
Abstract
Background:
Urinary tract infection is a common infection posing a significant healthcare burden globally. Currently, it is becoming hard to manage due to the drug resistance of uropathogens. This study aimed to evaluate the rate of culture positivity and the susceptibility pattern of isolates among clinically diagnosed patients with urinary tract infection.
Methods:
An institution-based cross-sectional study was conducted on patients clinically diagnosed with urinary tract infections and received a drug prescription at Hiwot Fana Specialized University Hospital from August 2018 to June 2019. A clean-catch mid-stream urine specimen was collected and bacterial identification and susceptibility test were performed using standard microbiological methods. Data were entered into EpiInfo 7 and exported to STATA 15 for analysis. Data were analyzed using descriptive analysis and bi-variate and multivariate regression analyses and presented with graphs, frequency, and tables.
Results:
A total of 687 urine samples were collected from patients with clinically diagnosed urinary tract infections. The mean age was 31 years and 56.62% were female. 28.38% of the participants had a culture-positive result, of which 86.15% had monomicrobial infections. Inpatients (AOR = 3.8, 95% CI = (1.8–7.9)) and hypertensive patients (AOR = 2.1, 95% CI = (1.1–4.4)) had higher odds of culture-positive results. Staphylococcus species (35.3%), E. coli (25.34%), Pseudomonas species (6.8%), and other Enterobacterales are isolated. Most isolates showed resistance to more than one drug, and amikacin, gentamicin, and nitrofurantoin showed relatively higher activity against isolates.
Conclusion:
About one-third of the clinically diagnosed patients with urinary tract infection were culture-positive with many types of bacterial uropathogens. Inpatients and hypertensive patients had a higher risk of developing bacterial infections. Bacterial isolates showed different percentages of susceptibility to the tested antibiotics.
Background
The presence and growth of bacteria anywhere in the urinary tract, kidney, ureter, bladder, and urethra can cause urinary tract infections (UTIs). 1 UTI can be lower (cystitis) or upper (pyelonephritis) UTI based on the patient’s clinical presentation. Patients with pyelonephritis may require hospital admission for treatment with intravenous antibiotics, unlike cystitis. 2 UTI is a common bacterial infection in humans, affecting more than 150 million people and requiring an enormous antibiotic expenditure annually.3–5 Traditionally, many people perceive UTI as a disease of women as more than 50% will develop an infection in their lifespan, although men are also affected. 4
UTI is challenging to differentiate from other diseases with the same clinical picture, particularly in need of rapid treatment decisions, and there is limited diagnostic capacity. 6 Physicians often rely on less sensitive and specific laboratory or point-of-care tests such as urinalysis to confirm clinical decisions for empirical treatment. 7 The culture-based test can have a profound effect on the era of antimicrobial resistance by identifying the microbial cause and guide the choice of antibiotic therapy. The known drawback of a culture-based test is a long turnaround time, at least 48 h, which makes it inconvenient as patients may recover or leave the hospital by the time. 8
Various bacterial pathogens with arrays of clinical presentation can be associated with UTI. Etiologies include E. coli, Staphylococcus species, Enterococcus species, Klebsiella species, Enterobacter species, and Proteus species, especially during catheter-related and nosocomial infections.9,10
The emergence of resistant bacterial strains has challenged the current therapies to treat and control the spread of infections, 11 and treatment has not advanced and does not prevent re-infections. 12 Resistance to fluoroquinolones, a frequent treatment for UTI, has also increased, as is the prevalence of multidrug-resistant (MDR) Pseudomonas aeruginosa and extended-spectrum-beta-lactamase (ESBL)-producing Enterobacterales.13–15 Recently, carbapenem-resistant Enterobacterales have emerged and gradually became a significant public health challenge. 16 In third world countries, the problem immense as most healthcare facilities has no culture-based diagnostic facility. 17
Proper empirical medication is necessary for successful treatment and to prevent complications of UTI. However, with the increasing prevalence of antibiotic-resistant urinary pathogens, the selection of appropriate empirical therapy is increasingly challenging.18,19
Methods
Study setting, design, and period
A cross-sectional study was conducted at Hiwot Fana Specialized University Hospital, Harar, Ethiopia, from October 2018 to June 2019. Currently, the hospital is a teaching hospital under Haramaya University College of Health and Medical Sciences and serves as a referral hospital for the eastern part of Ethiopia.
A sample size of 651 patients was determined, with an assumption of 36% prevalence, 20 80% power, 0.05% margin of error, and a design effect of 1.5. During the study period, 687 patients were diagnosed as UTI patients and received a drug prescription.
Data and specimen collection
The questionnaire (Supplementary material) was developed after reviewing different literature studies,21–23 translated into the local language (Afan Oromo and Amharic), and pretested 5% of the sample size at Jugol Hospital. The variables include sociodemographic characteristics, prescribed drugs, infection history, admission information, and comorbidities. The urine sample was collected from each participant using a sterile leak-proof container aseptically. Urine samples from catheterized inpatients were collected using a sterile syringe from the catheter. The samples were transported to the Bacteriology Laboratory at Haramaya University College of Health and Medical Sciences within 30 min of collection 24 in a cold box.
Isolation and identification of bacteria
Isolates were identified and characterized following the Cheesbrough 25 culture and biochemical test recommendation. Urine samples were inoculated on cysteine lactose electrolyte deficient (CLED) agar and 5% blood agar (HIMEDIA Ltd., India) plates 26 using a 1-µm calibrated loop. After overnight aerobic incubation at 37°C, colony morphology and biochemical reactions, including sugar fermentation, gas, H2S production, amino acid utilization, catalase, oxidase, urease, indole, citrate utilization, coagulase, and motility tests, were used for phenotypic characterizations (Supplementary material). A colony count of ⩾104 CFU/mL (colony forming units per milliliter) was labeled as significant bacteriuria. 27
Antimicrobial susceptibility testing
The Kirby–Bauer disk diffusion method, based on the Clinical and Laboratory Standards Institute (CLSI) recommendation, 28 was used for susceptibility testing. The suspension of bacterial inoculum, equivalent to 0.5 McFarland standards, was uniformly spread on Mueller–Hinton agar (HIMEDIA Ltd., India) plates using a sterile applicator cotton-swab.
Cefotaxime (30 µg), cefoxitin (30 µg), ceftazidime (30 µg), ceftriaxone (30 µg), chloramphenicol (30 µg), trimethoprim-sulfamethoxazole (1.25/23.75 µg), cefepime (30 µg), erythromycin (15 µg), clindamycin (2 µg), oxacillin (1 µg), cefazolin (30 µg), meropenem (10 µg), cefuroxime (30 µg), vancomycin (30 µg), azithromycin (15 µg), rifampin (5 µg), gentamicin (10 µg), ciprofloxacin (5 µg), amikacin (30 µg), tobramycin (10 µg), nitrofurantoin (300 µg), amoxicillin/clavulanic acid (augmentin) (20/10 µg), penicillin G (10 UI), kanamycin (30 µg), amoxicillin (10 µg), and tetracycline (30 µg) are tested.
Gentamicin, ciprofloxacin, amikacin, tobramycin, nitrofurantoin, amoxicillin/clavulanic acid (augmentin), penicillin G, kanamycin, and amoxicillin were used for all isolates and others for the selected group of isolates. The interpretative guidelines set by the CLSI 28 were used to interpret results as sensitive (S), intermediate (I), or resistance (R). Bacterial isolates resistant to three or more antimicrobials belonging to the different structural classes were considered MDR. 29
Quality control
To assure questionnaire accuracy, the English version was translated into local languages (Afan Oromo and Amharic), and vice versa, by separate language experts and pretested at Haramaya General Hospital. Data collectors (laboratory personnel and nurses) were trained regarding all stages of the data collection process. Performance of culture medium and drug disks was checked using reference strains such as S. aureus (American Type Culture Collection (ATCC)® 25923), P. aeruginosa (ATCC ® 27853), and E. coli (ATCC ® 25922).
Data analysis
Data were checked for completeness, coded, and entered into the EpiInfo software (version 7.2.; Centers for Disease Control and Prevention (CDC)) and exported to the STATA 15 for analysis. Descriptive statistical tools were used to summarize findings. Logistic regression models were used to predict the correlation between the dependent and the independent variables. The multivariate logistic regression model includes variables with a p-value ⩽ 0.25 in the bivariate logistic regression. Crude and adjusted odds ratios with a 95% confidence interval (CI) were used to sign the predictors, and a p-value less than 0.05 in the multivariate analysis was used as a cutoff value. The Hosmer–Lemeshow’s goodness-of-fit test was applied to check the assumption of the model. Educational status was included after removing participants below 5 years of age.
Ethical consideration
The Institutional Health Research Ethics Review Committee of the College of Health and Medical Sciences, Haramaya University, has approved the study (No. IHRERC/078/2017). Each study participant/guardian gave written informed consent before data collection, and personal information was kept confidential.
Result
Sociodemographic character
A total of 687 study participants (56.62%, 389 females) were diagnosed with UTI and received drug prescriptions. The mean age was 31 years with a minimum of 3 days and a maximum of 80 years, 18.78% of the participants were below 20–25 years of age, and the majority (55.1%) of the participants live in rural areas (Table 1).
Characteristics of patients diagnosed with UTIs at HFSUH, Harar Ethiopia (2018–2019).

UTIs: urinary tract infections; HFSUH: Hiwot Fana Specialized University Hospital.
A total of 84 (12.23%) participants were pregnant women and 3.64% were children below 5 years of age (Figure 1).

Age-group distribution of patients diagnosed with UTIs at HFSUH, Harar Ethiopia (2018–2019).
Of all the participants, 57 (8.3%) were inpatients admitted for a mean of 10 days (95% CI = 8–12 days), and 191 (27.8%) participants had comorbidity, of which 16 participants had more than one comorbid condition. Of the comorbidity, 164 had a renal problem, followed by pregnancy and hypertension (Figure 2).

Comorbidity among patients diagnosed with UTIs at HFSUH, Harar Ethiopia (2018–2019).
Prevalence of UTIs
A total of 195 (28.38%) participants had culture-positive results. Most of them had a monomicrobial infection (86.15%), and the rest (13.85%) had a polymicrobial infection. Totally, 221 bacterial pathogens were isolated: E. coli was the leading pathogen 56 (25.34%), followed by S. saprophyticus, S. warneri, coagulase-negative Staphylococci (CoNS), and Pseudomonas spp. Members of the Gram-negative bacteria have a higher prevalence, accounting for 62% of the isolates (Figure 3).

Bacterial isolates from patients diagnosed with UTIs at HFSUH, Harar Ethiopia (2018–2019).
Risk factors
On univariate regression analysis, history of catheterization, hypertension, previous infections, and being an inpatient had a significant association with UTI. On multivariate analysis, hypertension, being an inpatient, and educational status had a significant association with culture-positive results.
Based on the analysis, hypertensive patients are two times more likely to have culture-positive results than non-hypertensive patients. Being an inpatient increased the odds of developing a culture-positive infection by more than three times, and participants who achieved secondary education had two times more odds than those who cannot read and write (p = 0.003) and those who have completed primary education (p = 0.007). Even though the association was not significant, participants with a history of catheterization showed higher culture-positive results (p = 0.053) (Table 2).
Association of sociodemographic and clinical characteristics with culture-positive results of patients, Harar Ethiopia (2018–2019).

reference; AOR: adjusted odds ratio; COR: Crude odds ratio; CI: confidence interval.
Susceptibility testing
The test was performed on 221 isolates. Of those drugs, amikacin, gentamicin, and nitrofurantoin had higher activity than the other drugs with a susceptibility pattern of 69.2%, 61.1%, and 55.7%, respectively. Cefotaxime, cefazolin, cefuroxime, and ceftriaxone were tested only for Gram-negative isolates, and all of those drugs were not effective for the majority of the isolates with susceptibility less than 35%. Drugs like erythromycin, chloramphenicol, clindamycin, rifampin, and azithromycin were tested for Gram-positive isolates, and isolates showed higher susceptibility to rifampin (70.1%) and azithromycin (51.7%), and erythromycin being less effective with 31.7% susceptibility. Overall, penicillin, amoxicillin, and trimethoprim-sulfamethoxazole showed the highest rate of resistance (Figure 4). There is a high degree of multidrug resistance as shown in Table 3, and 24 isolates have resistance to five commonly used antibacterial drugs.

Antibiogram of isolates from urinary tract infections at HFSUH, Harar Ethiopia (2018–2019).
Multidrug resistance of isolates from urinary tract infections, Harar Ethiopia (2018–2019).
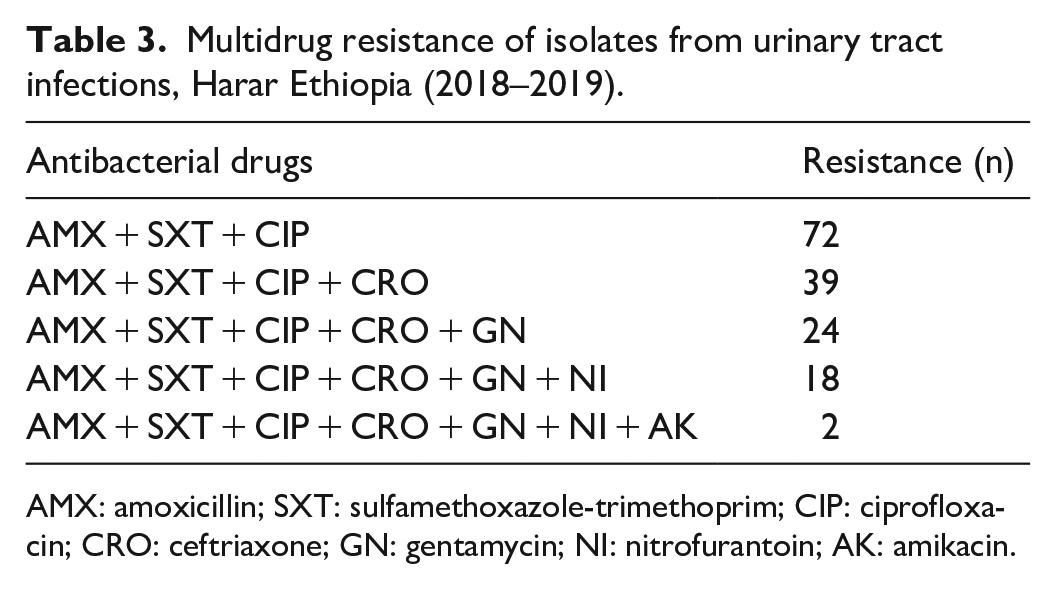
AMX: amoxicillin; SXT: sulfamethoxazole-trimethoprim; CIP: ciprofloxacin; CRO: ceftriaxone; GN: gentamycin; NI: nitrofurantoin; AK: amikacin.
Discussion
UTIs and other preventable diseases are devastating to the lives of ordinary citizens in communities with limited resources. The situation becomes even complicated with an underlying chronic condition and resistant microorganisms to the routine treatment regimen. 30
In this study, 28.38% of the participants had a culture-positive result, which is in conjunction with other studies in Ethiopia.20,31,32 Some studies have reported a higher rate of culture-positive UTI. 23 The disparity between studies could result from the difference in sample size, type of study population, methodology, length of the study period, and definition of bacteriuria. Most of the study participants had received ciprofloxacin therapies (77.44%); this is because most of the study participants (91.7%) were outpatients and in Ethiopian standard drug therapy regimen, ciprofloxacin is one of the first-line drugs for community-onset UTI. 33 Amoxicillin prescription is usually for UTI in pregnancy and only 12.08% of the study participants received the therapy.
Inpatients were two times more likely to have culture-positive results than outpatients. Inpatients are categorized as having a hospital-acquired infection, as the mean number of days from admission is 10 days, and more than half (52.6%) of the clinically diagnosed hospital-acquired urinary tract infection (HAUTI) were culture-positive compared to community-onset UTI (30.3%). It can be because inpatients are prone to infections due to their deteriorated health condition, and microbes in a hospital setting are resistant to commonly used drugs as well as equipped with various virulence factors as well the frequent isolation of Proteae among inpatients.34–36 The other explanation could be, an overactive bladder and interstitial cystitis/bladder pain syndrome have a similar clinical picture with UTI (urgency, pain, pressure, or discomfort), and it could end up with a diagnosis of UTI clinically but will not have a culture-positive result. 1
In the current study, having any comorbidity, in general, has no significant association with culture-positive results. Diabetes, pregnancy, and renal problems have no statistically significant association with UTI, but hypertension has a significant association, and hypertensive patients are two times more likely to have culture-positive results. It could be due to the effects of hypertension with kidney disease. 37 This finding is in contrast to other studies.23,38–40 These variations could be attributed to social, environmental, economic, and healthcare-seeking behavioral differences.
A study in the United Kingdom has indicated that patients with diabetes mellitus (DM) have a four-time risk of developing UTI than non-DM group. 41 Even though pregnancy was not significantly associated with culture-positive results, 27.4% of the pregnancy cases were culture-positive. It is higher than a study from Nigeria 41 and Ethiopia,42,43 and comparable with other studies in India 44 and Ethiopia. 45 Pregnancy is mostly considered as one of the risk factors for UTI as it has hormonal and physiological changes in a mother. Differences in the environment, social habits, standard of personal hygiene, or low economic status of the study participants may cause the variation.
On analysis, previous UTI history has no significant association with culture-positive results, unlike some other studies.45–47 Infection recurrence is common in UTI, and previous UTI is one of the risk factors for UTI.48,49 Previous studies23,46 have indicated that females have higher culture-positive results, even though in our study, gender has no statistically significant association. It is probably due to multiple factors, including the shorter urethra of females that allow easy access to the bladder during sexual intercourse and increasing bacterial counts in the bladder. 50 The variation could be due to differences in cultural, religious, and hygienic practices 23 among females in different geographical locations.
A higher number of patients with catheter-usage history were culture-positive without statistically significant association. Similar findings were observed in the study by Seifu and Gebissa, 23 whereas a significant association was reported by Gebremariam et al. 46 As it creates an additional portal for bacterial invasion and moves bacteria into the bladder, catheter placement increases the risk of UTI. 51
The renal problem is one of the risk factors for UTI by other studies in contradiction to this study. Kidney problems, like glomerulonephritis, calculi, and genetic abnormality of kidneys, are the major predisposing factors for UTI. 52 This discordance could be due to the follow-up of those patients with a renal problem to healthcare settings in response to the raised health education and media coverage.
Though Gram-negative rods are commonly reported from UTI, the pathogenic spectrum could vary with study area, population, and time. Similarly, out of 221 isolates in this study, 62% were Gram-negative bacteria unlike the study of Habteyohannes et al., 43 which has reported 74.1% Gram-positive isolates. However, a similar finding was reported from other studies.32,46,53 E. coli was the leading pathogen (25.34%) which is comparable with the study of Glaser and Scheaffer. 54 Some reports have indicated a higher isolation rate of E. coli: 46.4%, 45 39.3%, 23 and 52.7%. 20
S. saprophyticus, S. warneri, CoNS, and Pseudomonas spp were the other dominant isolates in the current study. Staphylococcus spp has been indicated as principal isolates by some other reports,20,36,45,46 whereas S. aureus was indicated by the studies from Arba Minch (Ethiopia) 32 and Adigrat (Ethiopia), 55 and CoNS from Hawassa (Ethiopia). 56 Pseudomonas spp was identified as the second type of Gram-negative isolate in our study compared to that of Abejew et al., 31 whereas other studies reported K. pneumoniae or Klebsiella species.17,32,53,57,58 Some studies have reported the isolation of Leuconostoc spp, Salmonella typhimurium, 23 which is absent in our case. Environmental conditions and frequent practices in different regions could be the cause of discrepancies in the distribution and type of uropathogens.
In agreement with the study of Seifu and Gebissa, 23 our study also showed that polymicrobial infections in 13.5% of the samples had polymicrobial isolates, which are higher than the research from Mekelle. 46 Disorders that interfere with urine flow and indwelling catheter contribute to the development of polymicrobial infections.
Healthcare personnel’s ability to choose proper treatment for UTI has been affected by growing antibiotic resistance. In this study, there was 91% resistance to amoxicillin and 97% to penicillin G, and a similar result was reported by several studies.32,57–59 Amoxicillin resistance was far higher than in the developed world, for example, in Europe, resistance ranges from 48% (The Netherlands) to 60% (Belgium) for amoxicillin. 60 The difference could be due to prescribing rate, antibiotic use, and patient population.61,62 Unlike in this report, some studies have indicated that ceftriaxone and ciprofloxacin were more effective.46,55,58 Inadequate treatment can add to further drug resistance due to inappropriate antimicrobial use. 63
Gentamicin and amikacin were more effective for Gram-negative and Gram-positive isolates, same with some studies.23,31 Contradicting results from a study in Ethiopia for Gram-negative isolates 46 were observed. It might be due to the unavailability of tablet forms for gentamicin and amikacin in the community, which minimized the chance to misuse.
E. coli has high resistance (64.3%) to ciprofloxacin, commonly prescribed to UTI in the study area. A similar finding has been reported from Saudi Arabia, 64 though other studies reported contradicting results.31,46,53 E. coli was more susceptible to meropenem (92.8%) and gentamicin (75%), similar to a report by Al-Mijalli. 64 However, ceftriaxone, cefuroxime, cefotaxime, and ceftazidime were more effective for E. coli by some studies.20,53,65
Our study identified that many isolates are resistant to two and more drugs, in conjunction with others from Ethiopia.31,53,66 Around 11% of isolates were resistant to five common drugs: amoxicillin, trimethoprim-sulfamethoxazole, ciprofloxacin, ceftriaxone, and gentamicin. Prolonged exposure and repeated use of antibiotics could have led to higher resistance of isolates. 67 Gram-positive isolates have shown more resistance to erythromycin comparable to the report by Merga Duffa et al. 53 Repeated use of antibiotics can also predispose to UTIs by damaging peri-urethral flora, allowing colonization by uropathogens. 68 Moreover, this condition allows exchanging their genetic material horizontally, enabling them to be more resistant.
Limitations of the study
In addition to assessing several factors, a large sample size and drug susceptibility testing for various antibacterial agents are the strengths. One major limitation is the inability to identify some bacterial isolates into species and serotypes. The use of conventional tests, which are less accurate than 16s rDNA sequencing or API-20E, is the other limitation. Furthermore, the study could not indicate ESBL and CRE isolates due to a lack of resources.
Conclusion and recommendation
About one-third of the clinically diagnosed UTI patients were culture-positive in this study. Inpatients and hypertensive patients were at higher risk of developing bacterial infections. Many types of bacteria were isolated, mainly E. coli, Staphylococcus species, Pseudomonas spp, and other Enterobacterales. These strains showed different percentages of susceptibility to the tested antibiotics. The current study points out that amikacin, gentamicin, and nitrofurantoin are a choice of drugs for UTI in the study area. The majority of the isolates have shown multidrug resistance, especially to commonly used drugs. As patients are diagnosed and treated empirically in the study setting, Hospitals should establish antimicrobial stewardship programs. Patients should be managed with microbiological evidence to avoid antimicrobial prescriptions for patients without bacterial infection and better control the spread of drug resistance. The careful prescribing practice of antibiotics is needed to halt the progress of drug resistance. Trends of antibiotic resistance, change in local antibiotic policies, and rational antibiotic therapy can be attained by continued surveillance. Patients with hypertension, catheter, and inpatients have a higher chance of culture-positive results. Particular attention should be given to patients with comorbidities, as they are prone to bacterial UTI.
Supplemental Material
sj-xlsx-1-smo-10.1177_20503121211001162 – Supplemental material for Bacterial uropathogens and susceptibility testing among patients diagnosed with urinary tract infections at Hiwot Fana Specialized University Hospital, Eastern Ethiopia
Supplemental material, sj-xlsx-1-smo-10.1177_20503121211001162 for Bacterial uropathogens and susceptibility testing among patients diagnosed with urinary tract infections at Hiwot Fana Specialized University Hospital, Eastern Ethiopia by Tewodros Tesfa, Yohannes Baye, Mekonnen Sisay, Firehiwot Amare and Tigist Gashaw in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121211001162 – Supplemental material for Bacterial uropathogens and susceptibility testing among patients diagnosed with urinary tract infections at Hiwot Fana Specialized University Hospital, Eastern Ethiopia
Supplemental material, sj-docx-2-smo-10.1177_20503121211001162 for Bacterial uropathogens and susceptibility testing among patients diagnosed with urinary tract infections at Hiwot Fana Specialized University Hospital, Eastern Ethiopia by Tewodros Tesfa, Yohannes Baye, Mekonnen Sisay, Firehiwot Amare and Tigist Gashaw in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to express their heartfelt gratitude to Haramaya University College of Health and Medical Sciences for funding the project and the staff members of the Department of Medical Laboratory Sciences for providing genuine technical and laboratory support. They also thank the staff members of Hiwot Fana Specialized University Hospital for their cooperation during data collection.
Author contribution
All authors had conceived and drafted the project; had substantial contributions to the study design and the development of the data collection checklist; have read and approved the final version of the document. T.T. has collected the data, and drafted and prepared the manuscript for publication.
Availability of data and materials
Data generated or analyzed during this study can be obtained from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Health Research Ethics Review Committee of the College of Health and Medical Sciences, Haramaya University (approval number: IHRERC/078/2017).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funds for data collection and laboratory analysis were obtained from Haramaya University.
Informed consent
For minors who were below 16 years of age, the parents/guardians were briefed about the study, and written and informed consent was obtained from all the participants/guardians before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.