
Abstract
Selective wrist denervation is a surgical technique frequently performed for the treatment of chronic wrist pain. While this technique is often effective in pain reduction, it is still associated with certain complications such as pain recurrence secondary to neuroma formation. We present a case report that details the clinical case of a young yoga teacher suffering from debilitating chronic wrist pain, refractory to conservative treatments. We describe a new surgical technique for the treatment of chronic wrist pain: posterior interosseous nerve and anterior interosseous nerve neurectomy followed by neurorrhaphy in preventing neuroma formation. Post-operatively, the patient’s wrist pain continuously improved and completely resolved without any signs of recurrence. Posterior interosseous nerve and anterior interosseous nerve neurectomy followed by an end-to-end neurorrhaphy can be used as an effective novel surgical technique in the management of chronic wrist pain with prevention of neuroma formation.
Keywords
Introduction
Chronic wrist pain is defined as a non-resolving pain in one or both wrists lasting for more than 3 months. 1 Generally, the treatment of chronic wrist pain can be achieved non-surgically or surgically, and a step-by-step approach is normally followed. 1 When conservative management fails, a referral to a hand specialist with the possibility of surgical treatment becomes warranted. Pain in the wrist is transmitted through nerves that innervate the radiocarpal and ulnocarpal joints, mainly by Aδ and C fibers. Therefore, lysis of these nerve branches is known to theoretically and practically reduce pain while preserving motor or sensory functions. 2 Selective wrist denervation (SWD) is a surgical technique recommended for any painful and refractory wrist condition as a last resort before undergoing aggressive procedures, such as arthrodesis, arthroplasty, or radical wrist denervation. 3 SWD can be performed by doing a posterior interosseous nerve (PIN) neurectomy or/and an anterior interosseous nerve (AIN) neurectomy.4,5 One common complication of SWD is neuroma formation, which is an “inevitable and biologic response of the proximal stump after it has been divided in situations where regenerating axons are impeded from re-entering the distal stump.” 6 Several techniques have been suggested in the literature to prevent neuroma formation, including implantation of the nerve in a surrounding muscle or vein, neurorrhaphy, nerve stripping or silicone rubber capping. 7 Despite the existence of several approaches, no technique is recognized as the gold standard in the management of terminal neuromas.7,8 Nonetheless, centro-central anastomosis, also known as end-to-end neurorrhaphy, has been quite effective in reducing pain, with good functional results and an improvement rate varying between 94% and 100%. 9 By connecting the proximal ends of both severed nerves to each other, we can guide proximal axon growth and prevent the unorganized fascicular overgrowth at its end, which is a neuroma. 10 We therefore performed PIN and AIN neurectomy with neurorrhaphy of both nerves to treat a case of chronic wrist pain while concomitantly preventing neuroma formation in both sectioned nerves. This case report, to our knowledge, is the first to describe this surgical approach in the context of chronic wrist pain and prevention of peripheral injury-induced neuromas.
We first did a literature review using PubMed, Embase, and Cochrane databases to make sure this particular surgical technique has not already been described in the surgical management of chronic wrist pain. Several keywords were used with the Boolean operators “AND” and “OR”: chronic wrist pain, management, surgical technique, wrist denervation complications, and pain recurrence. Studies that showed relevance were retained; we did not find any similar cases reported in the literature.
Case
A 21-year-old right-handed woman was referred to our hand clinic for refractory chronic pain in her right wrist present for approximately 7 years. Being a part-time yoga teacher, the pain developed progressively in her right wrist and was experienced in most of her yoga routines. The patient was otherwise healthy; her medical and surgical histories were unremarkable. She had previously visited her family physician on several occasions for this condition and no cause for her pain had been identified. All possible conservative treatments were tried, from splinting and wrist rest to oral non-steroidal anti-inflammatory drugs and months of physical therapy, without avail. Pain in her wrist was persistent, becoming unbearable and preventing her from adequately pursuing her everyday activities and her profession. Since all non-operative treatments were exhausted and the patient requested a definitive treatment, she was referred to our orthopedic service. On her first visit, her chief complaint was impairing pain in her right wrist, mostly present upon exertion and occasionally at rest. No other symptoms, such as paresthesia or stiffness, were present. On physical exam, pain was localized over the scapholunate fossa, at the dorsum of hand, and aggravated on wrist extension. There were not any signs of inflammation, carpal instability, nascent dorsal wrist ganglion or vascular and trophic alterations. An X-ray of the wrist was done to eliminate any possible carpal bone fractures or a scapholunate etiology that would explain her persistent pain. X-rays of her right wrist were negative. A magnetic resonance imaging was also performed to evaluate any ligamentous injuries or occult ganglia, but similarly to the X-rays, none of the findings could justify the pain. Given the negative results of the imaging modalities, a diagnostic arthroscopy was recommended to explore the wrist and try to identify a possible source to her pain. Arthroscopy and debridement of the dorsal capsule of the right wrist were performed. On follow-up, her pain had slightly improved, but her range of motion (ROM) was expectedly limited. She was referred to physical therapy (PT) for ROM exercises and a follow-up appointment was given. Two months after the intervention and extensive PT, she was seen in clinic for the second time. Pain had improved but remained present, and she had not yet regained full motion of her wrist. One month later, she requested to be seen since her pain had worsened. During that visit, a 40 mg/ml depomedrol injection was administered in the right wrist joint to temporarily relieve the pain. Three months after the corticosteroid infiltration and almost 5 months post-arthroscopy, she experienced complete relapse of her symptoms despite non-steroidal anti-inflammatory drugs and regular PT. Given the chronicity of the pain in absence of an anatomic lesion and the exhaustion of non-surgical treatments, a definitive treatment option had to be offered. SWD consisting of PIN and AIN neurectomies and neurorrhaphy was suggested since it would potentially ensure a better success rate and could possibly reduce the risk of neuroma formation post-operatively. A diagnostic anesthetic block was performed in clinic around the distal PIN and AIN, 3 cm proximal to the radiocarpal joint, and was positive. The simultaneous block of both nerves is performed by simply advancing the needle through the interosseus membrane once the PIN block is complete, which grants access to the AIN. This anesthetic block had successfully eliminated the pain, which could not be triggered on physical exam or by the previously painful yoga postures. All the steps of the surgical procedure were explained to the patient and all frequent and rare complications were disclosed. After answering all her questions, the patient consented to undergo the procedure. Per-op, PIN and AIN neurectomy via dorsal approach (Figures 1 and 2) followed by PIN and AIN neurorrhaphy in an end-to-end fashion (Figure 3) were performed under loupe magnification (Zeiss 3.2X500). The surgery went as planned, with no per-operative complications. She was discharged home the same day with a short arm cast.
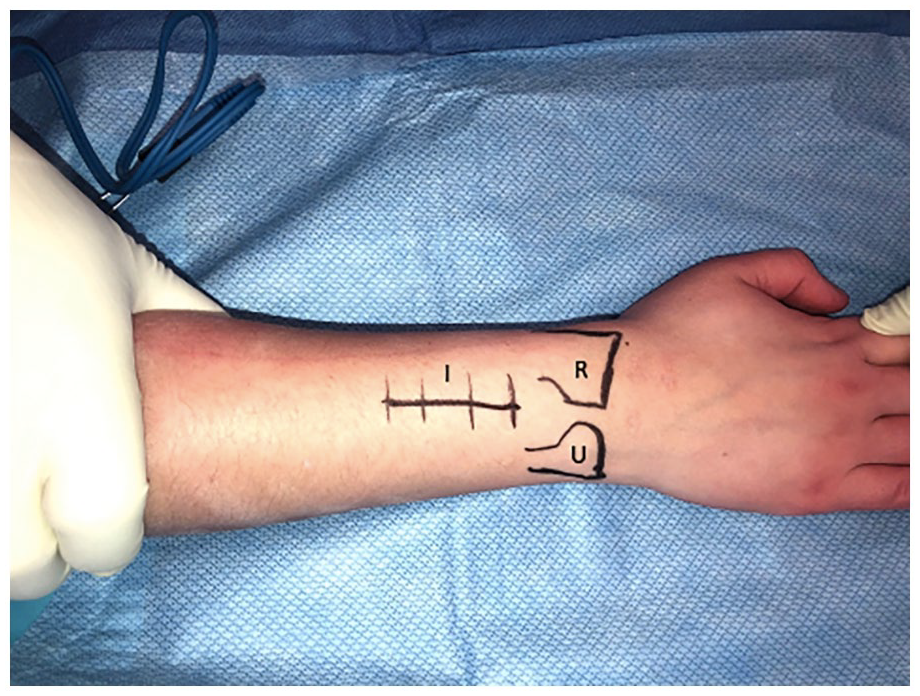
Pre-operative surgical incisions markings on the dorsal aspect of the right wrist. The radius and ulna are identified and marked to facilitate the dorsal approach to posterior interosseous nerve exposure.

A single 3 cm incision on the dorsum of the wrist with subcutaneous dissection. Posterior interosseous nerve and anterior interosseous nerve are exposed and identified.

Posterior and anterior interosseous nerves neurorrhaphy following neurectomies. Above the white background, the PIN and AIN are anastomosed together in an end-to-end fashion to aid in neuroma prevention.
The patient was seen consecutively at 2 weeks, time at which the cast was removed, scar management and physical therapy started, and at 2 months after the PIN and AIN neurectomy with neurorrhaphy. Patient stated the internal wrist pain had resolved immediately after the surgery and that the pain from the surgical procedure, such as the incision and stiffness from immobilization, had completely disappeared at the 2-month follow-up appointment. Wrist ROM was complete, and the surgical incision healed properly. We recommended she continue with regular ROM exercises at home and was discharged with follow-up as needed. She was reassessed 2 years after the intervention and no recurrence of any type of pain was objectified. She maintained full ROM without any limitations.
Discussion
This case report shares a novel approach of a neurorrhaphy as an adjunct to AIN and PIN neurectomy for the relief of chronic wrist pain. By anastomosing the proximal severed ends of both nerves, we would prevent the sectioned nerve ends from healing in an uncontrolled manner resulting in a lump of unorganized axon fibers and non-neural tissue growth, ultimately in neuroma formation.6,7 The latter is known to be a common complication of selective wrist neurectomy and a cause of persistent or increasing pain in the wrist post-interventions. 7 In fact, Loh et al. described clinical cases of four women and two men who developed chronic wrist pain after ganglionectomy through PIN or AIN neurectomy because of neuroma formation. 11 Furthermore, in a literature review conducted by Chin et al. to evaluate the treatment outcomes of SWD, the rates of the procedure’s complications, including pain recurrence, varied between 6% and 29% and neuromas developed in 8% of patients. 4 Several techniques have been suggested in the literature for the management of peripheral neuroma formation. However, even with all the current advancements in microsurgery, the proposed approaches remain experimental and are not evidence-based.7,8 Despite requiring high technical skill and being at times anatomically unachievable, end-to-end coaptation has still proven favorable outcomes in terms of pain reduction in the context of peripheral neuromas management of amputee. 9 Considering the significant possibility of neuroma formation with isolated neurectomies and its involvement in persistent wrist pain, we realized a PIN and AIN neurectomy followed by a neurorrhaphy of both nerves together in an end-to-end fashion. Our patient’s pain had partially subsided at her 2-week follow-up and had completely resolved after 2 months. No complications were experienced after the procedure, and with PT, she was able to maintain complete ROM in her right wrist. Patient was extremely satisfied with the procedure and had no relapse at her 2-year follow-up, despite pain recurrence being a very common complication of PIN and AIN neurectomy. 10 Therefore, we believe this technique confers an advantage in chronic pain management and could possibly prevent peripheral neuroma formation.
Conclusion
Posterior interosseous nerve and anterior interosseous nerve neurectomy followed by an end-to-end neurorrhaphy resulted as an effective surgical technique in the management of chronic wrist pain. While it has never been described and attempted before in the context of SWD, it is innovative and could possibly be successful at preventing neuroma formation and pain recurrence that is frequently associated with wrist neurectomies. Its effectiveness cannot be established following a single case and further surgical trials and clinical cases are required to cement its effectiveness and positive outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The preparation of this case report was funded by the Fond pour la Recherche et l’Enseignement en Orthopédie de Sherbrooke (FREOS).
Ethical approval
Ethical approval to report this case was obtained from the Comité d’éthique de la recherche du CIUSSS de l’Estrie-CHUS (Ethics approval number: 2021-4081). All procedures followed were in accordance with the ethical standards of the Comité d’éthique de la recherche du CIUSSS de l’Estrie-CHUS on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Statement of human and animal rights
This article is a case report of existing data and does not contain any additional studies with human or animal subjects.