
Abstract
Background and Aims:
Whether or not radiological results correlate with functional outcome after operative treatment of distal radius fractures still remains controversial. We carried out a retrospective study to analyse the long-term (6.5 year) outcome of radius fractures treated by means of surgery in our hospital. The aim of the study was to explore whether step-off on radius joint surface, shortening of the radius versus ulnar height and dorsal or volar tilt of the radius correlate with long-term Patient-Rated Wrist Evaluation or Quick Disability of the Arm, Shoulder and Hand scores among 100 consecutive patients after surgical treatment.
Materials and Methods:
Of these, 60 patients (63 wrists) participated. They were examined radiologically, clinically and by means of a questionnaire.
Results:
Shortening of the radius correlated significantly with both Patient-Rated Wrist Evaluation and Quick Disability of the Arm, Shoulder and Hand scores. Step-off on the radius joint surface correlated significantly with worse PRWE scores, with no difference in Quick Disability of the Arm, Shoulder and Hand evaluation. Dorsal or volar tilt showed no statistical correlation (though it was mild in this group). The age of the patients (below 60 years vs 60 years or above) did not affect the PRWE or Quick Disability of the Arm, Shoulder and Hand results.
Conclusion:
Our results indicate that when it comes to conserving the radial height and congruence of the joint surface, the more precise the reduction of the fracture achieved by surgical means, the better the functional outcome.
Keywords
Introduction
A distal radius fracture is the most common upper extremity fracture. The annual incidence in Finland is 258 per 100,000 inhabitants per year. 1 Among females, the incidence is higher and it grows progressively from perimenopausal age. 2 With ageing of the population, the incidence of distal radius fractures is increasing constantly.
Failure to regain normal anatomy has been shown to cause long-standing or even permanent pain and loss of wrist function. 3 Radial shortening of >2 mm and an articular step of >2 mm has been reported to be associated with worse patient-reported scores. 4 Interest in operative reduction of dislocated fractures has increased during the last decade, 5 especially in connection with the development of various surgical devices. Many reports show that better anatomical reduction leads to better functional outcome.6,7 In particular, use of locking volar plates in treating unstable distal-end radius fractures has been shown to be associated with excellent to good functional outcomes. 6 However, and especially among elderly people, it has been suggested that radiological or anatomical outcomes do not correlate with clinical outcome or patient satisfaction.8,9,10 In addition, patients are predisposed to complications of surgery, which are not rare.11,12,13 The influence of regaining normal anatomy is not clear when it comes to clinical outcome.8,14
According to Current Care National Guidelines of treatment, 15 acceptable reduction in conservative cast treatment of fracture of the radius are no dorsal/volar tilt over 15°/20°, radius shortening less than 3 mm and maximum step-off on joint surface 1 mm. These guidelines emphasize customizing of these recommendations in persons more than 65 years of age, in whom clear evidence of functional benefit of anatomical reduction has not been shown.9,10
Surgery considerably increases direct costs of treatment compared with closed reduction.16,17 If, however, surgery helps a patient to avoid disability in work or daily living, it can be assessed as being beneficial.
The aims of our study were to assess long-term radiological and functional outcomes in cases of distal radius fractures surgically treated at Helsinki University Hospital and to see whether or not the radiological outcome is associated with the clinical outcome. In treating distal radius fractures operatively, we sought to discover whether or not aiming for perfect anatomical reduction is really associated with good functional outcome. We looked at patient-reported outcomes, that is, Patient-Rated Wrist Evaluation (PRWE) 18 and Quick Disability of the Arm, Shoulder and Hand (QuickDASH) scores and clinical and radiological data. We also aimed to find out whether the results are different in different age groups (below 60 years vs 60 years and above).
Patients, materials and methods
We performed a retrospective, long-term follow-up case series study of 100 consecutive patients (103 wrists) with distal radius fractures surgically treated at Helsinki University Hospital, Clinic of Hand Surgery.
The inclusion criteria were all adult patients with traumatic distal radius fractures operated upon from 1 January 2009 to 22 April 2009 regardless of the type of operation. The exclusion criteria were home address outside the hospital district and/or postoperative procedures performed elsewhere in another hospital.
All 100 patients were invited to take part in a follow-up study in September–October 2015 (6.5 years after the operation). Of these patients, 9 had died, 5 lived abroad, 2 were in too poor a physical condition to participate, 12 were unreachable (no address available) and 12 did not arrive for their appointment. They were excluded; 60 patients (63 wrists) came for follow-up. They were the patients treated surgically during the time period of 1 January 2009 to 22 April 2009, and this consecutive case series was considered to represent about one-third of the annually operated distal radius fractures in our hospital. The research protocol was approved by Helsinki University Hospital Ethics Committee and written informed consent was obtained from all participants of this study.
The follow-up visit was organized 6.5 years after operation for each patient in the autumn of 2015. Radiography of the wrist (standardized posteroanterior and lateral aspects) was carried out. The patients completed PRWE and QuickDASH questionnaires and a clinical examination was performed. We interviewed the patients in connection with their symptoms and measured wrist ranges of motion (active extension, flexion, supination and pronation) with a manual goniometer and compared the results with those from the contralateral unaffected side. Grip strength was evaluated using a dynamometer (JAMAR hand dynamometer Model J00105, Lafayette, IN 47903, USA) and compared with that on the contralateral side, taking into account a 10% difference between the dominant and non-dominant hand. In grip-strength analysis, the bilateral cases were excluded. We recorded any complications, later operations and ability to work. The following parameters from radiographs were measured (Figure1): step-off/incongruity of the joint surface, radius shortening compared with the ulna and dorsal (or volar) abnormal tilt of the radius. Radiological results were taken to be ‘good’ if there were none of these. Clinical outcomes in cases of step-off, shortening and dorsal/volar tilt were analysed separately. A-type extra-articular fractures were excluded in analysis of the influence of step-off on the clinical results. Concerning shortening of the radius, the cases were divided into two subgroups: those with shortening of 2 mm or more (12 cases) and those with less than 2 mm of shortening or no shortening at all (51 cases).

(a) Radius height (shortening) compared with ulna (mm = A). (b) Dorsal inclination of radius (dorsal tilt, degrees = B). (c) Step-off on joint surface (mm = C).
Finally, we divided the 60 patients into two subgroups: persons under 60 years of age at the time of fracture 32 years and those aged 60 years or more than 28 years. We checked to see whether there was more bone deformity in the older group and evaluated the clinical outcome via PRWE and QuickDASH questionnaires separately for these groups. We also recorded complications.
Statistical methods
The Mann–Whitney U test was used for analysis of continuous variables in two independent groups. For parameters with skewed distribution, medians and ranges are reported. For normally distributed parameters, mean and standard deviation (SD) are reported. Significance was set at 0.05. We performed all statistical analyses with NCSS Hintze software, J 2012 (NCSS 8; NCSS, LLC, Kaysville, UT, USA; www.ncss.com).
Results
The mean age of the patients at the time of fracture was 55 years (range: 23–78 years, SD: 13.7 years) and at the follow-up visit, 61 years (29–84 years, SD: 14.6 years). There were more female patients (77%), and they had a higher mean age compared with the men (65 vs 49 years; Table 1). In 51% (32 wrists), the fracture was in the dominant hand, and according to AO Classification, 19 a type C fracture was present in 39 wrists (62%), a type B fracture in 4 wrists and a type A fracture in 20 wrists. In most cases, the operation type was reduction and fixation with a volar locking plate. In one case, a non-locking plate was used, and in three cases, K-wires only. K-wires for additional support were used in 12 cases. The operations were carried out by hand surgeons, orthopaedic surgeons and hand surgeon/orthopaedic surgeon trainees (after adequate education), which is the conventional practice in our hospital. In 34 of 63 wrists, good anatomical reduction was achieved radiologically (54%) according to generally accepted guidelines. 20 In 29 cases, there was some failure according to one or more of the radiological images: 11 showed step-off on the joint surface; in 15 wrists, the radius was shortened compared with ulnar height (data given as follows); in 11 cases, there was dorsal tilt of the radius, and there was abnormal volar tilt in 2 (Table 2). Examples of X-ray images of suboptimal radiological results are presented in Figure 2. In the cases of good reduction, there was no dorsal tilt, no radius shortening compared with the ulna and no step-off on the joint surface. The median QuickDASH score in these cases was 4.5 (0–40.9) and the PRWE score was 4.25 (0–51.5). A step-off on the joint surface was measured in 11 cases (17%; median = 1.8 mm and range = 1–3 mm). The influence of step-off was analysed after exclusion of A-type extra-articular fractures (Table 3). It was significantly associated with worse PRWE results (median = 17.5 vs 4.5, p = 0.043), but not with QuickDASH scores (median 11.4 vs 4.5, p = 0.364). The radius was shortened compared with the ulna in 15 cases (24%; median = 3 mm and range = 1–11 mm) in 12 wrists by 2 mm or more. We carried out the analysis by subdividing the cases into those with radial shortening of 2 mm or more and those with less than 2 mm of shortening (or no shortening). Shortening significantly correlated with the clinical results: PRWE, median 17.5 versus 4.5 (p = 0.035) and QuickDASH, median 11.4 versus 4.54 (p = 0.020; Table 3). Increased dorsal or volar tilt (when compared with normal volar tilt) was seen in 13 cases: dorsal tilt in 11, median 5°, volar tilt in two cases (10° and 15°). In Mann–Whitney U tests, there was no significant association between dorsal tilt and PRWE scores (median = 6.75 vs 5.0, p = 0.70) or QuickDASH results (median = 6.8 vs 4.5, p = 0.31; Table 2).
Demographics of the patients with surgically treated distal radius fractures.
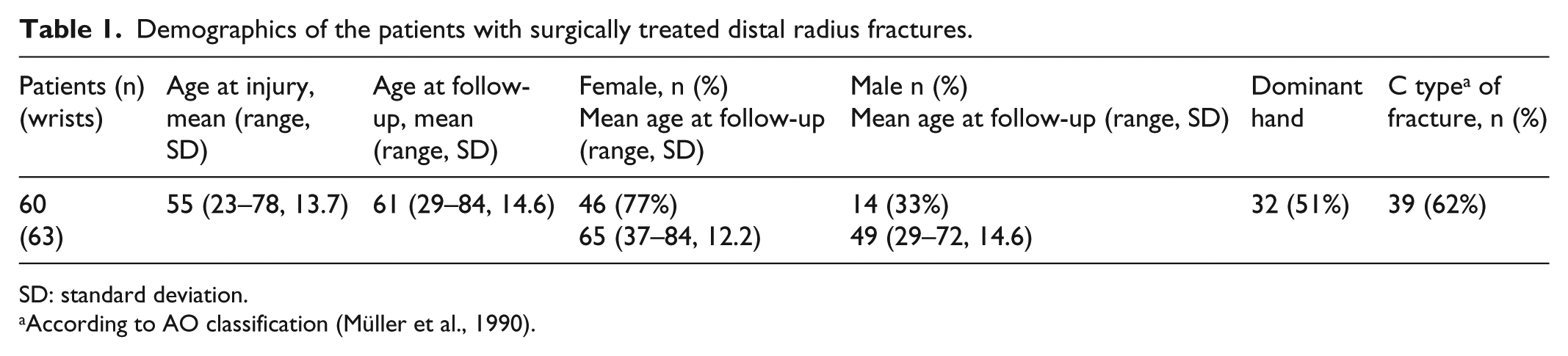
SD: standard deviation.
According to AO classification (Müller et al., 1990).
Radiological results in 63 cases of surgically treated distal radius fractures.

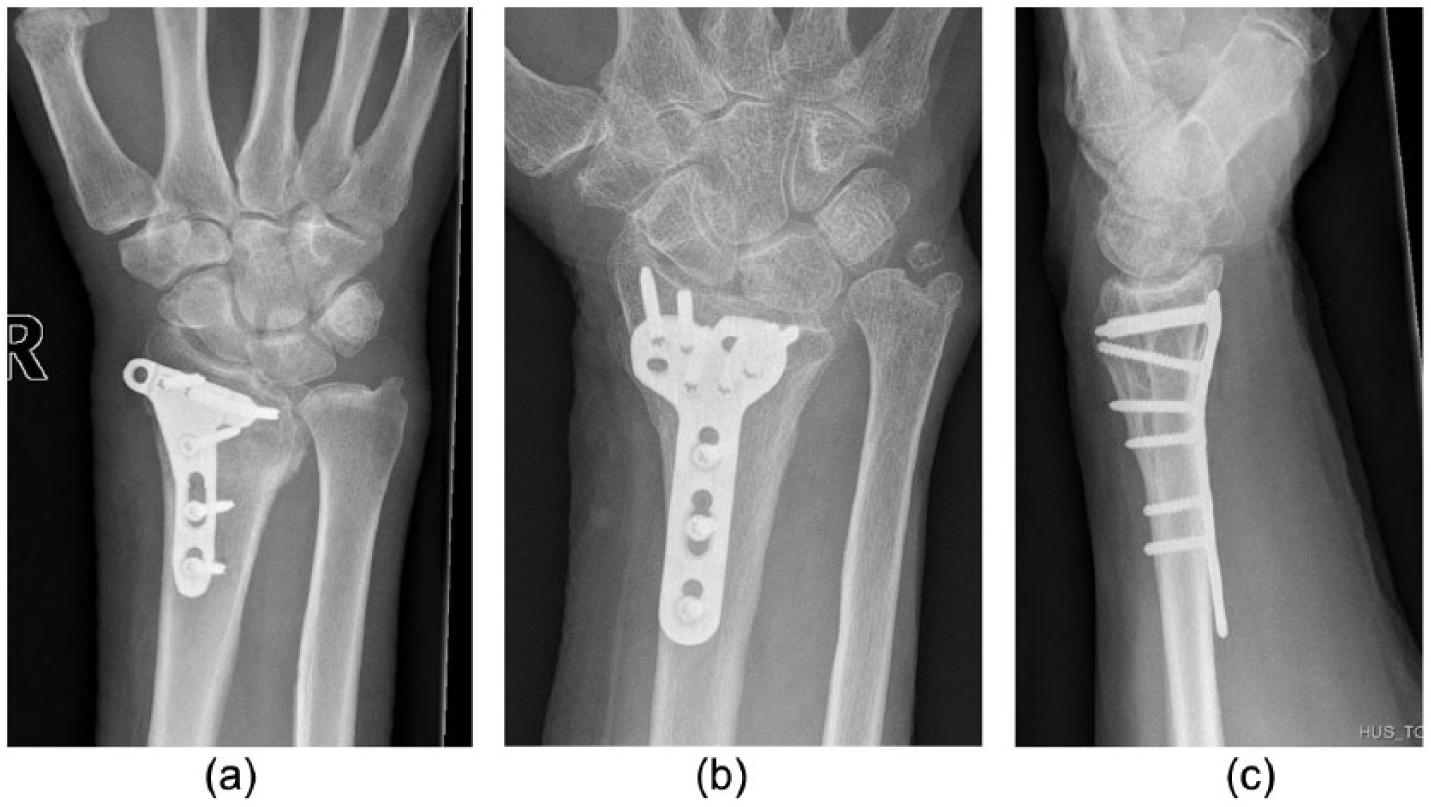
(a) Remaining step-off of 2 mm on radius surface. (b) Radius shortening compared with ulna 9 mm. (c) Dorsal tilt of radius 10°.
Association between radiological and functional outcome 6.5 years after surgical treatment (Mann–Whitney U test).

PRWE: Patient-Rated Wrist Evaluation; QDASH: Quick Disability of the Arm, Shoulder and Hand.
Shortening of radius compared with ulna.
PRWE, median value.
QDASH, median value.
In the majority of cases, there was some stiffness in extension (43 wrists; mean 13°) and flexion (35 wrists; mean 10°) compared with healthy wrists, but the deficits were mild. These deficits were not significantly associated with PRWE and QuickDASH scores. Mean grip strength compared with the opposite side (bilateral fractures excluded) was 89% (range = 45%–127%; SD = 16%). In six patients, grip strength was better on the surgically treated side. Five of them had had a fracture in the non-dominant hand. Extension lack was associated with poorer grip strength (p = 0.03). None of the measured radiological parameters (step-off, radius shortening or tilt) was significantly associated with grip strength.
Operative complications occurred in 10 cases (16%), and they needed reoperation (Table 4). Primary reduction failure happened in three wrists, screw penetrated into radiocarpal joint in two cases, tendon rupture in three (two extensor pollicis longus and one flexor pollicis longus), one median nerve entrapment and one postoperative haemorrhage. The clinical outcome was significantly worse in these cases (median PRWE score = 17.5 vs 5.0, p = 0.029; median QuickDASH score = 13.6 vs 4.5, p = 0.038). In addition, 16 reoperations were carried out: in six cases, plate removal and in 10 cases, K-wire removal. (Most of the K-wire removals were planned in advance.) Of the 60 patients, 33 (55%) were retired at the time of follow-up. None of those working suffered work disability as a result of the fracture; 26 patients had returned to earlier work. One person (with bilateral fracture) had undertaken re-education for another job.
Complications after distal radius fracture operations.
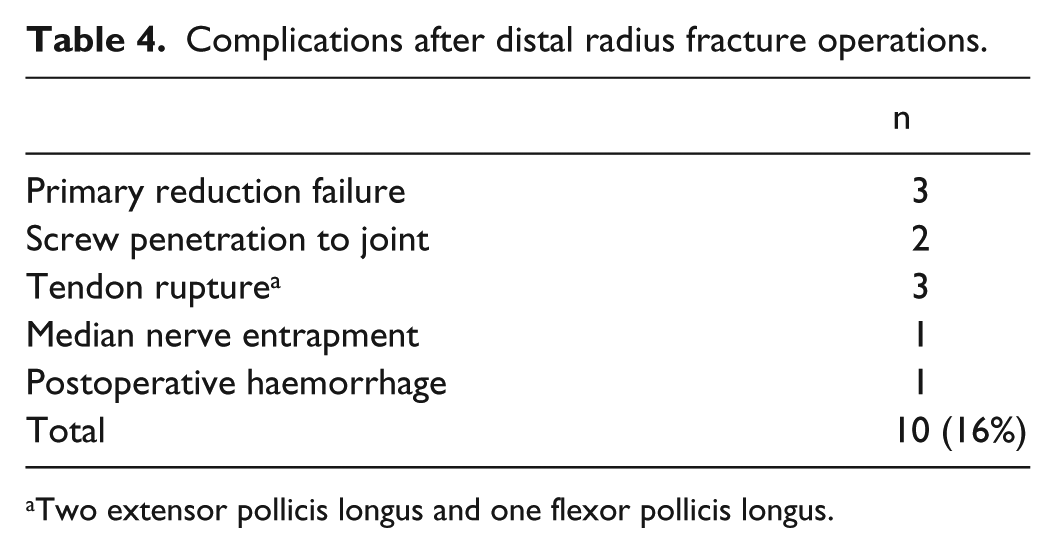
Two extensor pollicis longus and one flexor pollicis longus.
In the subgroups of those under 60 years of age and persons of 60 years or more, the clinical outcomes as evaluated by PRWE (median score 4.5 vs 8.25, p = 0.36) or QuickDASH (median score 4.5 vs 6.8, p = 0.06) were not significantly different. There were no significant differences in the radiological parameters, although the subgroups were too small to estimate significance reliably (Table 5).
Results concerning patients under 60 years of age and patients of 60 years or more.

Seven of the complications had occurred in the older group, versus three in the younger group. However, there was no statistically significant difference (p = 0.07) in this small subgroup. None of the complications appeared to be age-related. Unsatisfactory reduction causing screw penetration to the joint (two cases) and two unsatisfactory primary reductions were in older patients, as was the one case of collapsed fracture.
Discussion
In fracture treatment, good radiological results have been shown to correlate with good clinical results in several studies.20,21 Likewise, incorrect fracture reduction often results in problems.3,20,22
Incongruity at the joint surface and radius shortening have been found to be associated with compromised function.4,6,22-25 The present results strengthen these findings when it comes to shortening of the radius and also partly to step-off on the radius joint. In our study, measurable step-off at the joint surface was associated with worse outcome according to PRWE, but not with QuickDASH scores. This might be explained by PRWE perhaps being more specific for distal hand function, while QuickDASH includes more non-specific questions (e.g. social intercourse etc.). For assessing the significance of radius shortening, our subgroups were small, but all in all, any shortening resulted in worse clinical results according to PRWE and QuickDASH data. This also strengthens the findings of Dario et al., 14 who reported that ulnar variance was one of the most important radiographic parameters to be restored to obtain good functional outcome. As regards grip strength, we found no association with anatomical deformities. Six of the patients had the relative grip strength better in the hand treated with surgery. No specific explanation emerged; five of them had the fracture in their non-dominant hand.
Ng and McQueen 20 have pointed out that the impact of residual dorsal/palmar tilt is not clear in the literature and there has even been bias due to the error rate in measuring this value. In our material, dorsal or volar tilt of the radius was moderate (median dorsal tilt 5°), and it did not cause significant clinical inconvenience. Lindfors et al. 15 point out acceptable dorsal/volar tilt to be less than 15°/20°. Our median dorsal tilt was only 5° (range = 3°–22°), and the volar tilt was in the limits of the National Guidelines. This presumably is the reason for no significant affect on clinical outcome.
Complications after surgical treatment of distal radius fractures are not uncommon. Arora et al. 12 2013 reported an overall complication rate of 27% (31 of 114 wrists), though the most frequent problems were cases of mild flexor and extensor tendon irritation. In our material, the complication rate was 16% (in 10 wrists of 63), and the patients with complications underwent new operations: new reduction and osteosynthesis, hardware removal, tendon reconstruction, neurolysis and haemostasis. Partly, the complications were operation-technique-related and partly for other reasons. We also often carried out removal of fixation material (in 16 cases, 24%). Of them, 10 were K-wire removals planned in advance. Six plates were removed; mostly because of some discomfort.
In elderly people (more than 65 years of age), no association between functional and radiological outcomes has been found.8,9,10 However, in a recent study, Martinez-Mendez 23 found that with surgical plating, there was better outcome in patients of 60 years of age or more with complex intra-articular AO-type C fractures. In the elderly population in particular, it has been recommended to consider if the patient will benefit from surgical treatment.8,9,12,15 In our subgroups of those under 60 years of age and 60 years or above, we found no difference in the clinical outcome as assessed by PRWE or QuickDASH scores. However, the age limit was relatively low and near the mean age (55 years, SD = 13.7 years) of all the patients. Of the 10 complications, 7 occurred in the older group, but this cannot be considered to be a direct consequence of age.
We acknowledge weaknesses of our study. It is a retrospective case series follow-up study. The sample size was not calculated and determined by means of power analysis beforehand, as we considered that 100 consecutive patients (about one-third of those surgically treated in our institution yearly) would show the average results of our treatment. The fractures were not divided into subgroups according to AO classification except for the analysis of incongruence of the joint surface (Table 3). With such a small number of cases, the subgroups would become too small for comparison. In addition, we acknowledge that the initial injury type was not taken into account; a severely destroyed joint surface is difficult to reduce, and the reason for step-off and worse outcome could also be a sign of a high-energy trauma. The strength of the study is the fact that 60 patients (66% of the 91 invited patients who were alive) came to the follow-up visit and were clinically and radiologically evaluated 6.5 years after operation.
Conclusion
Our results indicate that the more precise the reduction of the fracture achieved by surgical means when it comes to avoiding radial shortening and articular step-off, the better is patient-rated functional outcome. Dorsal (or volar) tilt, in contrast, does not seem to affect the clinical results as long as it is moderate. We still have to keep in mind the relatively high number of complications related to surgery, as well as the need for reoperations because of hardware removal.
Footnotes
Acknowledgements
We thank MSc Timo Pessi for the statistical analysis and research nurse Leena Caravitis for the help in the practical arrangements of this research project as well as for collecting the data. And Thanks to Nick Bolton, PhD, for checking the English language of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted in accordance with the Ethical Committee of Helsinki Hospital District, Helsinki, Finland and research protocol was approved by Helsinki University Hospital Ethical Committee (no. HUS/330/13/02/2012).
Informed consent
Written informed consent was obtained from all participants of this study.
Trial registration
*NAME OF TRIAL REGISTRY: TRIAL REGISTRATION NUMBER*HUS/221/2017 and 16.1/2013 HYKS Oper ty EVO. Retrospective case series of 100 surgically treated wrists.