
Abstract
Purple urine bag syndrome is a rare albeit alarming purple discolouration of the urine typically seen in elderly ladies with constipation, urinary tract infection and concurrent urinary catheterisation. In this concise review, we report the pathophysiology of this condition and the case of one patient who developed this interesting phenomenon.
Introduction
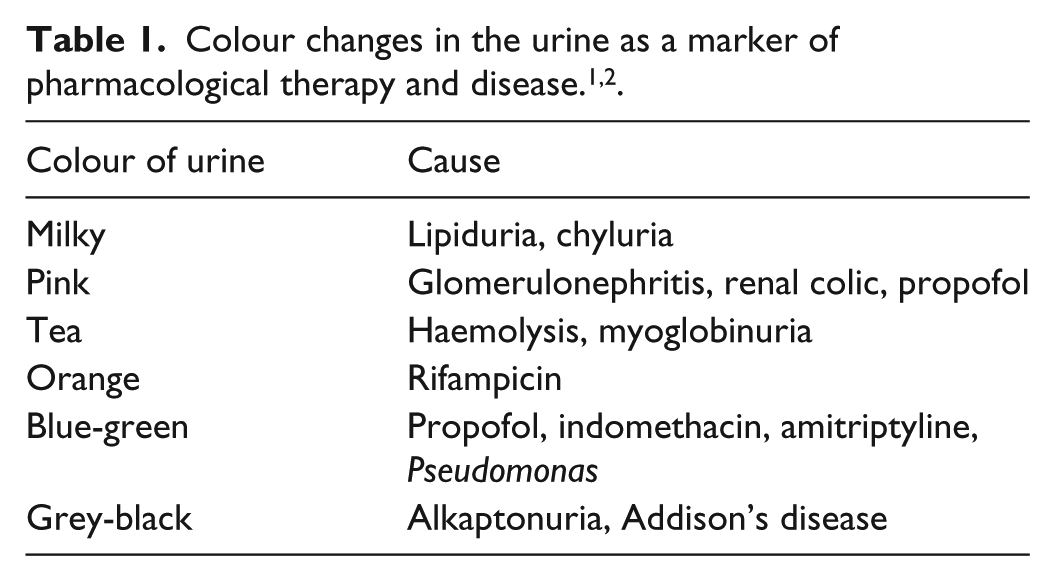
Visual inspection of the urine is an important method by which systemic disease can be diagnosed with clinician awareness needed especially when secondary to drug therapy (Table 1). While many colours of urine have been described with commonly encountered aetiologies, purple urine remains a striking and atypical occurrence, one which can lead to misdiagnosis, and inappropriate treatments yet has no obvious differential diagnosis. 3 Purple urine bag syndrome (PUBS) is a rare urinary disorder that was first characterised in 1978, although it is thought that in 1812, King George III suffered a similar complaint.4,5 This condition, while infrequent, is usually seen at the extreme of ages with paediatric cases described in the context of intussusception. As well as the similar albeit rare autosomal recessive disorder Drummond syndrome (blue diaper syndrome), in which tryptophan absorption and metabolism is affected with excess indoles produced in the urine. 6 However, the clear majority occurs in the traditionally described elderly geriatric patients who are bedridden with underlying constipation, urinary catheterisation and urinary tract infection (UTI). It is important to remember that catheter-associated UTI is the most common cause of infection in all healthcare facilities, and this intervention, while common and effective, undermines the methods by which the bladder aims to protect against infection with biofilm formation, residual bladder urine (~100 mL) below the level of the catheter and altered urethra urinary flow key reasons why their use and the complications they cause culminate to about £10,000 per annum per patient. 1 It is important to note that PUBS has been described in other patient groups. These include haemodialysis patients in whom the pigment indoxyl sulphate is albumin-bound and therefore not amenable to dialysis. In addition patients with nephrostomy tubes and urinary diversion procedures are at risk. However these remain a minority of cases and are often linked to urine acidity.3,4
Unlike traditional UTIs, those associated with PUBS are more likely to be asymptomatic but on culture may show significantly higher bacterial loads (1–2 logs) than those without the syndrome. 2 This latter point is important, as this leads to greater levels of the necessary bacterial sulphatases and phosphatases necessary for PUBS.
In one systematic review looking at the epidemiological trends of PUBS between 1980 and 2016 with 116 patients, it was shown that the cases of male PUBS are almost equal to female cases even though overall UTI rates remain significantly higher in the latter. In addition, there was no significant difference in culprit organisms between genders in catheter associated UTIs causing PUBS over this time, with 11.8% of cases presenting with fever or hypotension and ~20% of patients having underlying diabetes mellitus. Overall mortality rate was 6.8%. 7
Case
A 94-year-old lady with a background of cerebrovascular accident, chronic constipation and macular degeneration with a three times daily package of care was admitted to a hospital geriatric ward following a 2-week history of progressive confusion that had alarmed the relatives. On admission, abbreviated mental test (AMT) was 4/4 with no signs in the history of infectious symptoms or fall. Examination revealed a palpable bladder with a residual volume of 1000 mL that was secondary to both UTI confirmed by urine dipstick analysis that subsequently showed mixed growth on urine culture including Escherichia coli (white cells on culture >100 × 106/L) and constipation. The patient’s clinical condition improved following catheterization, trimethoprim and regular laxative use. After 1 week, the patient had a trial without catheter. Unfortunately, this failed after a post-void residual volume of 750 mL was noted. The patient was re-catheterized, and 2 weeks following this, purple discolouration to the urine was reported by experienced nursing staff who had never witnessed this phenomenon. The patient, during this event, complained of no dysuria. Urine dipstick analysis revealed alkaline pH of 7.2 and increased white blood cells (WBCs), and repeat culture revealed similar findings to the initial urine culture with mixed growth including E. coli noted. Further antibiotics were not prescribed and instead laxative administration and catheter exchange took place. The discolouration resolved within 2 days.
Discussion
It is hypothesised that the pathogenesis of PUBS is due to the bacterial decomposition of dietary tryptophan in the gut lumen to indole, pyruvic acid and ammonia. Upon entry into the liver, indole is conjugated into indoxyl sulphate which is filtered by the kidney. Upon exposure to genitourinary bacteria expressing sulphatase and phosphatase enzymes, it is further metabolised to indigo (indicans).4,8 Constipation is considered a key factor in this process, as it prolongs bowel transit and therefore tryptophan metabolism leading to elevated levels of urinary indole. 9 Indeed, studies looking into serum levels of amino acids in patients with PUBS found them to be significantly reduced, suggesting decreased colonic motility and bacterial overgrowth. 10 Importantly, this enzyme is most active in the presence of alkaline urine, although cases of PUBS in acidic urine have been noted. 11 However, key laboratory findings include urinary pH ⩾ 7, visual inspection of the urine and urine culture of culprit organisms. 12 Several bacteria, the majority of which are gramme negative, have been linked to the development of indicans such as Pseudomonas aeruginosa, E. coli, Proteus mirabilis, Providencia rettgeri, Klebsiella pneumoniae, group B strep and Proteus vulgaris with a mixture of these species usually present in urinary isolates in PUBS with not all organisms of the same species capable of producing the sulphatase and phosphatase enzymes. While indicans do not impart a purple colour to the urine on their own, when they are exposed to air, they are oxidised to form both indigo (blue) and indirubin (red) and react with the plastics of the polyvinylchloride (PVC)-containing catheter bag to form the purple colour observed. Without this reaction between the indigo/indirubin and the PVC bag, the urine may be dark brown or turbid.3,6,13–15
There are case reports however of PUBS developing in the setting of no known risk factors. With notions that certain laxatives (suppositories) may predispose to colonic mucosal inflammatory changes which lead to an environment that lends itself to PUBS. 16
In terms of the time until its development in catheterised patients, it may occur within hours or days of catheter insertion, with a prevalence of 9.8% in chronic care units, 8% in patients with chronic indwelling catheters in a 2-year period, 27% in dementia patients and up to 42.1% in a nursing home setting.2,13,17 However, while it seems common in some settings, there is a huge scope for misdiagnosis, as many urinary colours are described in the literature with an array of causes including haemoglobinuria, food dyes, porphyria and drugs including indomethacin, flutamide and mitoxantrone. 18 As such, it is no surprise that there is now a new Oxford Urine Chart to aid the physician and nursing staff with the spectrum of colours they may see. However, no consistent causes of purple urine are described in the literature. As such, key features of PUBS that one should consider in the history and examination is that the urine colour change should be noted only on exposure to the air, the exclusion of blackberries, beets etc from the diet and a review of the patients prescriptions. Key investigations in suspicion of PUBS should be urine dip, urine microscopy and review of urea and electrolyte, as dehydration contributes significantly to serum indoxyl sulphate levels. 3
However, the presence of PUBS has not been found to have any prognostic impact in those who develop it. That being said, it does have a high relative morbidity versus UTIs where PUBS does not features, this is not due to its associated conditions but the rare cases in the literature where PUBS has been the first sign of Fournier’s gangrene, particularly in immunosuppressed patients who will require urgent debridement and one case of PUBS that became complicated into multidrug resistant vulvar abscess.19–21 Recently, a case was reported about recurring PUBS over a 2-year period in a 29-year-old female patient with ileal diversion who featured both benign and severe features of the condition requiring Intensive Care Unit input with treatments such as meropenem and levofloxacin required due to underlying antibiotic resistance. Indeed, it is due to the often-benign presentation of this disorder which does not prompt treatment and the underlying antibiotic resistance of culprit organisms that rare cases of death have been associated with PUBS.22,23
Regardless, PUBS is a very striking event, one which is underappreciated by many medical professionals and concerning to family members especially, as it often affects elderly patients, and as such, counselling patients about the benign process it represents is key as well as educating patients regarding the possibility of developing PUBS. This is important, given the changing demographics in the British population with the geriatric population becoming more significant with each year. This may also be important particularly in palliative patients, where opioid therapies predispose to constipation and where holistic management more than in other settings is required. 24
At present, in most cases, it remains the clinician’s choice whether antibiotics are used for its resolution as no guidelines regarding its management exist, indications for antibiotic therapy include symptomatic UTI, sepsis and signs of contiguous areas of infection or if the PUBS persist or occurs in an immunosuppressed patient.3,14,17 In all instances, however, medical management includes the treatment of underlying constipation and good catheter care including exchange in order to not only to prevent PUBS but also bring about its resolution. This latter point is something which the literature highlights is not always done but is demonstrated well in this case.3,24
Conclusion
PUBS is an uncommon albeit striking manifestation of urinary catheterization and UTI in geriatric patients. Key to its pathogenesis is the metabolism of tryptophan to indoles and their metabolism by urinary bacteria to indigo and indicans, which is precipitated by underlying slow bowel transit. While benign this condition may in immunosuppressed patients be, the first signs of more concerning disease processes and in otherwise healthy patients may cause significant anxiety. It would seem prudent that awareness of this condition is needed to avoid unnecessary investigation and antibiotic use. As such, clinicians should seek to educate patients who may require long-term catheterisation the likelihood of developing PUBS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorised representative(s) for anonymized patient information to be published in this article.