
Abstract
Cholestasis can occur in newborns due to infections. However, the manifestations of the underlying infections usually dominate the presentation. We present a 2-month-old infant who presented with jaundice and no fever or signs of systemic illness. Liver biopsy was suggestive of cholangitis. He was subsequently detected to have urinary tract infection with Klebsiella pneumoniae. The child was treated with appropriate antibiotics for 2 weeks following which the cholestasis resolved. Thus, neonatal cholestasis due to infections can also occur in the post-neonatal period without clinical manifestations of an underlying infection.
Introduction
Sepsis is more likely to manifest with jaundice in infants and children than in adults. The primary site of infection is most often intraabdominal, but infection of various other sites such as urinary tract infection (UTI), pneumonia, endocarditis, and meningitis have been associated with this complication. 1 However, in these patients, symptoms of the infection usually predominate. Presentation of infections only as jaundice is rare. We present a 2-month-old male infant who presented with jaundice alone. He had no fever or signs of infection in the body. Subsequently he was detected to have cholangitis due to UTI.
Case report
A 2-month-old male infant presented with jaundice for 1 week with clay-colored stools and vomiting for 2 days. His mother had fever in her third month of gestation which lasted for a few days which was not associated with any rash, and she was treated with antipyretics for the same. The baby was born by caesarean section in view of meconium stained liquor with pregnancy-induced hypertension. His birth weight was 2.3 kg. He cried after stimulation and was kept under observation in the neonatal intensive care unit (NICU) for 2 days. He was exclusively breastfed.
On examination at presentation, his weight was 2.5 kg (below third centile), length was 52 cm (below third centile), and head circumference was 35 cm. His vitals were stable. He was pale, icteric. Liver was palpable 2 cm below the costal margin. Other systems were normal.
Investigations showed hemoglobin 6.3 g/dL, white blood cell count 13,000 cells/cumm (51% polymorphs, 41% lymphocytes), platelets 45,000/cumm, C-reactive protein 12 mg/L, and blood culture showed no growth. Serum total bilirubin was 7.4 mg% with a direct bilirubin of 5.1 mg%. Serum alanine transaminase was 105 IU/L, serum aspartate transferase was 97 IU/L, gamma glutamyl transferase (GGTP) was 593 IU/L, total serum proteins were 5.3%, and serum albumin was 3.4 g%. TORCH titers revealed elevated IgG levels of toxoplasma, cytomegalovirus and herpes simplex virus 1 and 2.
Ultrasound of the abdomen showed mild hepatomegaly with bright echotexture with contracted gall bladder. Liver biopsy revealed moderate neutrophilic infiltrate around the bile ductules and intraepithelial neutrophilic infiltrate. The infiltrate was seen extending into the surrounding hepatic parenchyma and at places with bile ductular reaction suggestive of ascending cholangitis as seen in Figure 1. Subsequently, urine routine examination showed 8–10 pus cells/hpf and urine culture grew Klebsiella pneumoniae (105 cfu/mL).

Portal tracts showing moderate neutrophilic infiltrate around the bile ductules and intraepithelial neutrophilic infiltrate.
The child was given a packed cell transfusion and was given intravenous (IV) antibiotics for 2 weeks based on the sensitivity pattern. Repeat urine culture showed no growth. Vitamins A, D, E, and K were given orally with oral ursodeoxycholic acid. Follow-up investigations are given in Table 1. The child was discharged and is now on regular follow-up.
Blood examination.
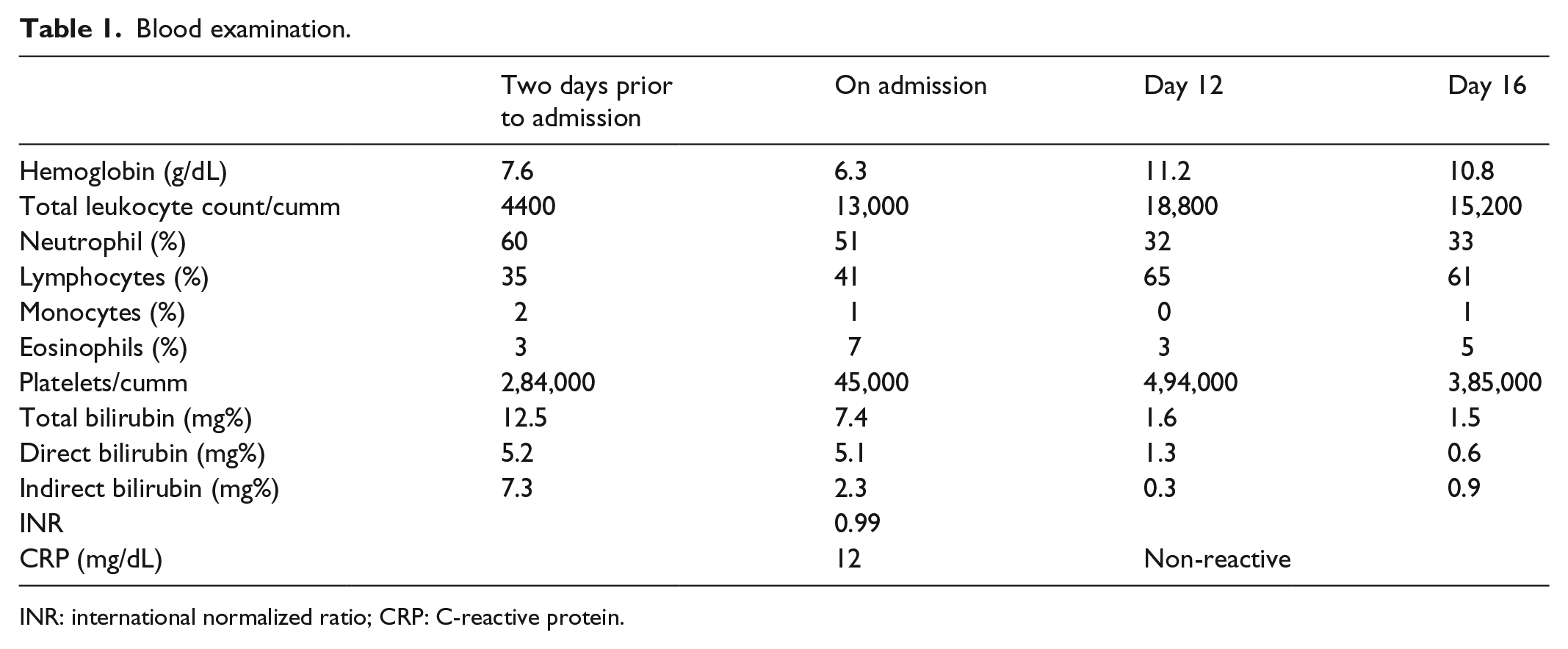
INR: international normalized ratio; CRP: C-reactive protein.
Discussion
Cholestasis is a known complication of gram-negative bacterial infections especially in infants. This syndrome is more frequent in the neonatal period and may account for as much as a third of the cases of neonatal jaundice. 2 Most cases of sepsis associated with cholestatic jaundice have evidence of gram-negative bacteremia, with Escherichia coli the more common pathogen.3,4 Pyelonephritis, peritonitis, appendicitis, diverticulitis, pneumonia, and meningitis are types of infections observed to cause jaundice. The urinary tract is the most common site of infection associated with this syndrome, especially in the neonatal period. 4 Liver histology shows intrahepatic cholestasis with Kupffer cell hyperplasia and little or no evidence of cellular necrosis. Aside from cholestasis, liver histology reveals an almost normal hepatic parenchyma. 3 In our patient, liver histology showed neutrophilic infiltrate but no obvious cholestasis. The manifestations of the underlying infection usually dominate the presentation. 5 In our patient, there were no manifestations of UTI or sepsis, rather the patient presented with only jaundice. Jaundice and cholestasis are usually reversible and subside completely after resolution of the infection. 1 In our patient too, the jaundice and cholestasis resolved after resolution of the UTI.
The principal mechanism of cholestasis during sepsis is from disruption of bile flow. Bile salts are normally synthesized in hepatocytes or reabsorbed in the intestine and imported into the hepatocytes using the sodium-dependent transporter taurocholate cotransporter and organic anion transport proteins (OATPs). Bile salts are then excreted into canaliculi by the bile salt export pump (BSEP) and multidrug-resistant protein (MRP). Similar to its effect on bilirubin metabolism, lipopolysaccharide (LPS) has also been shown to impede bile acid transport in animal models through both inhibition of transporter activities and downregulation of gene expressions.6–8
Cholestasis associated with sepsis is also attributable to impairment in bilirubin metabolism. Bilirubin is normally transported into hepatocytes by OATPs, conjugated by the uridine diphosphate–glucoronosyltransferase enzyme and excreted into bile by the canalicular multispecific organic anion transported 1 (cMOAT) or commonly known as multidrug resistance–associated protein 2 (MRP2). Endotoxin, specifically LPS, has been shown in rat model of sepsis to inhibit bilirubin uptake and excretion without significant effect on conjugation. 9 The mechanism is probably due to dysfunction of OATPs and MRP2 by endotoxemia.6,10
The presence of jaundice and sepsis or the degree of its severity does not seem to influence survival or predict the overall prognosis of the patient. 3 The overall prognosis depends on the underlying infection. There is usually complete resolution of hepatic dysfunction and cholestasis if the underlying condition is adequately treated, yet the outcome may be guarded if detection and treatment are delayed.
Conclusion
Neonatal cholestasis due to sepsis or other systemic infections can occur even in the post-neonatal period and patients may present as isolated jaundice without other manifestations of infection. Thus, a strong suspicion of systemic infections should be kept in patients with neonatal cholestasis even in the absence of toxicity or severe sickness.
Footnotes
Acknowledgements
The authors thank Dr Y.K. Amdekar, Medical Director, and Dr. Jaya Deshpande, Pathologist, Bai Jerbai Wadia Hospital for Children, Parel, Mumbai, India.
Author contribution
All authors were involved in patient management, preparation of manuscript, and approving the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from “Bai Jerbai Wadia Hospital for Children” Ethics Committee or Institutional Review Board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.