
Abstract
Liver abscess following foreign body perforation of the gastrointestinal tract is uncommon. Preoperative diagnosis is challenging as the ingestion of foreign body most often goes unnoticed with non-specific presentation. We report a case of a 68-year-old male patient presenting with abdominal pain and anorexia. His investigations and cross-sectional imaging revealed a liver abscess. A colonoscopy performed to find an etiology revealed an incidental finding of a colonic perforation from an impacted denture, which was successfully removed endoscopically. Therefore, pyogenic liver abscesses remain a therapeutic challenge despite advances in imaging and therapy. The case reflects the importance of investigating for etiology of unexplained liver abscesses. The patient made an uneventful recovery following abscess drainage by image-guided pigtail stent insertion. The colonic perforation was managed conservatively.
Introduction
Liver abscesses are one of the commonest causes for intraabdominal visceral abscesses, and they account for 48% of visceral abscesses and 13% of intraabdominal abscesses. 1 The incidence is slightly higher among men than in women. 2 Risk factors identified are comorbidities, such as diabetes mellitus, liver transplant, and hepatobiliary or pancreatic disease. 2 However, host factors such as primary invasive liver abscess syndrome following Klebsiella pneumoniae infection and conditions such as chronic granulomatous disease with recurrent infections are also known to contribute. 1 Furthermore, pyogenic liver abscesses are also associated with colorectal cancer and other malignancies in gastrointestinal tract. 3 The pathogenesis of pyogenic liver abscesses are multifactorial. Portal vein pyemia following bowel leakage, peritonitis, diverticulitis, inflammatory bowel disease, and carcinoma of the gastrointestinal (GI) tract are considered as an important source of infection, as later seen in our patient. Another route is by direct spread from biliary sepsis associated with biliary tract diseases, such as strictures, gallstones, and malignant obstruction. Hematogenous seeding through systemic circulation following a streptococcal or staphylococcal infection is considered another potential source of infection and more importantly should prompt evaluation for infective endocarditis.
Gastrointestinal tract perforation by ingested foreign bodies is uncommon, and formation of hepatic abscess secondary to foreign body perforation of GI tract is even rarer. It can result from portal vein pyemia following a foreign body in the GI tract or by migration of an ingested foreign body and direct perforation of the liver parenchyma through the GI tract.4–7 Management includes drainage of the abscess and antibiotic therapy. Drainage by non-surgical techniques such as image-guided drainage, endoscopic ultrasound (EUS)-guided drainage, or drainage by endoscopic retrograde cholangiopancreatography (ERCP) are preferred over open surgical or laparoscopic drainage. However, image-guided drainage is the preferred modality commonly performed due to its less invasive nature. The approach, however, depends largely on factors, such as the size and the number of abscesses. 1 We present a rare case of hepatic abscess caused by a colonic perforation by an accidentally ingested denture.
Case presentation
A 68-year-old male patient with a background history of hypertension presented with abdominal pain in the right upper quadrant associated with anorexia for 1-month duration. However, he did not report any fever, chills, altered bowel habits, melena, or per rectal bleeding. He had no previous abdominal surgeries. The general examination was unremarkable, devoid of any fever or tachycardia but the abdominal examination revealed a palpable liver extending beyond the costal margin. His basic blood biochemistry revealed an elevated leucocyte count of 16.8 × 103/µL with a C-reactive protein level of 9.4 mg/L and an elevated erythrocyte sedimentation rate of 119 mm/h. His liver and renal profiles were normal. Ultrasound abdomen revealed a hypoechoic lesion in the liver measuring 8.9 × 6.4 cm involving liver segments V, VI, and VII without internal vascularity suggestive of a liver abscess. Further imaging with triphasic CT of the chest, abdomen, and pelvis revealed a large irregular shaped loculated peripheral enhancing, centrally hypo-attenuated fluid density lesion measuring 8.3 × 10.8 × 6.1 cm in size involving segment IVA and IVB of the liver suggestive of a liver abscess with mass effect on the common hepatic artery branches (Figure 1). The CT did not show any features of intrahepatic or extrahepatic biliary obstruction. The collection was drained under ultrasound guidance with a pigtail catheter. Aspirated purulent fluid investigations confirmed a liver abscess. The full report revealed 17,600 mm3 of pus cells and protein of 9000 mg/dL with a significant growth of Escherichia coli, suggestive of the diagnosis of a liver abscess with cytology report confirming the diagnosis. The mycobacterial investigations for tuberculosis, amoebiasis, and Burkholderia pseudomallei, three important causes for liver abscess in South Asian region were negative. Upon further investigations, an elevated HbA1c of 6.4% in the pre-diabetic range was found although FBS was normal. Echocardiography was normal without any features to suggest endocarditis. The investigation for a cause continued with upper GI endoscopy, which was normal. However, interestingly, the colonoscopy revealed a denture impacted at the sigmoid colon adjacent to multiple diverticula. There was no endoscopic feature of diverticulitis. The patient was unaware of having swallowed a denture. The denture was removed carefully using a snare and foreign body forceps. There was superficial ulceration at the site of impaction but no obvious perforation seen on careful examination. It was thought that a microperforation would have spontaneously healed during the delayed personation. The patient was treated with intravenous cefotaxime for 2 weeks according to the sensitivity reports. The patients had an uneventful recovery. He discharged following 2-week hospital stay. Serial follow-up ultrasound scans revealed a resolving abscess. As the denture had only plastic attachments, it was difficult to identify on the previous CT scans; however, there was evidence of colonic perforation from a foreign body depicted in the CECT images retrospectively (Figure 2).

CECT abdomen depicting pyogenic liver abscess.
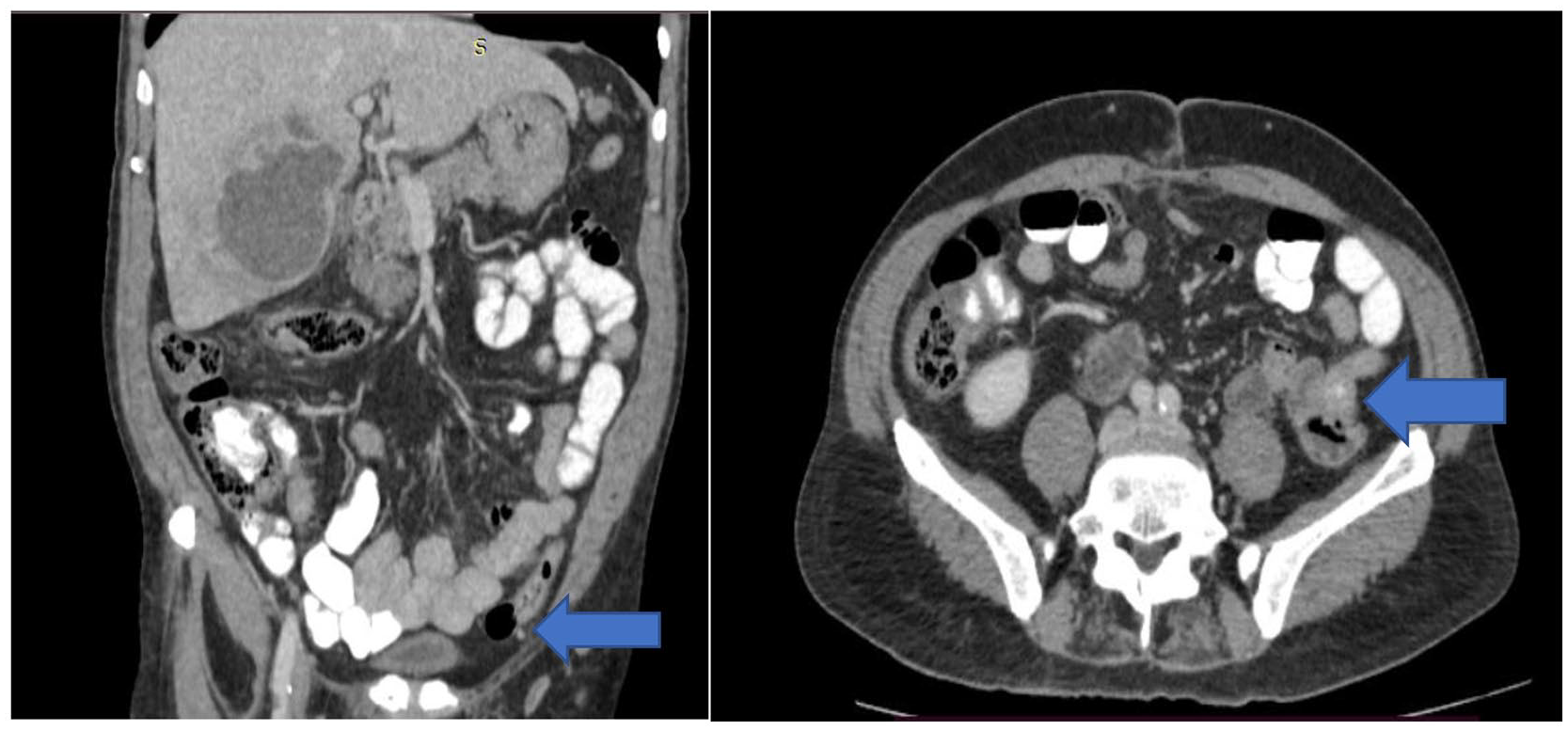
CECT abdomen—Denture impacted in colon depicted by the pointer.
Discussion
Pyogenic liver abscesses are the commonest type of visceral abscess. The etiology is diverse, which includes portal vein pyemia, direct spread from biliary sepsis, seeding from systemic circulation, and penetrating wounds inclusive of migration of ingested foreign bodies. 1 Our patient never had symptoms suggestive of colonic diverticulitis, and on abdominal examination, there was no tenderness over left lower quadrant. Most ingested foreign bodies (80%–90%) are known to spontaneously pass through within 1 week without any symptoms. 7 When symptomatic, it is usually due to underlying intestinal obstruction. Perforation is very rare accounting for less than 1% of the patients. Although the incidence is low, sharp ingested objects such as fish bones, needles, and toothpicks are known to result in perforation of hollow viscera commonly, the stomach, duodenum, ileocecal, and rectosigmoid regions of the GI tract.7,8 The diagnosis is challenging mostly owing to the non-specific symptoms on presentation. Most patients rarely recall the history of swallowing a foreign body on presentation and it will remain undetected until a potential complication like abscess formation occurs. Here, we discuss a case of a patient who had a pyogenic liver abscess following possible colonic perforation from a swallowed denture.
The classical presentation of a pyogenic hepatic abscess including fever, abdominal pain, and jaundice is rare. 1 Our patient presented with right upper quadrant pain with anorexia and weight loss, which are features of systemic response to an abscess formation. The routine biochemistry was also non-specific. Although cross-sectional imaging with ultrasound and contrast-enhanced CT are known to have a high resolution and accuracy, it commonly only identifies the hepatic abscess and fails to locate the etiology. 7 The quest for an etiology is fulfilled by other relevant investigations as seen in our patient. Our patient did not have most risk factors except for being pre-diabetic. There were no altered bowel habits to suspect inflammatory bowel disease or diverticulitis. Endoscopy is known to be of use when performed early in the course. Foreign bodies in the foregut before migration and in the hindgut and healed sites of perforation in the GI tract may be seen on endoscopy. 9 A study done by Chong et al revealed that out of the available diagnostic tools for foreign body perforation of the GI tract, CT is the modality used for diagnosis in most studies (53%), whereas only a minority of studies had endoscopy aiding the primary diagnosis out of which colonoscopy isolated in 3% of studies with esophagogastroduodenoscopy identifying the perforation in 4% of the studies. 6 In the present case, the impacted denture perforating the colon was detected only during colonoscopy (Figures 3–5).
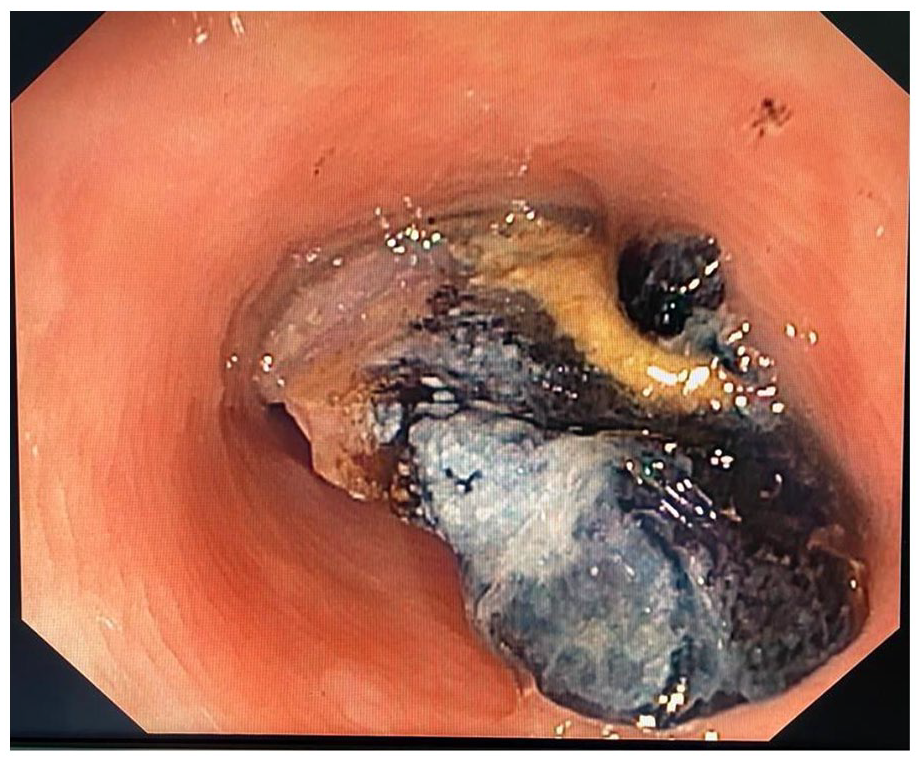
Endoscopic view of the perforating denture.

Endoscopic view of the denture in colon.

Removed denture.
Literature is limited mostly to case reports which include a variety of swallowed foreign bodies causing liver abscesses including bones, toothpicks, needles, pens, and rarely dentures. 5 A review by Santos et al. 5 on liver abscesses following foreign body perforation of GI tract revealed that fish bones are the commonest ingested foreign body and stomach is the commonest site of perforation. The use of dentures has been identified as one of the main risk factors for ingestion of foreign bodies because they result in impaired sensory feedback of the palate. Other related risk factors for foreign body ingestion were extremes of age, cognitive impairment or psychiatric conditions, and alcohol intoxication.10,11 Furthermore, they found that most resulted in hepatic abscesses in the left lobe. 5 The treatment of pyogenic liver abscess includes a conservative approach with aspiration and systemic antibiotic therapy which was successfully achieved in this patient.1,4,5 A study by Kanazawa et al. 7 revealed that image-guided percutaneous catheter insertion and drainage were more effective than intermittent needle aspiration. Since our patient’s liver abscess was easily detectable by ultrasound, the aspiration was successful with pigtail catheter insertion.
Conclusion
Pyogenic hepatic abscesses are the commonest intra-abdominal visceral abscess. The quest for etiology remains a diagnostic challenge. The presentation of swallowed foreign bodies causing perforation is often insidious and non-specific. Although cross-sectional imaging is known to be the first-line diagnostic tool with high rates of detection of foreign body perforation, it can still have limitations. This case reflects the importance of the use of endoscopy as a diagnostic and a therapeutic tool in management of these patients.
Footnotes
Acknowledgements
The authors wish to acknowledge ward staff who took care of this patient.
Availability of data and material
Data used in this analysis are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.