
Abstract
We hereby present a 70-year-old male Ethiopian farmer who presented with clinical manifestations suggestive of acute large bowel obstruction, which had persisted for 3 days. Over the past 3 years, he has experienced three similar recurring episodes, which were alleviated by decompression using a rectal tube. Upon initial examination, the patient displayed signs of cardiopulmonary distress, although no indications of peritonitis were observed. Further evaluation through plain abdominal and chest X-rays revealed findings consistent with sigmoid volvulus, as well as mediastinal shift, elevated diaphragm, and a right-positioned heart. Consequently, a sigmoid resection and an end colostomy were done. The patient showed improvement and was discharged from the hospital on the 14th day following the surgery. It is atypical for an individual to present with acute sigmoid volvulus accompanied by a mediastinal shift resulting from mass action on the hemidiaphragm. Therefore, it may be imperative to involve a pulmonologist in managing this rare situation. By ensuring that the surgical team is well-informed in such circumstances, patients can receive enhanced care and treatment.
Introduction
Intestinal volvulus refers to the twisting of the intestine around its blood supply axis. This condition commonly occurs in the sigmoid colon, near the base of the sigmoid mesentery. Sigmoid volvulus is the most frequent type of large bowel volvulus that leads to colonic obstruction. It is particularly prevalent in regions known as the “volvulus belt,” which includes the Middle East, Africa, the Indian subcontinent, Turkey, and South America.1,2 Sigmoid volvulus is a rare cause of intestinal obstruction in children and adolescents and is thought to be an illness of elderly individuals with a widely variable frequency globally. 3
Diagnosing sigmoid volvulus before surgery is usually not challenging, as it exhibits typical clinical signs of large bowel obstruction and specific radiographic abnormalities, particularly in the sigmoid belt regions.4,5 The treatment approach depends on the clinical conditions of the patient upon presentation and intraoperative findings. 6 For uncomplicated cases, the preferred treatment options include endoscopic reduction or emergency rectal tube deflation. However, these methods are temporary and should be followed by elective final surgery. Possible treatment options may involve primary resection and anastomosis, as well as the removal of excess sigmoid colon and Hartmann’s operation.1,7
However, rarely, sigmoid volvulus can have associated atypical findings. In such cases, surgeons, anesthetists, and anesthesiologists can improve their chances of success by having a high level of suspicion and knowledge about the condition. In this particular case, we present a rare occurrence of recurrent sigmoid volvulus in a 70-year-old male patient, which was accompanied by mediastinal shift including heart and respiratory distress.
Case presentation
The patient is a 70-year-old Ethiopian man who presented to the emergency department with clinical features suggestive of bowel obstruction, including abdominal pain, progressive abdominal distension, failure to pass feces and flatus, and three episodes of vomiting, which he had been experiencing for the past 3 days. He had three similar episodes in the last 3 years, all of which were successfully treated with decompression using a rectal tube. However, despite being advised to undergo elective resection after the decompressions, he was unable to do so due to financial constraints. The patient denies any history of rectal bleeding, cough, chest pain, weight loss, or previous abdominal surgery. However, he does experience intermittent episodes of significant constipation.
Upon presentation to the emergency department, the patient exhibited acute signs of illness, appearing visibly distressed and in pain with respiratory difficulties. The recorded vital signs were as follows: blood pressure of 130/80 mm Hg, pulse rate of 92 beats per minute, respiratory rate of 36 breaths per minute, oxygen saturation of 85%, and axillary temperature of 36.2°C.
During the physical examination, it was observed that the patient had a slightly dry tongue and buccal mucosa. Bilaterally decreased air entry was noted in the lower two-thirds of the chest, and cardiac sounds were absent on the left side but audible on the right side with no additional sounds. The abdomen was notably distended and moved with respiration. Percussion revealed a hyper-tympanic sound, and there was no tenderness upon palpation. There was no evidence of fluid collection in the abdominal cavity, and bowel sounds were within the normal range. The rectal examination revealed an empty rectum that was ballooned.
Further diagnostic tests were conducted, including a plain abdominal radiograph, which indicated a sigmoid volvulus, and a chest film, which showed an elevated left hemidiaphragm, a pushed cardiac shadow, and a tracheal shift to the right (Figures 1 and 2). Blood tests yielded normal results. An attempted blind decompression using a rectal tube was unsuccessful (potentially due to the severe nature of the torsion and the exercise of caution during the procedure, given that it is a blind procedure). Consequently, the patient was taken to the operating theater for an exploratory laparotomy after written informed consent was obtained from the patient(s) (for their anonymized information to be published in this article as well).

Preoperative posteroanterior chest X-ray of the patient showed an elevated diaphragm on the left side along with tracheal and mediastinal shift.

Preoperative erect plain abdominal X-ray showing dilated sigmoid colon on the left upper quadrant with a typical coffee bean appearance.
The intraoperative finding revealed a significant and abnormal rotation of the sigmoid colon, which had rotated 360° in a counter-clockwise direction. In addition, the sigmoid colon was greatly distended, causing it to push the left hemidiaphragm upwards and displacing the spleen downwards. This displacement also resulted in the heart being pushed toward the right side, causing the cardiac beat to be visible near the top of the right lobe of the liver. Adhesion was observed between the distended sigmoid bowel and the inferior surface of the diaphragm, as well as the falciform ligament (Figure 3).

Intraoperative findings showed a viable and significantly dilated sigmoid colon.
To address these issues, the adhesion was carefully released using a sharp dissection. The volvulus was then de-rotated, and a resection of the redundant sigmoid colon was performed, along with a Hartmann’s procedure. During the procedure, the cardiac beat gradually returned closer to the midline after the distended segment of the colon was removed. The resected sigmoid colon, which measured 15 cm in diameter and 80 cm in length, was sent for histologic examination.
Postoperatively, the patient was transferred to a post-anesthesia recovery unit for monitoring, given maintenance fluid, and continued antibiotic treatment. One hour after the operation, the patient’s oxygen saturation dropped to 80% with room air, and he experienced rapid breathing (50 breaths per minute), which persisted until the fourth postoperative day. A pulmonologist was consulted and considered the possibility of re-expansion pulmonary edema, which was managed conservatively with intranasal oxygen support. On the fourth postoperative day, the patient developed a productive cough and a low-grade fever, leading to a revision of the antibiotics to cover hospital-acquired pneumonia. Therefore, intravenous vancomycin and ceftazidime were initiated.
On the fourth postoperative day, the patient passed feces, and an oral diet was started. The productive cough, rapid breathing, and oxygen desaturation gradually decreased until the tenth postoperative day. Postoperative echocardiography revealed dextrocardia, but no valvular or other pathologies were observed. Chest films showed bilateral lung expansion, the cardiac shadow closer to the midline, and the trachea in a central location. However, an abnormally elevated left hemidiaphragm was noted until the time of discharge, with slight improvement seen in subsequent chest films. Unfortunately, comparing the current films with the previous chest X-ray was not possible since our patient did not have any studies before (Figures 4 and 5).
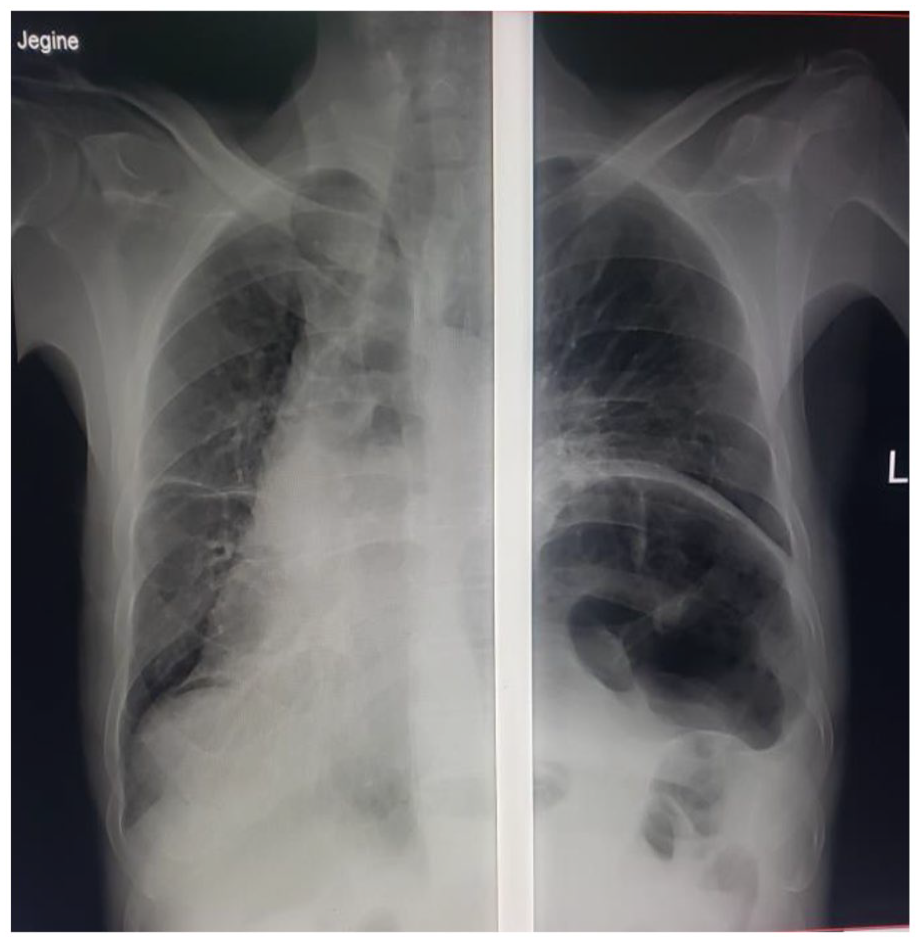
Chest X-ray of the patient on the first postoperative day showed improvement in the mediastinal and tracheal shift.
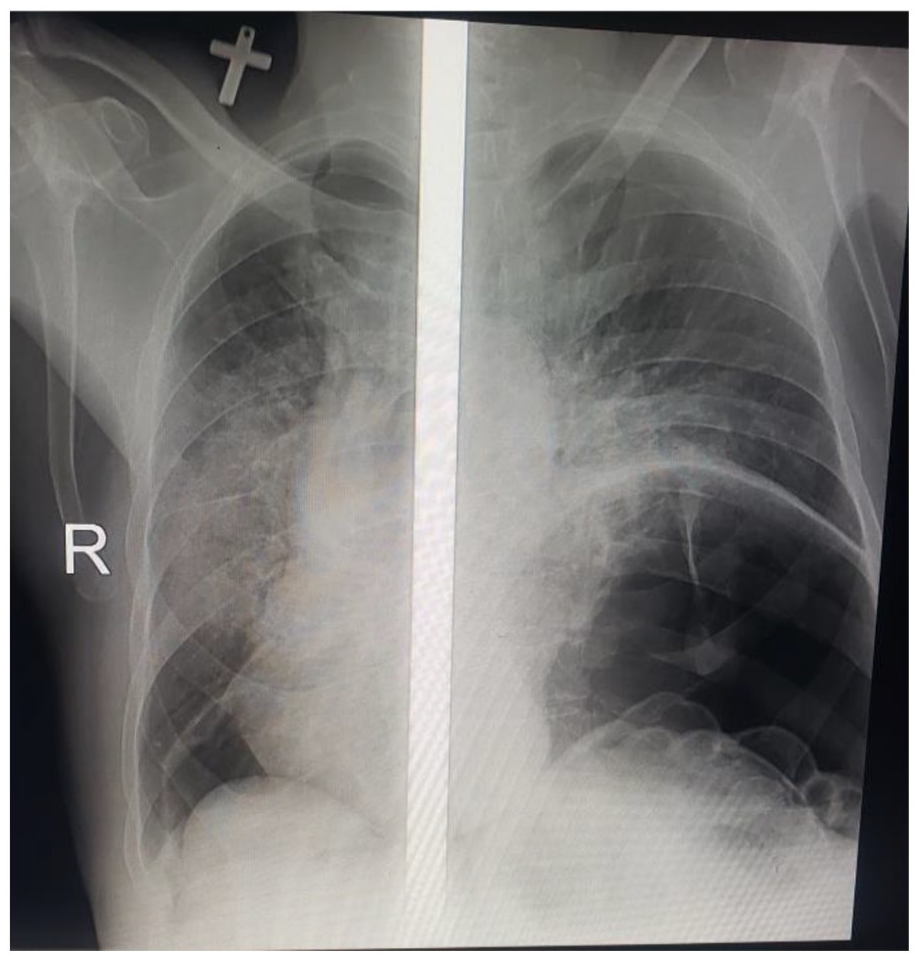
Chest X-ray of the patient on the seventh postoperative day showed significant improvement from the previous findings.
The patient made good progress and was discharged on their 14th postoperative day, with a follow-up appointment scheduled for 2 weeks later. At the appointment clinic on the 28th postoperative day, the patient had no complaints except for mild discomfort around the wound site.
Discussion
Sigmoid volvulus remains an important cause of large bowel obstruction in the elderly population, particularly in the region known as the “Sigmoid Belt.” 1 The development of the volvulus is influenced by the anatomical dimensions of the sigmoid colon. However, some studies have failed to account for the confounding influence of acute sigmoid obstruction on these dimensions. One study suggests that individuals with a long sigmoid colon and a long mesentery with a narrow base are at a higher risk of developing sigmoid volvulus. 8 Other factors, such as Hirschsprung disease, neurologic disorders, prolonged constipation, or megacolon, can also contribute to the occurrence of sigmoid volvulus. 9
The literature has put forth a diverse array of classifications of sigmoid volvulus, which include the following: torsion direction, torsion degree, clinical course, severity, and prevalence. Torsion direction can be categorized as either clockwise or counterclockwise. Torsion degrees can be further classified as less than 360°, exactly 360°, or greater than 360°. The clinical course can be described as acute, subacute, or chronic. Severity can be distinguished as either complete or partial. Lastly, prevalence can be characterized as sporadic or endemic. 10 The case we discussed involved an acute sigmoid volvulus, which rotated 360° counter-clockwise over its mesentery.
The patient’s functional condition, the timing of the surgery, the illness stage, and their cooperation with the physicians throughout the preoperative decision-making process all have a significant impact on the mortality rate associated with sigmoid volvulus. 11 Various imaging studies can assist in the planning stage of the surgery as well. While X-rays can provide valuable information, their two-dimensional images have certain limitations. To conduct a comprehensive assessment of a patient, computed tomography (CT) is often employed. CT scans allow for the examination of all tissues, including tumors, as well as the identification of reasons for displacement, skeletal and anatomical abnormalities, and other relevant factors. 12
Imaging studies conducted on our patient, which included an X-ray, revealed a significant elevation of the diaphragm, accompanied by a shift of the mediastinum including the heart and trachea to the right. This was observed in addition to the presence of sigmoid volvulus. Generally speaking, external factors, such as intrathoracic conditions like tension pneumothorax and masses that exert pressure on the trachea and mediastinum, are commonly responsible for inducing tracheal deviation and mediastinal shift. 12 However, although uncommon, another possible cause for deviation could be the elevation of the diaphragm due to abdominal causes, as seen in the presented case.
The treatment approach for sigmoid volvulus varies depending on the patient’s condition and clinical appearance. Once the patient has been adequately resuscitated, treatment options can range from a simple tube or sigmoidoscopic decompression to more extensive surgical intervention in emergency or elective situations. 13 The choice of treatment will depend on factors such as the patient’s age, surgical findings, and hemodynamic condition. Surgical options may include derotation of the sigmoid colon, removal of the gangrenous segment with restoration of bowel continuity, or the creation of a Hartmann’s colostomy.14,15 In our case, resection of the significantly enlarged, edematous sigmoid colon was done along with Hartmann’s procedure after adequate resuscitation.
The patient’s postoperative decrease in oxygen saturation was likely caused by re-expansion pulmonary edema, as his echocardiographic evaluation revealed only a displaced heart on the right side of the chest. This condition, although somewhat uncommon, occurs when a collapsed lung is rapidly re-inflated. The underlying pathophysiology involves mechanical stress during re-expansion and abnormalities in the histology of pulmonary microvessels.16,17 To address this condition, the patient received symptomatic treatments. Fortunately, these interventions led to a positive outcome, and the patient’s condition improved.
Key clinical message
This case underscores the infrequency of acute sigmoid volvulus with mediastinal shift, underscoring the imperative for heightened awareness among medical professionals. Furthermore, it accentuates the necessity for a multidisciplinary approach in the management of such cases.
Conclusion
The case we have presented is an exceptional occurrence of acute sigmoid volvulus in a 70-year-old male patient, resulting in a mediastinal shift due to a mass effect on the hemidiaphragm. The rarity of this sigmoid volvulus presentation presents challenges during surgery and may lead to postoperative complications related to the mass effect on the cardiopulmonary system. In managing such a unique scenario, a multidisciplinary approach is necessary. Increasing awareness among the operating team regarding such cases could potentially enhance overall patient outcomes.
Footnotes
Acknowledgements
The author would like to acknowledge and for involving in overall patient management and taking intraoperative images.
Author contribution
M. O. Y. manuscript draft writing, and revision; M. A. A. manuscript draft writing, and involved in the management of the patient; H. T. A. manuscript revision and approval; Y. D. M. revision, involved in the management of the patient and submission.
Availability of data and materials
All the images and detailed information of this case are available at the University of Gondar Comprehensive Specialized Teaching Hospital patient record.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.