6–13 Only nine cases of early parasomal evisceration have been reported worldwide. Majority of the patients were above the age of 60 years (Table 1), and there were eight males and one female. 12 All patients had evisceration within 14 days of ostomy creation and shortest being 3 days.10,13 Small bowel was found to be the commonly eviscerated part of the intestine. One patient had evisceration of omentum in addition to small bowel. 12 Chronic obstructive pulmonary disease (COPD), smoking and poor nutritional status were identified as associated risk factors. However, two patients did not have any identifiable risk factors.8,12 All patients were managed with emergency surgical intervention either laparotomy or by refashioning of the stoma.
Summery of the reported cases of early parasomal evisceration.

COPD: chronic obstructive pulmonary disease; ARDS: acute respiratory distress syndrome.
The reported patient had many contributory factors for evisceration. Patient had bowel obstruction within an already compromised peritoneal cavity due to peritoneal deposits; enlarged para-aortic nodes and ascites may have caused significant rise in the intra-abdominal pressure. Exacerbation of bronchial asthma may have further contributed to the increased abdominal pressure. Disseminated malignancy, poor nutritional status and impaired healing capacity might have caused an increased risk of stomal dehiscence. In the initial surgery, a larger opening of the anterior abdominal wall was created to accommodate the dilated small bowel. Resolution of intestinal oedema may have created enough space for the intestinal loops to prolapse through the stoma site.
The use of laparoscopy aids in both the diagnosis and therapeutic aspects of managing acute abdominal conditions. Improved visualization of abdominal pathologies helps in arriving at the diagnosis and laparoscopic management has early recovery and reduced length of hospital stay. 14 In selected patients, the use of laparoscopy in adhesive intestinal obstruction is helpful in relieving the cause of obstruction with adhesiolysis. 15 The acute obstruction due to luminal causes like large intestinal tumour can also be managed with laparoscopy with primary resection of tumour depending on the suitability of the patient. 16 In the reported patient, a diagnostic laparoscopy and the decision of the site of the stoma might have been useful for a tension-free, relatively smaller incision at the stoma site. Considering the CT findings, large para aortic nodes occupying the abdominal cavity might have hindered the use of safe laparoscopy as an option. Using a skin bridge might reduce the stoma-related complications and comparatively better early post-operative care of a loop stoma. 17
Unfortunately, the repeated surgical interventions resulted in significant morbidity to the patient. The added insult due to exacerbation of bronchial asthma and pneumonia complicated with ARDS resulted in mortality. As this was an emergency surgery, prior nutritional optimization was not feasible. In retrospect, the larger abdominal wall defect to accommodate the dilated small bowel should have been avoided, as it may have precipitated the small-bowel evisceration in the context of multiple risk factors including increased intra-abdominal pressure. A laparotomy in the first instance may have been more suitable to properly assess the disease and to create an adequately sized opening for the stoma. However, laparotomy has its own risk of wound complications and subsequent dehiscence in this patient. With the increasing incidence of colorectal cancers in the world including both developed and developing countries, 18 surgeons will continue to encounter such challenging cases in future.
Conclusion
Early parastomal evisceration is an extremely infrequent life threatening complication that requires emergency treatment. Disseminated cancer, bowel obstruction, poor nutritional status, ascites and exacerbation of bronchial asthma were additional risk factors in our patient. With the rising incidence of colorectal cancers, surgeons will continue to encounter such challenging cases in future.
Footnotes
Author contributions
O.B., U.J., Y.P. and N.G. contributed to collection of information and writing of the manuscript. K.S. contributed to writing and final approval of the manuscript. All authors have read and approved the manuscript.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient