
Abstract
Enterolithiasis is an uncommon entity in humans but frequently seen in equine mammals. A primary enterolith is a mineral concretion formed within the gastrointestinal tract due to the alteration in the anatomical integrity due to variety of conditions resulting in intestinal stasis. We report a patient with small intestinal obstruction due to a primary enterolith. A 65-year-old woman presented to the emergency department with central colicky abdominal pain, absolute constipation followed by vomiting. An enterolith located in distal ileum causing small intestinal obstruction was established with the aid of abdominal X-ray radiograph and computed tomography. Exploratory laparotomy was performed to extract the enterolith and to resect a strictured proximal jejunal segment which was suspected to be the original site of enterolith formation. Chemical analysis of the enterolith supports the speculation of a proximally formed primary enterolith eventually migrating to the site of impaction in the terminal ileum.
Introduction
Primary enterolithiasis is uncommon in humans and is generally formed in the setting of intestinal stasis. This entity is a commonplace in animals, such as horses and zebras. 1
Enteroliths are usually asymptomatic, detected in the abdominal radiographs. Rarely, it may lead to complications including intestinal obstruction, perforation, or bleeding. We report a case of primary enterolithiasis causing small intestinal obstruction, in which the diagnosis was established by the abdominal X-rays and computed tomography.
Case
A 65-year-old woman was admitted to the emergency department with colicky, non-radiating central abdominal pain, and nausea for 5 days. She had not passed stools over this period. Her symptoms worsened over the last few hours associating with bilious vomiting. She denied having fever, urinary symptoms, constitutional symptoms, features suggestive of inflammatory bowel disease, or contact history of tuberculosis. Two months prior, she had undergone an attempted open vesicolithotomy when she developed a similar but less severe episode of abdominal pain. She was on antianginal medication for ischemic heart disease.
She was afebrile, neither pale nor icteric. Abdominal examination revealed a distended abdomen with generalized tenderness without guarding or rigidity. There was no hernia, organomegaly, or masses in the abdomen. Her bowel sounds were exaggerated. She was tachycardic but normotensive.
Laboratory investigations including complete blood count, C-reactive protein level, and urinalysis were unremarkable. An abdominal X-ray revealed a dilated small bowel with an opaque ovoid density showing multiple concentric layers in the lower abdomen. Contrast-enhanced computed tomography revealed a calculus in the ileum without pneumobilia, gallstones, or cholecystoenteric fistula (Figure 1).

(a) X-ray abdomen (lateral) demonstrating the enterolith with multiple concentric layers and (b) computed tomography demonstrating the radiodense enterolith.
An exploratory laparotomy was performed with a mid-line incision. An obstructing calculus in the distal ileum was observed after vertical enterotomy was performed. There were two strictures one foot apart in the proximal jejunum without macroscopic evidence of chronic intestinal inflammation (Figure 2). After closure of enterotomy, the calculus was sent for chemical and infrared analyses. Segmental resection of the small intestine with strictures was performed after ligating and dividing the mesenteric blood vessels and dividing the small intestine between bowel clamps. End-to-end hand sawn small intestinal anastomosis was created with single-layer interrupted stitches using 3-0 polydioxanone sutures. Mass closure of laparotomy was performed after leaving an abdominal drain. The patient made an uneventful recovery, the abdominal drain was removed on postoperative day 3 and was discharged on postoperative day 5. Histology of the resected bowel segment with strictures revealed nonspecific inflammatory changes. The patient was discharged from the clinic follow-up 3 months after the operation, as she continued to be free of symptoms.
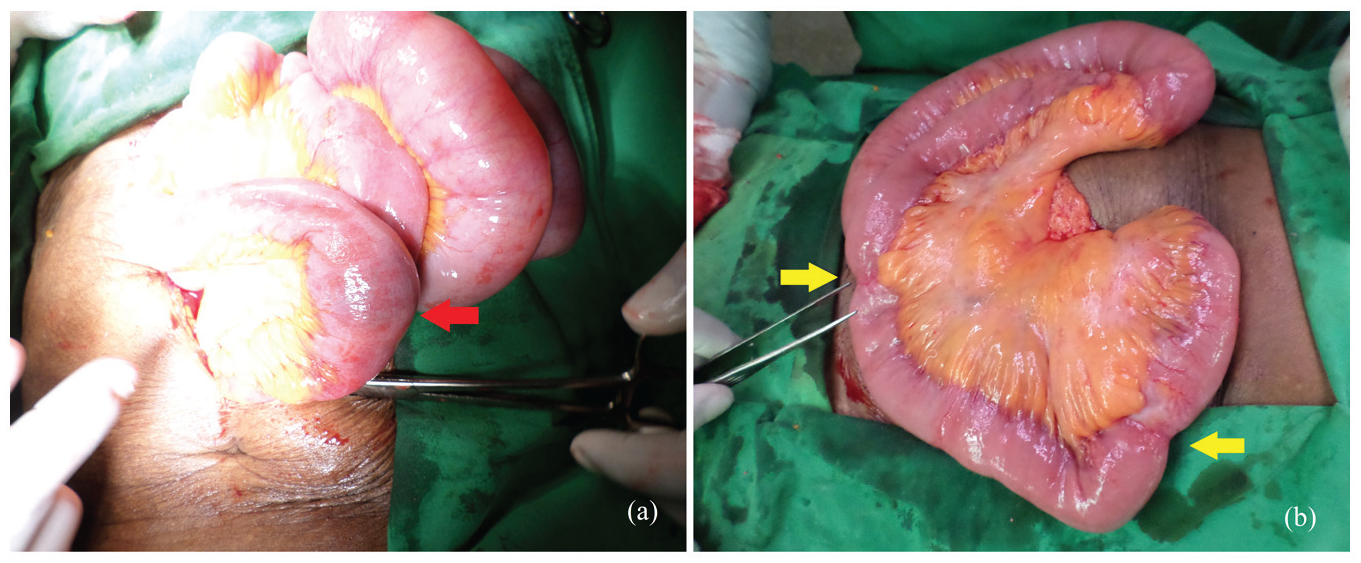
(a) Obstructing enterolith in the distal ileum and (b) a couple of strictures located one foot apart in the proximal jejunum.
Stone analysis
The cross-section showed a characteristic concentric layered appearance formed around an oblong-shaped center filled with gel-like material (Figure 3). Chemical analysis was conducted according to layers. Calcium oxalate and magnesium phosphate were the most abundant chemical compounds found mainly in outer layers. Inner layers contained cholic acid and a scanty amount of bilirubin. Infrared analysis of the calculus revealed 60% w/w of calcium oxalate dehydrate.

Cross-section of the enterolith demonstrating characteristic concentric layers formed around an oblong-shaped center filled with gel-like material.
Discussion
An enterolith is a mineral concretion in the gastrointestinal tract and has a reported prevalence varied from 0.3% to 10%. The true prevalence is unknown as most cases are only identified in symptomatic patients. Gender and age predilection of enterolithiasis generally reflect the epidemiology of the underlying etiology of the disease that predisposed to the formation of enteroliths. Enterolithiasis can be primary or secondary. Secondary enteroliths are formed in the organs outside the gastrointestinal tract (e.g., gallbladder, urinary system) that have migrated into the gastrointestinal tract as a result of fistulation. There was no radiological or intraoperative evidence of cholecystitis or cholecystoenteric fistula in our patient.1,2
Primary enteroliths form within the gastrointestinal tract due to an alteration in anatomical integrity resulting in intestinal stasis. This may be a result of congenital or acquired conditions (e.g., diverticular disease, meconium, Crohn’s disease, intestinal tuberculosis, intestinal fistula, and incarcerated hernias), postsurgical changes (e.g., blind pouches, adhesions, afferent loops, and enteric anastomoses), or rare conditions with abnormal intestinal motility (e.g., intestinal aganglionosis or ischemic enteritis). Our patient had two proximal intestinal strictures with nonspecific inflammation which might have been the cause for intestinal stasis. Long-term consumption of dietary calcium has been evaluated as a cause for enterolithiasis, but remains controversial.3–8
True primary enteroliths are result of precipitating substances in chyme. False primary enteroliths are formed when the minerals are deposited in concentric layers around the insoluble foreign substances in the gastrointestinal tract (e.g., bezoars, varnish, or insoluble salts).1,9
The chemical composition of the enteroliths provides evidence of the site of the origins and site of stone formation and the final site of impact. The most common form of secondary enterolith is gallstones composed of cholesterol and bilirubin. Furthermore, cholic acid precipitates in lower pH which is found typically in the proximal small intestine. Calcium salts precipitate in the alkaline pH and thus mostly formed in the terminal small intestine. Our stone analysis demonstrated the presence of cholic acid in the inner layers and calcium and magnesium salts in the outer layers reflecting the site of the formation at the proximal jejunal strictures with subsequent migration to the distal ileum. 9
Most enteroliths are asymptomatic. Clinical presentation of enteroliths depends on the location and the dimensions of the enterolith. Some may present with subacute episodes of colicky abdominal pain, nausea, and vomiting due to the propagation of the enterolith through the intestinal lumen. The most frequent complication of enterolith is intestinal obstruction followed by gangrene, perforation, bleeding, intussusception, and iron deficiency anemia. Colicky abdominal pain is the commonest symptom. Absolute constipation and abdominal distension precede vomiting in the distal obstruction similar to our patient, but the opposite occurs in the proximal obstruction. A clinical diagnosis of enterolithiasis is challenging due to the rarity of the condition and the nonspecific nature of the clinical features. The differential diagnoses for bowel obstruction can be extramural (e.g., adhesions, and hernia), mural (e.g., inflammatory conditions, strictures, and tumors), or intraluminal causes (e.g., foreign bodies, parasites, and bezoars). Intestinal colic due to enteroliths may be misinterpreted as symptomatic calculi in the urinary tract clinically as well as radiologically as in our patient. A background history of a condition causing long-term intestinal stasis should raise the suspicion.1,3,10
The visibility on plain abdominal X-rays depends on the calcium content of the enteroliths. The distally located enteroliths are more abundant with calcium salts and are more radiopaque. The enterolith of our patient demonstrated a layered appearance different from the commonly described as “coin-on-end” appearance. Other extraluminal calcific pathologies including ureteral stones, fecaliths, omental calcifications, calcified fibroids, and lymph nodes can mimic enteroliths. Computed tomography with oral contrast may reveal the radiolucent proximal enterolith as a void. Apparent mobility in an abdominal series is another strategy to differentiate enteroliths from the mimickers when the diagnosis is doubtful. The sensitivity of ultrasonic imaging is hindered by the presence of intestinal gas.11,12
The treatment options include removal of the enterolith and treatment of underlying etiology to prevent a recurrence. Expectant management has a limited place and has been reported for symptomatic enteroliths <2 cm without luminal compromise such as strictures or obstruction. The mainstay of treatment is open surgery with the enterolithotomy and manual removal. Although several successful laparoscopic surgeries have been reported, this approach is limited when the complexity of the unestablished etiology for intestinal stasis remains unclear. Endoscopic electrohydrolic lithotripsy has been successful in some cases. To prevent stone recurrence, the underlying pathology for the compromised intestinal motility should be treated accordingly with medical (e.g., inflammatory and infective), endoscopic (e.g., dilatation of strictures), or surgery (e.g., stricturoplasty, segmental bowel resection) to prevent further formation of enteroliths. Mortality of primary enterolithisis is low but can rise to 3% due to underlying conditions with poor prognosis, frailty in elderly patient, and missed or delayed diagnosis.13–15
Conclusion
Alterations in bowel motility and microenvironment of the intestine including pH level play a significant role in the pathogenesis of enteroliths. Clinical presentation ranges from intestinal colic, intestinal obstruction, gangrene, perforation, bleeding, or iron deficiency anemia. Clinical diagnosis of enterolithiasis is challenging but may be aided by radiological studies.
The treatment should aim to eliminate the enterolith and correct underlying pathology to prevent additional stone formation. Chemical analysis of an intestinal stone shows stone composition which can guide treatment and give information regarding the etiology and may prevent more stone from forming.
Footnotes
Acknowledgements
None.
Author contribution
MEK conceived the idea of reporting this case, GPUS and MEK were involved in the management of the patient data collection and interpretation, MEK and GPUS wrote the manuscript, MEK and BGNR modified the manuscript, and all authors approved the final version for manuscript.
Availability of data and materials
All data used to support the findings of this study are included within the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for anonymized information to be published in this article.