
Abstract
Gallstone ileus is a rare entity and constitutes an uncommon complication of gallstone disease. It is caused by the impaction of a gallstone in the gastrointestinal tract and may cause serious symptoms or even life-threatening complications. It should be part of the differential diagnosis of acute abdomen especially in patients presenting with signs and symptoms of bowel obstruction and known gallstone disease. An early diagnosis is essential, and surgical treatment is the gold standard in order to relieve the obstruction. We present the case of an 84-year-old male patient with gallstone ileus due to cholecysto-intestinal fistula and impacted gallstone at jejunum. He was treated via urgent enterolithotomy, and his post-operative period was uneventful. This report aims to further educate clinical doctors on this rare medical condition which may pose a potentially serious health risk.
Introduction
Gallstone ileus (GI) is the bowel obstruction caused by the impaction of a gallstone in the gastrointestinal tract (GIT). 1 It is an uncommon complication of gallstone disease. 2 Only a small number of patients (0.3%–0.5%) will develop symptoms. 2 In the vast majority of these cases, the perforation of gallbladder, due to severe inflammation and pressure from the gallstones, is followed by adhesion of the nearby structures in order to halt the spreading abdominal contamination with infected bile. As a result, a cholecysto-intestinal fistula is formed through which gallstones pass into the GIT, bypassing the common bile duct (CBD). Recent reports claim that in more than 80% of cases, a connection is identified between gallbladder and duodenum. 3 Gallstones can also reach the intestinal lumen through CBD following endoscopic retrograde cholangiopancreatography and endoscopic sphincteromy. 4 Passage via an intact CBD and Vater’s papilla can rarely occur, and it represents less than 1% of all GI cases. 4
In almost two-thirds of cases, the obstruction is localized at ileum and ileocecal valve.5,6 Episodes of GIT obstruction are directly related to gallstones’ size. 6 Gallstones smaller than 2 cm are more likely to pass through the GIT and been excreted with the stools. 6
GI is considered a relatively rare cause of intestinal obstruction forming 1%–4% of all cases of GIT obstruction regardless of age. 7 However, in older patients, GI is much more common, counting in some reports for up to 25% of cases with GIT obstruction in patients over 65 years old. 7 The female-to-male ratio appears to be 4.5:1. 6
We report the case of an 84-year-old male patient with GI due to impacted gallstone at jejunum. This report aims to bring to clinicians’ attention this relatively rare entity and highlight the management options.
Case report
We present the case of an 84-year-old Caucasian male who was admitted to the hospital on 11 February 2022 with symptoms of vomiting, diffuse abdominal pain, nausea and obstipation. Patient’s past medical history was remarkable for diabetes mellitus type II, hypertension and dyslipidemia. Furthermore, he had no history of previous surgical interventions.
On inspection, he demonstrated signs of dehydration. The clinical examination revealed abdominal distention, intensified bowel sounds, tympany to percussion and sensitivity in all abdominal quadrants. In addition, there was no blood or palpable mass on digital rectal examination. The blood tests revealed elevated inflammatory markers, electrolyte disorders and deterioration of the renal function (Table 1).
Blood test results on admission.
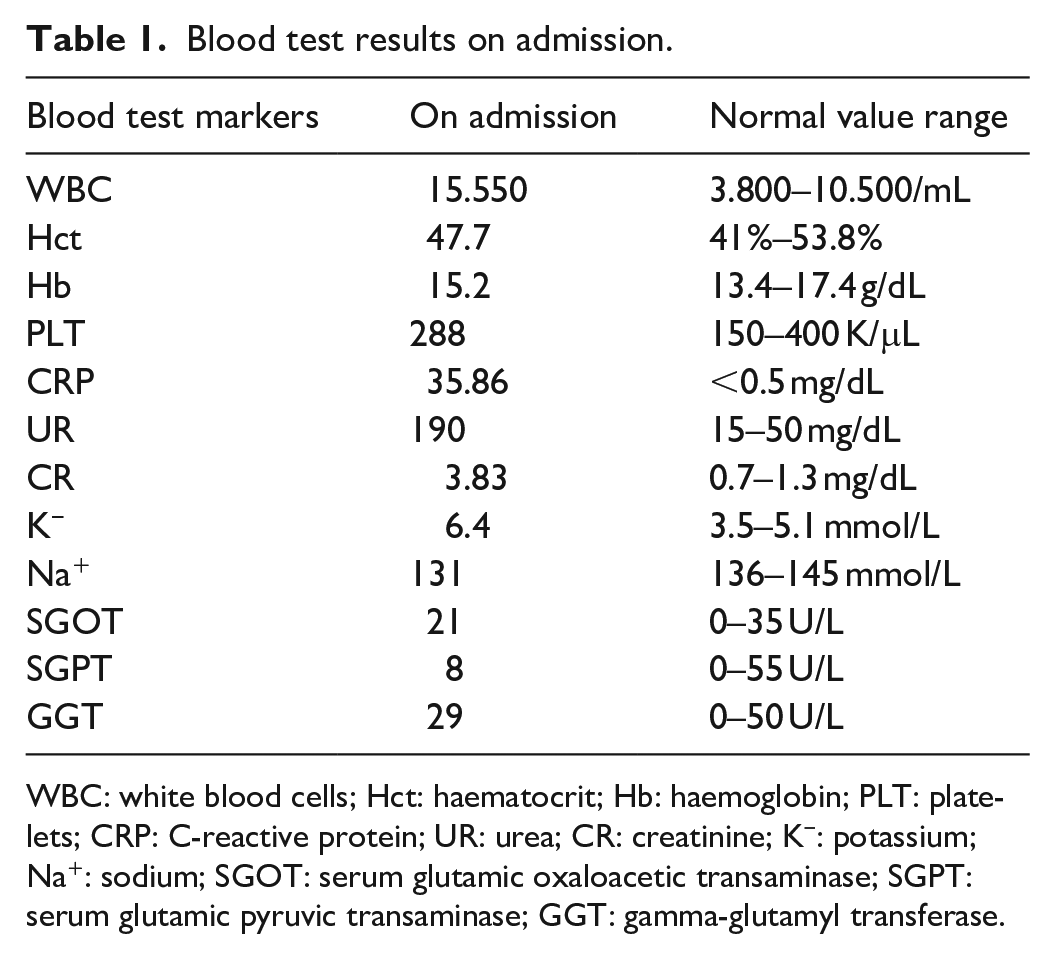
WBC: white blood cells; Hct: haematocrit; Hb: haemoglobin; PLT: platelets; CRP: C-reactive protein; UR: urea; CR: creatinine; K−: potassium; Na+: sodium; SGOT: serum glutamic oxaloacetic transaminase; SGPT: serum glutamic pyruvic transaminase; GGT: gamma-glutamyl transferase.
Taking into consideration the findings from the clinical examination and the blood tests, an abdominal X-ray was performed, revealing distended loops of small intestine, followed by computerized tomography (CT) of the abdomen. The latter detected a gallstone 2.8 cm diameter in the jejunum causing mechanical bowel obstruction (Figure 1) and a cholecystoduodenal fistula (Figure 2).

CT scan of the abdomen depicting a 2.8-cm diameter gallstone in the jejunum causing mechanical bowel obstruction. The arrow demonstrates the gallstone.

CT scan of the abdomen showing abnormal communication between gallbladder and GIT. The arrow demonstrates the cholecystoduodenal fistula.
Due to deterioration of his clinical status, the patient underwent an exploratory laparotomy. Intraoperatively, a 2.8-cm diameter gallstone was recognized provoking intestinal obstruction. Through gentle manipulation, the gallstone was brought proximally to a non-edematous segment of the bowel, and a longitudinal incision was made on the antimesenteric edge (Figure 3). The extraction of the gallstone was followed by a two-layered suture closure of the enterotomy.

Extraction of the gallstone through an incision on the antimesenteric edge of the bowel.
The patient had an uneventful recovery and was discharged on the sixth post-operative day. He was scheduled for cholecystectomy after 2 months. Despite the fact that it was fully explained to the patient the advantages and the possible complications from a second procedure, the patient denied undergoing to cholecystectomy and discontinuation of the fistula. His last follow-up was in September 2022, 8 months after his admission to the hospital, in which he was found in good clinical status and with no signs of ileus or cholangitis.
Discussion
GI is a rare clinical entity mainly affecting the elderly. Its clinical presentation is similar to other types of mechanical ileus, including abdominal distension and pain, nausea, vomiting, dehydration and electrolyte disturbances, making its clinical diagnosis extremely challenging.1–3 In case of intestinal perforation at the site of impaction due to increased endoluminal pressure, symptoms of peritonitis will be predominant. 1
Abdominal imaging is pivotal in confirming the diagnosis of GI. According to Yu et al., 8 CT of the abdomen has sensitivity of 93% and specificity of 100% in diagnosing GI, and is considered the gold standard imaging technique. Abdominal ultrasound is useful to identify cholelithiasis and choledocholithiasis, and in some cases may be able to depict the exact location of the cholecysto-intestinal fistula. 9 Magnetic resonance cholangiopancreatography and endoscopy have also been used in the diagnosis of GI. 2
Surgery is the gold standard treatment for the relief of obstruction in case of prolonged ileus, or failure of conservative management. 1 Preoperative optimization involving GIT decompression, fluid resuscitation and restoration of electrolyte imbalances is prerequisite for any intervention. However, the optimal surgical approach is still debatable and depends on patient’s clinical condition and surgeons’ preference. Three strategies have been described: (1) enterolithotomy, (2) a two-staged approach involving initial enterolithotomy followed by delayed cholecystectomy and discontinuation of the fistula and (3) enterolithotomy combined with cholecystectomy and fistula discontinuation at one stage.1,2
Enterolithotomy is the most commonly performed surgical procedure and is performed either open or laparoscopically.10–12 Enterolithotomy is a relatively straight forward procedure and is preferred in high-risk and unstable patients. 2 The technique involves the formation of a longitudinal incision at the antimesenteric edge of the bowel over the point of gallstone impaction followed by extraction of the gallstone. Bowel resection is necessary in cases of co-existing endoluminal stenosis, intestinal ischaemia or perforation. 2 The main concern in this approach is the preservation of abnormal communication between biliary tree and GIT. Although spontaneous closure of cholecysto-intestinal fistula has been reported in 61.5% of all cases, the remaining fistula has been associated with significant complications such as high risk of GI recurrence, retrograde cholangitis and development of gallbladder malignancy. 13 Alternatively, the two-stage surgical procedure has been proposed. The second intervention is performed electively while the patient has recovered from the initial episode of GI. 12 There is no consensus over the time interval period between enterolithotomy and the second stage of the intervention. 14 In the literature, the interval period between the two operations has been reported in between 4 weeks and 6 months. 14 Nevertheless, a second surgical intervention increases the rate of overall morbidity and mortality, and is increasing the overall cost. 14 Taking into consideration all the above, one-stage surgery has emerged as a promising alternative approach. Enterolithotomy combined with cholecystectomy and fistula discontinuation eliminates the need for reintervention and reduces the incidence of complications related to fistula persistence. 15 However, the intraoperative time becomes prolonged, the repair of fistula is technically demanding, and the rates of morbidity and mortality are higher compared to cases treated only with enterolithotomy; thus, the single-staged procedure is preferred mainly in haemodynamically stable patients with clear indications for biliary surgery. 15 In the literature, all three methods have been used in different cases of GI with excellent results (4–6, 9, 11, 12, and 16–19) (Table 2).
Comparison of cases with gallstone ileus regarding patients’ demographic data, location of gallstone, treatment and outcome.

In our case, we decided to proceed only to enterolithotomy due to patient’s poor clinical status which was a direct consequence of his extensive past medical history. The patient underwent an exploratory laparotomy 4 h after his admission to the hospital, and his comorbidities prevented us from proceeding to single-stage procedure. A single-stage procedure would lead to significant prolongation of the operating and anaesthetic time as well as the complexity of the intervention. We customized our approach based on patient’s clinical status, trying to resolve the obstruction without increasing the risk of possible complications. Although our approach has been described and used successfully in the literature, we would like to highlight that tailoring management on an individual’s base is the cornerstone for a successful outcome.
Conclusion
GI is an uncommon medical condition but may pose a potentially serious health risk. It is crucial for physicians to consider GI as possible cause of small bowel obstruction especially in patients with prolonged history and symptoms of gallstone disease. Repair of cholecysto-intestinal fistula and relief of the obstruction is probably the optimal option in these patients’s management as long as their clinical status allows such an approach.
Footnotes
Author contributions
M.E.F., M.A.M., M.I.G. and E.I.K. analysed and interpreted the patient’s data. The first draft of the manuscript was written by I.G.G. in consultation with A.F.S. and E.S.A. All authors commented on previous versions of the manuscript. A.L., T.G.K. and M.S.C. participated in design and coordination. All authors read and approved the final manuscript.
Availability of data and material
The data sets generated and analysed during this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This case report was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The case report was approved by the Ethics Committee of the Scientific Board of Venizeleio General Hospital of Heraklion (Decision No. 44 /Meeting 8/07-04-2022).
Informed consent
Written informed consent was obtained from the patient. A copy of the written consent is available for review by the Editor-in-Chief of the journal.