
Abstract
Madelung deformity is a congenital disorder with the malformation of anterior ulnar bowing of radius and a dorsally protruding ulnar head caused by premature growth disturbance at the medial volar aspect of the distal radius. This report describes a bilateral idiopathic Madelung deformity in a 17-year-old woman treated successfully using reverse wedge osteotomy of the distal radius in a symptomatic left wrist. Reverse wedge osteotomy can orient the radial joint surface while correcting the whole radius length by reversely putting the wedge bone removed from the distal metaphysis of radius, the base of which is cut from the surplus of the radial and dorsal cortical bone in the hypotrophic portion. We corrected the palmar subluxation of the carpus, restored her good function, and relieved her wrist pain.
Introduction
Madelung deformity, described originally by Otto Wihelm Madelung in 1878, results from a growth disturbance of the volar ulnar components of the distal radius with a prevalence of less than 0.03%.1,2 It is commonly observed in girls in early adolescence and is diagnosed at the onset of wrist pain and restriction of the forearm and wrist range of motion and skeletal deformity such as anterior ulnar bowing of the distal radius and prominence of the distal ulna and.1,2 In terms of a genetic basis, Madelung deformity is the most distinctive feature in patients with short stature homeobox (SHOX) gene deficiency such as Leri Weill dyschondrosteosis. 3 The radiographic features of Madelung deformity include ulnar and dorsal arcuation of the distal radius, increment inclination of the distal radius joint surface, triangulation of the carpus with proximal and volar migration of the lunate, and protruding dorsal subluxation of the ulnar head. 4 True Madelung deformity with an anomalous radiolunate ligament (Vickers ligament) 5 can be differentiated from Madelung-type deformities by post trauma and infection and osseous dysplasias without Vickers ligament. 2 This ligament, which seems to be the key factor allowing the progression and development of Madelung deformity including the less common entire radius variant, 6 was described by Vickers and Nielsen first. 5 Various surgical procedures to treat Madelung deformity have been reported. 7 Lengthening of the radius, shortening of the ulna, or a combination of both as the approaches for surgical correction of Madelung deformity have been preferred by surgeons. 7 Especially, surgical osteotomy techniques with volar locking plate fixation were reported to have stable corrective power.8 –11 Reverse wedge osteotomy, described first by Dagrégorio et al., was evolved to reorient the radial joint surface while correcting the overall radius length and reversing a bone wedge removed from the distal metaphysis of the radius, with a base cut from the surplus of the radial and dorsal cortical bone and a vertex in the hypotrophic area.8,9 This report describes a 17-year-old female high school student with Madelung deformity who was treated successfully using reverse wedge osteotomy.
Case report
A 17-year-old woman whose chief complaint was left wrist pain on the dorsal and ulnar side and anomalous appearance of the left wrist, presented at our institution. She was informed about deformity of her left forearm by a school physician when she was a junior high school student. However, she did not visit the hospital because her left wrist was asymptomatic. She had scoliosis (left thoracic–lumbar scoliotic curve extending from Th11 to L4 with apex at L1, measured as about 12° using Cobb method). No one in her family has this variant.
As a participant in a high school Japanese drum club, she often had wrist pain after playing the drums. Her wrist pain of the ulnar side had worsened gradually during activities of daily life, such as when opening a bottle lid. At first presentation, her wrist and hand translated the volar side relative to the longitudinal axis of the forearm; the ulnar head projected dorsally (Figure 1(a) and (b)). Clinical examination revealed that she had deep pain by pressure of the dorsally protruding ulnar head on the left side. However, she had not complained of any symptom in the right wrist. The posteroanterior and lateral radiograph of left wrist showed a 30° ulnar tilting angle, 5.7 mm lunate proximal subsidence and a distal radial notch and 50° palmar tilt angle (Figure 2(a)). On the right side were a 53° ulnar tilting angle, 2.0 mm lunate proximal subsidence and no distal radial notch and 80° palmar tilt angle (Figure 2(b)).

(a) The left hand appears to be mildly hypoplastic compared to the right hand. (b) Dorsal bowing of the forearm and dorsal prominence of the ulnar head.
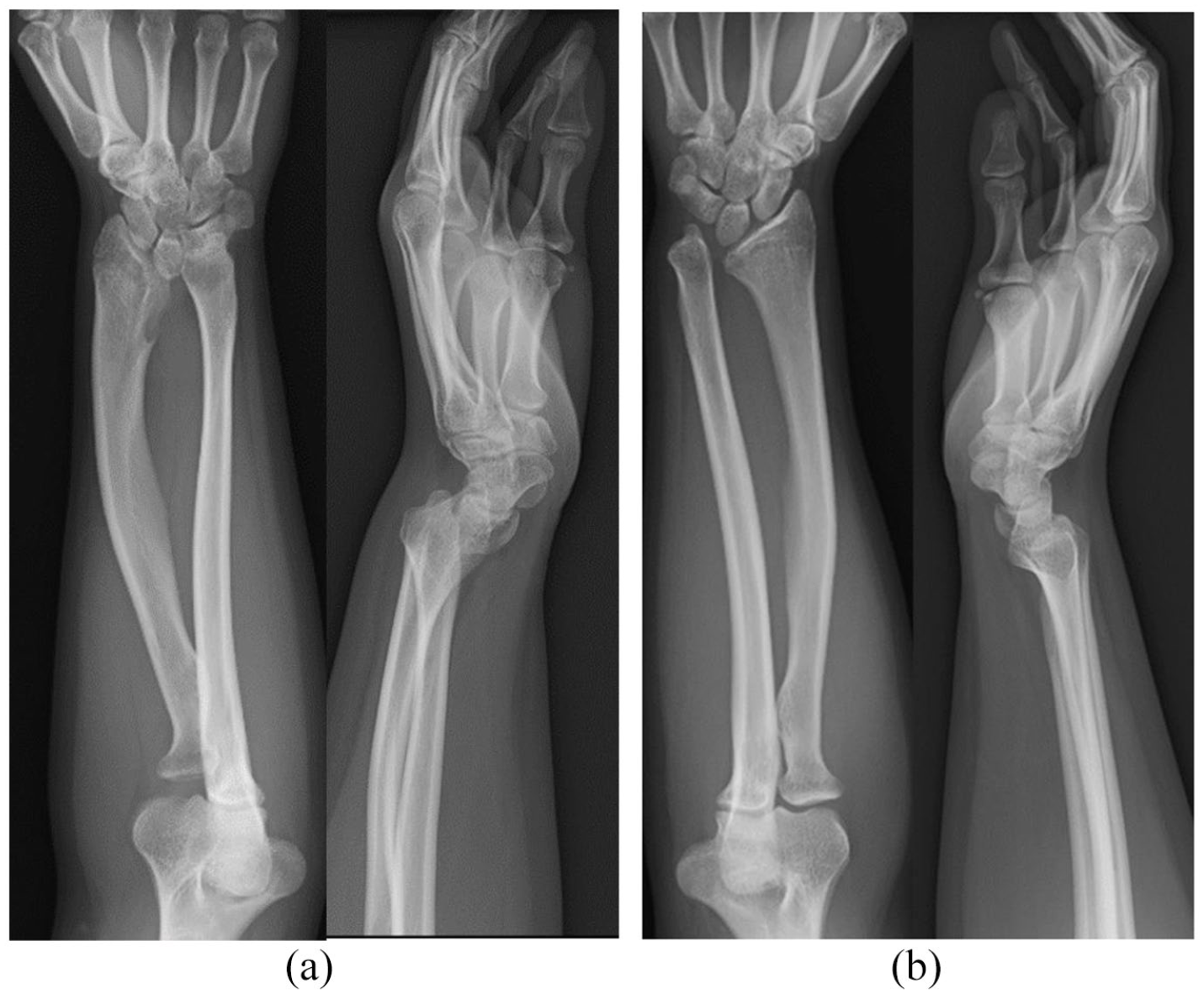
(a) Posteroanterior radiography showed 30° ulnar tilting of the distal articular surface of the radius and 5.7 mm lunate proximal subsidence and a distal radial notch in the left wrist. Lateral radiography showed 50° palmar tilting of the distal articular surface of the radius in the left wrist. (b) Posteroanterior radiograph showed 53° ulnar tilting of the distal articular surface of the radius and 2.0 mm lunate proximal subsidence and no distal radial notch in the right wrist. Lateral radiograph showed 80° palmar tilting of the distal articular surface of the radius in the right wrist.
Left wrist extension and flexion were, respectively, 45° and 60°. Forearm pronation and supination were 90° and 90° (right side wrist extension and flexion were 60° and 60°, with forearm pronation and supination of 90° and 90°). Scores of QuickDASH of Japanese version and Hand 20 at the first visit were, respectively, 79.5 and 81. The Japanese version of QuickDASH has equivalent evaluation capacities to those of the original version. 12 Hand 20, a self-administered comprehensive measure, comprises 20 questions with illustrations intended to identify upper extremity symptoms and capability to perform certain activities. The response to each question was rated using a 0–10 Numeric Rating Scale. The points are added up to produce a total score (minimum 0, maximum 100). A higher total score is related with worse upper extremity function. Suzuki et al. verified Hand 20 reliability and validity. 13 Grip strength of the left side was 20.7 kg (right side, 29.3 kg).
We diagnosed the patient as having bilateral Madelung deformity and instructed her to stop heavy use of her left wrist such as hitting the Japanese drum, heaving and lifting heavy luggage, and push-ups. Moreover, we administered conservative treatment with a wrist brace. Her ulnar wrist pain worsened during activities of daily life. Therefore, we planned a corrective osteotomy.
Surgery planning
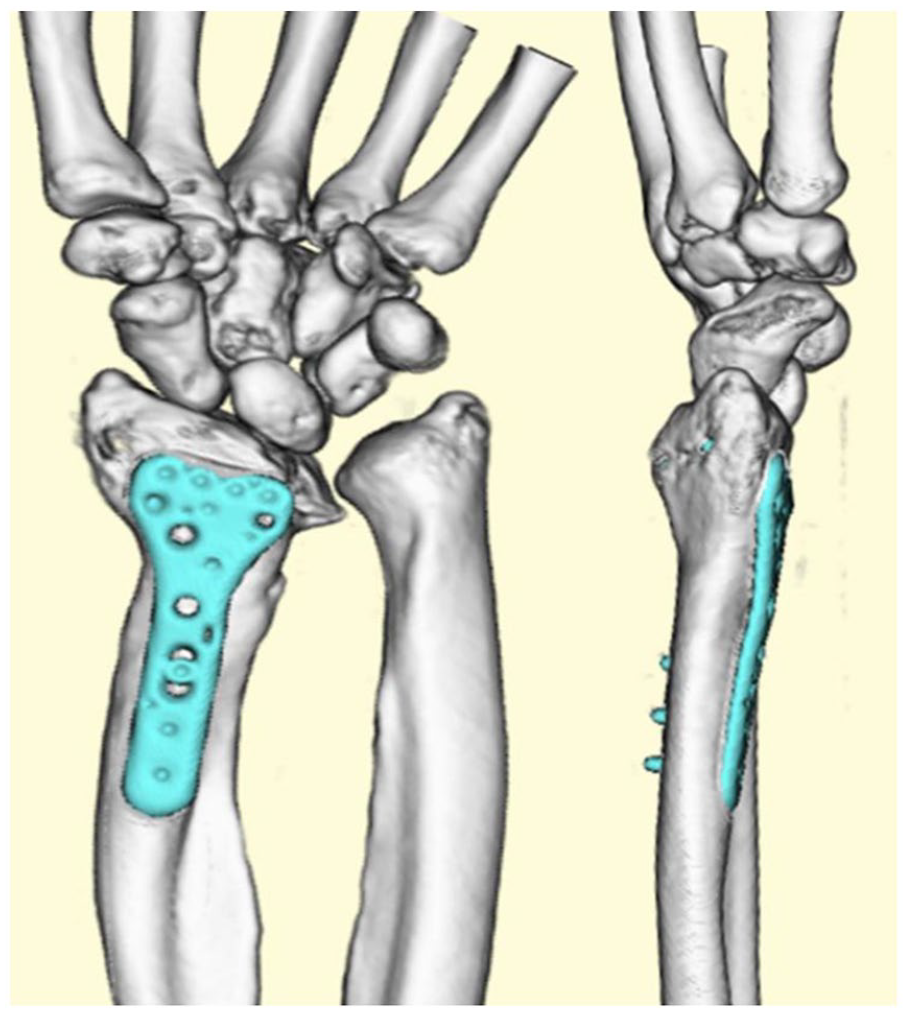
Based on data obtained using preoperative three-dimensional (3D) computed tomography (CT), we simulated and planned to resect the wedge bone manually with an angle of the apex of the wedge of 20° and to reverse it into the bone cutting site for correcting the radial inclination and dorsal tilt (Figure 3).

It was planned that the wedge bone with an angle of the apex of the wedge of 20° should be resected from the distal metaphysis of radius and be put reversely into the bone cutting site to correct the radial inclination and dorsal tilt.
Surgical procedure and intraoperative findings
An approach was made through the flexor carpi radialis sheath. Vickers ligament arising from the ulnar metaphysis of radius was found and released after we reflected the pronator quadratus to the ulnar side (Figure 4(a)). Aiming for an angle of the apex of the wedge of 20°, we cut parallel to the wrist joint surface in the metaphysis of radius at the proximal portion of the Lister tubercle and cut perpendicular to the longitudinal axis of the radius (Figure 4(b)). After cutting out the wedge bone (Figure 4(c)), it was reversed into the bone cutting site to obtain closure on the excess and opening on the deficient cortical bone with applying distraction force in the peripheral direction, and to ensure perfect contact of the bone section surfaces to correct the radial joint surface (Figure 4(d)). Reduction is maintained by an oblique 1,5 mm diameter wires. Fixation was ensured using locking screws with the locking plate (Stellar2; Hoya Technosurgical Corp., Japan), bent convexly on the palm side to maintain the correction angle. Postoperative radiography of the wrist joint revealed the ulnar tilting angle, lunate proximal subsidence and lunate fossa angle, palmar, volar tilt angle, and palmar carpal displacement (Figure 5). At the 23-month follow-up, the patient reported no further pain; wrist extension and flexion were, respectively, 70° and 80°; and forearm pronation and supination were, respectively, 90° and 90°. The grip strength of the left hand improved to 28.1 kg. The QuickDASH and Hand 20 score improved, respectively, to 0 and 0. Radiographs demonstrated bone maturation during this time (Figure 5). Postoperative three-dimensional CT revealed that ulnar tilting angle, lunate proximal subsidence, and palmar tilt angle improved, respectively, from 30° to 60°, and 5.7 mm to 1.2 mm and 50° to 79° (Figure 6). Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.

(a) Thickened Vicker ligament was identified. (b) A circumferential bone wedge with the base taken from the excess radial and dorsal cortical was performed. (c) Resected wedge bone. (d) The bone wedge taken from the distal was placed reversely; the overall radius length was reduced.

X-ray immediately after surgery showed improvement based on McCarroll’s radiologic parameters.
Three-dimensional CT at the 28-month follow-up showed bone union and the retention of improvement of McCarroll’s radiologic parameters.
Discussion
We performed the reverse wedge osteotomy to correct Madelung deformity for a 17-year-old woman with wrist pain on the dorsal and ulnar side. Thereby, we achieved clinical good outcomes and achieved patient satisfaction. This surgical procedure reported by Dagrégorio associates subtraction from the surplus and addition to the deficient cortical bone, providing incomparable three-dimensional corrective power.8,9 Mallard et al. described significant improvement on McCarroll’s five radiologic parameters 4 for Madelung’s deformity assessment in 11 wrists in 6 adult female patients who had undergone operations using this procedure. 9 However, various surgical procedures for correcting Madelung deformity, relief of wrist pain, and improvement of wrist or hand function have been reported. 7 Vickers and Nielsen resected an abnormally thickened volar ligament (Vickers ligament), which tethered the lunate to the radius and which interposed fat to prevent recurrence of a bony bridge, thereby enabling radius growth in a more normal fashion for younger patients with anticipated remaining growth potential. 5 Prior studies demonstrated the association between the classification of Madelung deformity and the presence of Vickers ligament. 2 Ali et al., reported that true Madelung deformity with Vickers ligament in patients with Leri Weill dyschondrosteosis can be differentiated from Madelung-type without Vickers ligament arising from trauma or multiple hereditary exostoses. 2 Farr et al., found the significant association with the presence of Vickers ligament and the radiographic findings such as a distal radial notch and a more severe entire radius variant in a retrospective multicentre study of 75 surgical cases. 6 In our case with whole bone Madelung’s deformity, we found a distal radial notch in the preoperative radiograph and observed this ligament intraoperatively in line with Farr’s results.
Radial closing or opening osteotomy with or without ulna shortening has been performed exclusively in many cases. 7 Earlier studies have demonstrated a distal radius dome osteotomy with resection of Vickers’ ligament, preserving radial length and correcting the radial joint surface in three planes as an effective corrective procedure. 11 Acciaro et al., reported the usefulness of a small volar locking plate fixation for reverse dome osteotomy of the distal radial epiphysis, which is reversing the shape of the classical dome osteotomy and allowing for the multiplanar correction, in 13 pediatric patients with the common distal radius variant. 11 They achieved clinical good outcomes and wrist pain relief in all patients in midterm follow up. 11 We used the standard volar locking plate fixation for revers wedge osteotomy in the patients with closed epiphyseal line of the distal radius. The non-invasive fixation technique with a small volar locking plate may be useful for revers wedge osteotomy on the peripheral side of the epiphyseal line so as not to damage the epiphyseal line in pediatric patients with Madelung deformity.
Recently, corrective osteotomy with developed 3D simulation technology has been reported. Imai et al. and Yanagisawa et al. produced customized surgical guides designed by preoperative 3D computer simulation and performed cylindrical corrective osteotomy of the distal radius.10,14 They reported good outcomes in applying 3D corrective osteotomy. However, this computer simulation technology is not always possible in many hospitals.
Furthermore, Megremis et al. reported good performance of corrective surgery using the Taylor spatial frame external fixation system for a 13-year-old girl with bilateral Madelung deformity. 15 This hexapod system, which is supported with web-based software programs, enables for the simultaneous correction of all components of multiplanar limb malformation with minimization of the time required for deformity correction compared with the conventional Ilizarov technique. However, it might be complicated if a surgeon were not accustomed to the conventional Ilizarov technique. Reverse wedge osteotomy seems to be apparently technically simpler without a forced maneuver or remote bone harvesting for the patients with Madelung deformity.
In the surgical management of Madelung deformity, a lack of evidence-based algorithms regarding the surgical decision-making process remains, however, various surgical treatments have satisfactory outcomes. 7 Peymani et al., suggested the data collection template of surgical outcomes of Madelung deformity to increase the homogeneity and evidence equality of the surgical outcome of a variety procedures. 7 Further studies should be needed to create the clinical guidelines regarding the surgical decision-making process of Madelung deformity.
Conclusion
This report describes performance and effects of reverse wedge osteotomy to correct Madelung deformity in a 17-year-old female student with wrist pain on the dorsal and ulnar side. She was satisfied with the good clinical outcomes we achieved. We regard this osteotomy as one effective corrective procedure for patients with Madelung deformity.
Footnotes
Acknowledgements
We would like to thank Atsuhito Seki MD, PhD, and Takehiko Takagi, MD, PhD of Department of Orthopedic Surgery, National Center for Child Health and Development for their invaluable comments related to the surgical treatment used for this case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.