
Abstract
In this case report, we correct the analysis of mitigating intentional foreign body ingestion offered by Sarah J. Diamond and Amnon Sonnenberg. Patients who notoriously swallow foreign objects generate significant economic costs to hospitals. In previous publications, it has been argued that hospitals might reduce the need for endoscopy by offering such patients a paid position to discourage foreign body ingestions. However, the game-theoretical analysis offered in the literature was based on a static game which did not justify the relevant equilibrium. To obtain the actual goal of keeping the patient away from foreign body ingestion, we consider a repeated game with an infinite horizon. We show that there exists a combination of strategies applied by the hospital and the patient that leads to a steady state in which the patient will be discouraged from foreign body ingestion.
Introduction
Intentional foreign body ingestion is quite a common clinical issue. A small number of cases, at most 1%, may require surgical intervention. Patients who intentionally swallow foreign objects generate significant economic costs to hospitals.1,2 Thus, it is of utmost importance to focus on preventing such behavior. Diamond and Sonnenberg 3 offered a solution to the problem of hospitals and their patients who notoriously and intentionally swallow foreign objects. These authors used a game-theoretical approach to attempt to justify that the hospitals might reduce the need for endoscopy by providing some incentives to such patients. Since a minority of patients is responsible for repeated intervention, it has been suggested that hospitals could offer such patients a paid position, to discourage foreign body ingestions.
Case presentation
Diamond and Sonnenberg 3 considered the game of two players: a hospital and a patient given in Table 1.
One-shot game of the hospital and the patient as players in which the hospital chooses between endoscopy and providing incentives to the patient and the patient decides between ingesting and not ingesting foreign body.
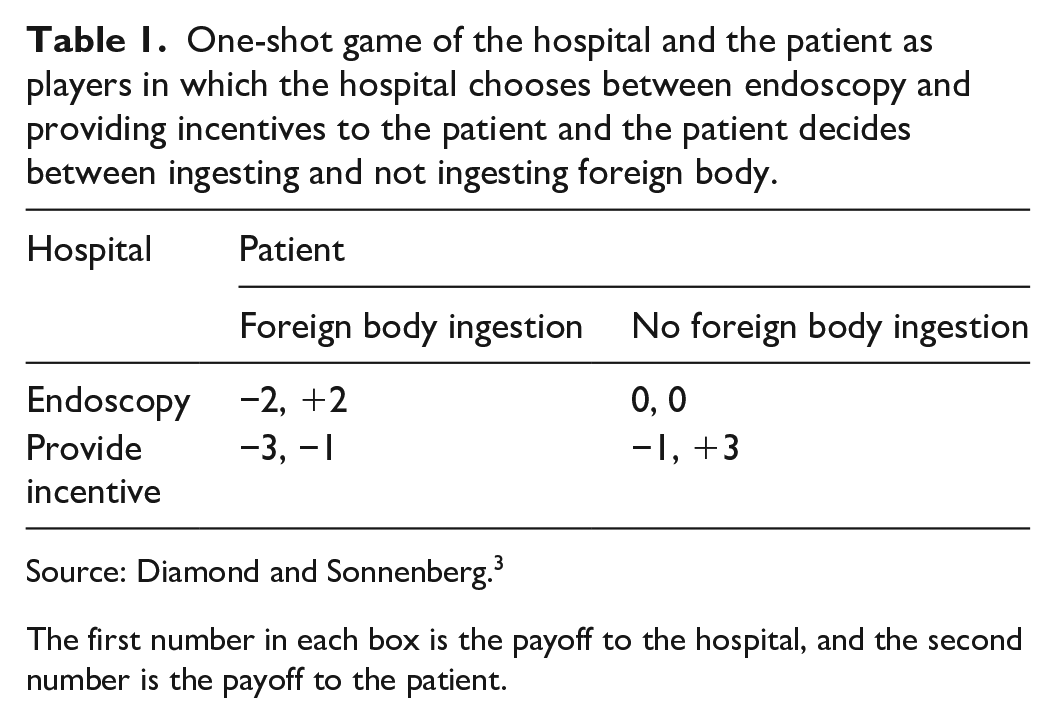
Source: Diamond and Sonnenberg. 3
The first number in each box is the payoff to the hospital, and the second number is the payoff to the patient.
They claimed that given the incentives provided by the hospital, the patient’s strategy would be no foreign body ingestion. Moreover, it has been argued by the authors that it is a steady state. However, from the game theory viewpoint, such a conclusion is not quite correct in the provided framework.
We should observe that the choice of no foreign body ingestion by the patient encourages the hospital to switch from “providing incentive” to the strategy of “endoscopy” because it allows it to increase its payoff from −1 to 0. In that case, however, the patient would obtain a payoff of 0 and would be better off by switching to the strategy of foreign body ingestion, which raises its payoff from 0 to +2.
Even though the outcome (−1, +3) generated by the strategy combination (“provide incentive,” “no foreign body ingestion”) is better for both, the hospital and the patient than the outcome (−2, +2) generated by the profile (“endoscopy,” “foreign body ingestion”), the only steady state is this last strategy combination. This would mean that the hospital will not reach its objectives. The hospital cannot be trusted by the patient that it will adhere to its strategy of providing incentives.
Discussion
The way to obtain the actual goal of keeping the patient away from foreign body ingestion is to consider a repeated game with an infinite horizon (we do not know how long the patient will be alive). In the case of a repeated (dynamic) game, we have to take into account a discount factor
Each player i (i = hospital or patient) has a payoff function

The dynamic game offered here has multiple equilibria. The famous Folk Theorem applies to this infinitely repeated game. 5 It states that any payoff vector that is better for all players than a Nash-equilibrium payoff vector of the constituent (static) game can be sustained as the outcome of a perfect equilibrium of the infinitely repeated game if the players are sufficiently patient (when both players of the game sufficiently value the future payoffs). However, we will focus our attention on the equilibrium outcome in which the patient is discouraged from ingesting foreign objects by the hospital creating appropriate incentives.
Let us consider a strategy in which at time t = 0 hospital decides to “provide incentive” and the patient chooses “no foreign body ingestion.” Both players continue to stick to their choices as long as none of them deviates from the chosen action. Should any of the players deviate from those choices, then the hospital will switch to “endoscopy,” and the patient will decide to choose “foreign body ingestion” in every future period (forever).
In game theory, we refer to this behavior as a grim trigger strategy, since an undesired behavior by any player triggers relentless “punishment” by both players. Here is a short proof that such a strategy will support the most desired behavior, that is (“provide incentive,” “no foreign body ingestion”).
Suppose that both the hospital and the patient adopt the grim trigger strategy. In that case, the outcome is (−1, +3) in each period; thus, the hospital receives the total payoff from the infinitely repeated game equal to
In such an initial situation, the patient would have no incentives to unilaterally deviate from the choice of “no foreign body ingestion” because otherwise, the patient would receive a stream of benefits (−1, +2, +2, . . .). Thus, the patient’s payoff would be
Let us consider the hospital’s incentives. Should the hospital deviate to “endoscopy” at t = 0, then in all subsequent periods it continues with “endoscopy” and the patient switches to “foreign body ingestion” from t = 1 on. Such behavior on the hospital’s part results in the following stream of its payoffs: (0, −2, −2, . . .) whose total value is

It means that the hospital cannot increase its payoff by deviating to “endoscopy” if and only if
Conclusion
Thus, we conclude that for
Footnotes
Acknowledgements
None.
Author contribution
J.P.: dynamic model formulation, manuscript writing. M.P.: conception, literature review, editing and critical revision of the article, and the final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institutions do not require ethical approval for reporting individual cases or case series.
Informed consent
No information on individual patients is contained in this article, so written informed consent was not necessary to be obtained from the patients for their anonymized information to be published in this article.