
Abstract
Residual foreign bodies are usually observed inside the body after foreign body penetration injuries. However, foreign bodies inside or near the joints are rarely encountered. In the case study included in this report, the case of a foreign body in the posterior ankle region of a 10-year-old child is presented, along with a new study highlighting the technique of its excision with hindfoot endoscopy. The visualization and capture of a foreign body within this region, and its relation to endoscopic excision, has been reported as being a support for hindfoot endoscopy. The aim of this article is to highlight the need for the provision of a low threshold arthroscopic hindfoot surgery in children who display the appropriate symptoms. The purpose of this surgery is to efficiently remove intra-articular hindfoot loose bodies and to gain functionally improved results, when compared with open techniques.
Introduction
Residual foreign bodies inside the body are usually seen after injuries that involve foreign body penetration. These injuries are mostly seen in the lower extremities, but can also be seen in the upper extremities, and especially in the plantar region of the foot. Foreign bodies inside or near the joints are rarely seen. 1 Excision of the foreign body, and the debridement of the surrounding granulation tissue, is the usual treatment for these injuries. Excision is mostly performed with open techniques, but, in the case of intra-articular foreign bodies, it may be performed arthroscopically.
Hindfoot endoscopy is now considered a reliable treatment technique for lesions in the posterior ankle region and is generally preferred to open techniques. The major indications of the need for hindfoot endoscopy are osteochondral lesions, bone and soft tissue impingements, tendinitis, ligament injuries, and tumoral lesions, and there is the possibility that further items may be added to these indicators.2,3
In this article, the case of foreign body in the posterior ankle region of a 10-year-old child, and new results that relate to the technique of its excision with hindfoot endoscopy, is presented. The visualizing and the capture of a foreign body within this region, and its related endoscopic excision, has been reported as being new set of data relating to hindfoot endoscopy.
Case study
A 10-year-old boy, who was suffering from an injury to his posterior ankle region due to it being penetrated by a sharp object (a needle) 3 years ago, was presented to our clinic. A physical examination revealed posteromedial ankle tenderness, which made walking very painful. Posterior ankle impingement tests were positive, no infectious findings were present during the evaluation, and complete blood count, sedimentation, C-reactive protein levels were all found to be normal. There was also no trace of rheumatologic, immune, or metabolic disorders that served to confuse the diagnosis.
Anteroposterior and lateral direct radiographies of the ankle were taken. Radiographic examination revealed the presence of a metallic sharp object (foreign body) in the hindfoot region, just posteriorly located as os trigonum (Figure 1(a)). It was therefore decided to perform an excison via hindfoot endoscopy. Preoperatively tetanus prophylaxis was controlled, and antibiotic prophylaxis (Cefazolin Sodium 0.5 g) was administered.

Preoperative (a) and postoperative (b) anteroposterior and lateral radiography.
A standard two-portal endoscopic approach technique was used in the prone position, as described by Van Dijk et al. 4 Posterolateral and posteromedial portals were used, with the posterolateral portal being used for the arthroscope, and the posteromedial portal being used for the instruments. Following the endoscopic examination, the presence of dense granulation tissue was detected in the middle of the soft tissue area of the hindfoot (Figure 2(a)). During the procedure, granulation tissue was first released from its surrounding tissues, total excision and endoscopic debridement were performed, flexor hallucis longus tendon was exposed and released, and finally, the os trigonum was checked for impingement, and no impingement was detected with ankle plantar flexion. The needle was subsequently found inside the granulation tissue (Figure 2(b)).
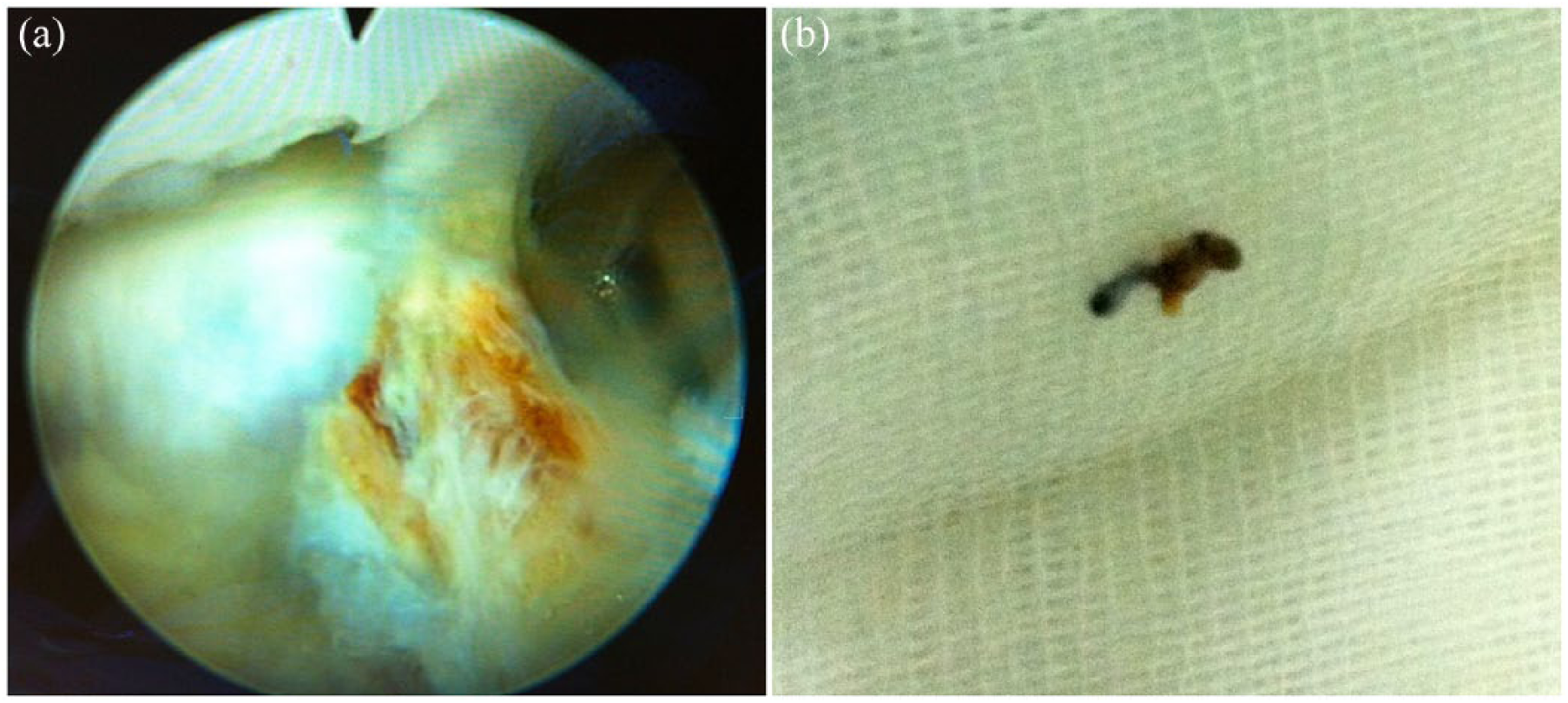
Endoscopic view of the granulation tissue (a) and the needle after excision (b).
Postoperative radiographies were taken and the hindfoot was confirmed to have been cleared of the foreign body (Figure 1(b)). Early weight-bearing and active range of motion were initiated after 24 h, post operatively. The child had an excellent post operative recovery and regained full function 1 year following the procedure.
Ethics: This case report is presented after informed written consent of the patient and parents.
Discussion
Intra-articular foreign bodies are quite rare when compared to extra-articular localized extremity foreign bodies. Intra-articular foreign bodies tend to be more symptomatic, because of the granulation tissue that generally surround them. Foreign bodies in areas around the foot are usually seen after the penetration of sharp objects like needles and are almost always found in the plantar part of the foot. Foreign bodies in the posterior ankle region are rarely seen.
The main indication of hindfoot endoscopy is posterior ankle pain. The different pathologies that lead to posterior ankle pain can also be treated with hindfoot endoscopy.2,3 Posterior ankle impingement syndrome; os trigonum syndrome; tendinitis of the flexor hallucis longus, posterior tibial tendon, or peroneal tendons; post-traumatic calcifications; bony avulsions; osteochondral defects; tibiotalar and subtalar arthrosis; synovitis; loose bodies, Achilles tendinopathy, Haglund’s deformity, intra-articular cysts, intraosseous cysts, and their combinations, can all be the cause of posterior ankle pain.2,4–6
The endoscopic treatment of hindfoot and posterior ankle pathologies is an effective and safe method, compared to open surgical treatment.2,5,6 The two-portal posterior endoscopic approach, with the patient in the prone position, offers excellent access to the posterior ankle compartment. 4 Excision of a foreign body in the posterior ankle region is difficult because of the high density of soft tissue. It also can become problematic, especially in children, because of open physis. In general, there are more problems with open excision than with endoscopic excision. Open excision itself may produce granulation tissue during the healing process, and it may be very difficult to find the foreign body during open surgery.
While complications like nerve and tendon injuries may be seen more clearly during open excision, endoscopic excision is an extremely suitable choice of treatment in these cases due to its practicality and safety. The scope of what can be done with arthroscopy and endoscopy of the foot and ankle is expanding. The development of sound knowledge of the indications, merits, and potential risks of new techniques mean that will become powerful tools in foot and ankle surgery. 7
Conclusion
In conclusion, endoscopic foreign body excision from the hindfoot is a new variation of hindfoot endoscopy. It is seen to be a safe and effective treatment of choice in specific cases, especially in children. In future, newer revisions may be made to hindfoot endoscopy to improve it still further.
The aim of this article was to highlight the need of having a low threshold for arthroscopic hindfoot surgery in symptomatic children. The purpose of this is to efficiently remove intra-articular hindfoot loose bodies and to gain functionally improved results when compared with the open techniques.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient and his parents verbally and written consented to the use of his clinical images for this report. Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.