
Abstract
Knee dislocation with concomitant multiligament injury is a rare and devastating injury. We report the successful repair of a rare case of open knee dislocation with concomitant multiligament injury and patellar tendon rupture of an 18-year-old male due to a motorcycle accident. The patient presented with an open wound running parallel to the knee joint line and patellar tendon rupture with full exposure of the cartilage of the distal femur. Staged surgical management including the application of a ring-type external fixator with a hinged joint, lateral collateral ligament repair, medial collateral ligament reconstruction using autogenous hamstring tendon, and joint release was performed. Range of movement was recovered to 0 degrees of knee extension and 80 degrees of knee flexion, and extension lag was negative. The Lysholm score of the patient was recovered to 92. The patient was able to return to work in the construction field 2 years after sustaining the injury. The patient had no complaint of pain and was able to resume construction work, even though reconstruction of the anterior cruciate ligament and posterior cruciate ligament was not performed. The application of a hinged ring-type external fixation device might play a key role in early range of movement restoration and to maintain the reduced position and acceptable recovery of the posterior cruciate ligament injury without the need for reconstructive surgery. This report is the first to describe the safety and effectiveness of staged surgical management for the repair of open knee dislocation with concomitant multiligament injury and patellar tendon rupture. However, further studies with longer follow-up periods will be needed to observe the development of osteoarthritis or weakness of the knee. Staged surgical management is a safe and effective procedure for repairing an open knee dislocation with concomitant multiligament injury and patellar tendon rupture.
Introduction
Knee dislocation with concomitant multiligament injury (MLI) is a rare and devastating injury that accounts for approximately 0.02% of all musculoskeletal injuries.1,2 Rupture of the patellar tendon is also a severe injury that requires a long recovery period and results often in functional limitations, such as extension lag or flexion loss. 3 A search of the literature retrieved a few reports only of patellar tendon rupture (PTR) with injury to the anterior cruciate ligament (ACL) or medial collateral ligament (MCL),4–7 but no reports of open PTR with knee dislocation. Here, we report a rare case of open knee dislocation with concomitant MLI and PTR sustained in a motorcycle accident.
Case presentation
An 18-year-old male who was involved in a motorcycle accident had sustained knee posterior dislocation with an open wound and was transferred to the Emergency Department of another institution. Clinical and radiological evaluations performed at that institution identified an open wound running parallel to the knee joint line and PTR. The cartilaginous area of the distal femur was fully exposed, but the open wound was not severely contaminated (Figure 1). In spite of posterior knee dislocation, computed tomography angiography found no obvious arterial injury (Figure 2). Surgical debridement, irrigation, and external fixation (EF) were performed (Figure 3).

Open scar at the time of injury.

CT angiography at the time of injury.

Postoperative X-P after external fixation (EF) was applied.
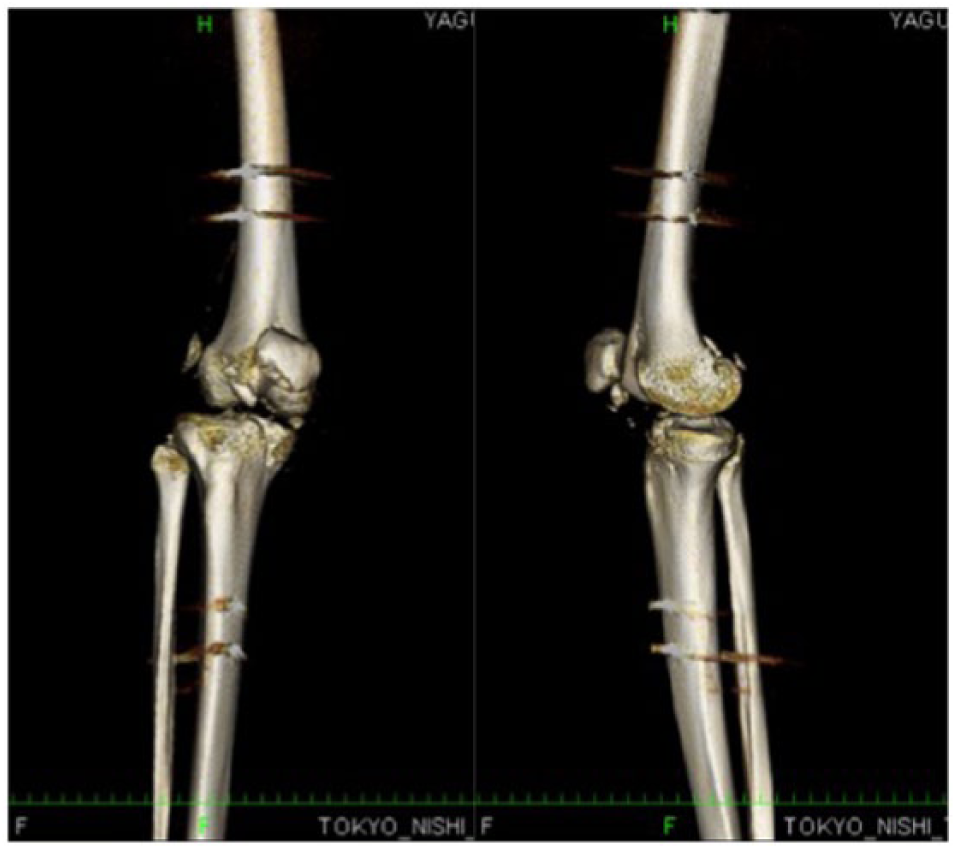
The patient was transferred to our trauma center on post-injury day 16. Upon admission, he complained of pain, numbness, and paresthesia along the lateral branch of the peroneal nerve. Radiological evaluation revealed small fragments of the distal patella and an insufficient reduction of posterior translation. In addition, the posterior translation of the tibia relative to the femur was >10 mm (Figure 4). Therefore, surgical debridement and manual reduction under general anesthesia after the temporary release of the EF were performed, which achieved an appropriate reduction (Figure 5).

Radiological evaluation of residual posterior translation of tibia relative to femur.
Postoperative CT following a reduction which achieved an appropriate reduction.
The first surgical procedure
The first surgery was performed on post-injury day 24. Injuries to the ACL and posterior cruciate ligament (PCL) were observed from the open wound, while varus–valgus instability with the knee extended was also confirmed under general anesthesia. The surgeon made a longitudinal skin incision along the medial proximal tibial and the ipsilateral semitendinosus (ST) and gracilis (G) tendons were harvested, while maintaining the distal attachments. The G tendon was sutured to the proximal end of the ruptured deep layer of the MCL as an augmentation. Next, a skin incision was made along the lateral collateral ligament (LCL) and the biceps femoris tendon was retracted, which revealed that the proximal end of the LCL was ruptured. Through the incision, an inverted fragment with cartilage was observed, which was reduced and stabilized with the use of a 4.5-mm headless screw (Depuy Synthes, Warsaw, IN, USA).
The small fragment of the distal patella was removed and three suture anchors (4.5-mm HEALIX ADVANCE BR Anchor) were used to fix the ruptured patellar tendon to the distal patella. Since the medial side of the patellar tendon was severely damaged and there was an obvious deficit, the harvested ST was passed through the retinaculum to augment the medial side of the repaired patellar tendon. A suture anchor (6.5-mm HEALIX ADVANCE BR Anchor; Depuy Synthes) was inserted at the proximal attachment of the LCL. Then, the LCL was fixed by the placement of additional sutures. The initial EF device was changed to a ring-type EF device (Ilizarov external fixation; Keisei Medical Industrial Co., Ltd., Niigata, Japan) with a hinged joint and the center of knee rotation was defined at 2 cm proximal from the knee joint line. Thus, 2-mm K wires were inserted to connect the proximal and distal EF devices (Figure 6).

Intra- and postoperative images when applying a ring-type EF device.
Postoperative management following the first surgical procedure
Range of movement (ROM) exercises and half partial weight bearing (WB) were started 1 week following the first surgery, and full WB was allowed after 2 weeks. The ring-type EF device was removed at 7 weeks after surgery. At that time, the ROM was 0 degrees of knee extension and 20 degrees of knee flexion. The patient underwent ROM exercises and physical therapy wearing an elastic knee orthosis. ROM was 65 degrees of knee flexion and 0 degrees of knee extension at 7 months after surgery; thus, a second surgery was planned to improve joint mobilization.
The second surgical procedure (joint mobilization)
Arthroscopic (AS) joint mobilization was performed under general anesthesia. Release of the lateral para-patellar and supra-patellar pouch recesses, and the vastus medialis, as well as transverse resection of rectus femoris tendon, was performed. ROM following the second procedure recovered to 80 degrees of knee flexion and −5 degrees of knee extension. MCL reconstruction was not performed because of joint stiffness, and joint release was planned to be performed in advance.
The third surgical procedure (AS MCL reconstruction)
After conventional evaluation of the lateral para-patellar portal and a general intra-articular evaluation, AS synovectomy and joint mobilization were performed under general anesthesia. The ACL was loose and the white/white to red/white areas of both menisci were severely degenerated. In addition, there was a cartilaginous lesion in the intercondylar fossa (International Cartilage Repair Society grade III).
After these procedures, a 3-cm oblique skin incision was made along the medial proximal tibia of the contralateral limb to release the soft tissue. The ST and G tendons were harvested using a tendon stripper (Smith & Nephew Endoscopy, Huntingdon, UK). The diameter of the doubled tendons was 8 mm. Then, 3-cm longitudinal skin incisions were made at the ipsilateral femoral and tibial anatomical footprints of the MCL, and femoral and tibial bone tunnels were created at the anatomical footprint of the superficial fiber of the MCL. Then, the soft tissue between two incisions was peeled off to smoothly pass the graft through the soft tissue tunnel. 8
A 2.4-mm guide wire was inserted and a 4.5-mm ENDOBUTTON drill (Smith & Nephew Endoscopy) and 8-mm drill were used to create bone tunnels. A 20-mm socket was created at the femoral anatomical footprint. Then, the tendons were passed through an ENDOBUTTON CL (Smith & Nephew Endoscopy) and placed within the femoral bone tunnel.
The graft was passed through the femoral bone tunnel using a 2.7-mm passing pin (Smith & Nephew Endoscopy). Flipping of the ENDOBUTTON device was confirmed on fluoroscopy. Subsequently, the graft was passed beneath the soft tissue tunnel, proximally to distally, and the graft was passed through the tibial bone tunnel in the same fashion with the knee extended. The distal ends of the tendons were tethered using 2-0 Ticron sutures and attached to the ENDOBUTTON device (Smith & Nephew Endoscopy). After preparing the graft, the distal end of the graft was pulled with maximum manual force and the distal end of the graft was tethered to the tibial ENDOBUTTON device. The soft tissue was closed in layers and valgus instability became negative in both the extension and slightly flex positions (Figure 7).

Intra- and postoperative images of MCL reconstruction.
A knee brace was applied to keep the knee in extension following surgery.
Postoperative management following the third surgical procedure
ROM exercises and WB were allowed from postoperative day 1 and the degree of WB was dependent on the pain around the scar. At 2 weeks after surgery, ROM was 70 degrees of knee flexion and −5 degrees of knee extension with no complaint of valgus instability of the operated limb.
Clinical evaluation at the latest follow-up
At the last follow-up examination, ROM was recovered to 0 degrees of knee extension and 80 degrees of knee flexion, and extension lag was negative. The Lysholm score of the patient was 92. The patient had sufficiently recovered and returned to work in the construction field (Tegner activity scale score = 5) at 2 years after sustaining the injury (Figure 8).

Clinical images at the time of the latest follow-up examination.
Discussion
Knee dislocation caused by high-energy trauma is frequently encountered and requires multiple surgical reconstructions to obtain adequate knee stability. Reconstructive surgery, rather than surgical repair, is recommended shortly after such injuries to obtain optimal clinical outcomes.9–12 In addition, the incidence of the associated neurovascular complications is reportedly 29%, 13 since the popliteal artery is quite vulnerable. In case of concomitant popliteal artery injury, simultaneous artery repair is required at the time of reduction usually with an EF device applied both above and below the knee joint. On the other hand, there is currently a paucity of evidence concerning the treatment strategy for knee dislocations with open wounds that reach intra-articularly.
Even though there was no popliteal artery injury in this patient, definitive surgery was delayed because of Sunderland grade I peroneal nerve palsy until healing of the open wound across the patellar tendon was confirmed without evidence of infection. 15 With such injuries, the infection rate is high and surgical treatment is challenging, as more than 80% of patients report residual functional deficits. 14 At the first surgery, patellar tendon repair with augmentation using ST was performed because of a deficit of the medial patellar tendon. Reconstruction of the ACL and/or PCL was not performed during the first surgery because of knee joint contraction due to prolonged application of the EF device. 15 Therefore, only LCL repair was performed simultaneously. Knee joint contracture persisted after the removal of the EF devise; thus, MCL reconstruction was postponed and AS joint release had to be performed in advance.
The patient had no complaint of pain and was able to resume construction work, even though reconstruction of the ACL and PCL was not performed. Sisto and Warren 16 reported that early repair followed by cast bracing and manipulation for complete knee dislocation resulted in the return to vigorous activities in nearly 80% of patients. In addition, Lee et al. 17 demonstrated that the use of an external hinge, such as a Quengel hinge, to prevent posterior translation for patients with PCL injuries successfully resulted in a difference with the uninjured side of less than 3 mm, suggesting that the application of a hinged ring-type EF device might play a key role in early ROM restoration and to maintain the reduced position and acceptable recovery of the PCL injury without the need for reconstructive surgery, which might result in failure and/or complications in response to high-stress activities.18–20 With ACL and/or PCL injuries, there is certain risk of the development of osteoarthritis of the knee. However, there have already been reports of harvesting the bilateral hamstrings for the augmentation of the patellar tendon and MCL reconstruction. In addition, the ipsilateral central third of bone-patellar tendon-bone (BTB) was inappropriate as a graft source because of the post-trauma condition. Therefore, for patients complaining of knee weakness, the quadriceps tendon or contralateral BTB should be harvested as an autogenous graft source.
This report is the first to describe the safety and effectiveness of staged surgical management for the repair of open knee dislocation with concomitant MLI and PTR. However, further studies with longer follow-up periods will be needed to observe the development of osteoarthritis or weakness of the knee. Surgical irrigation, debridement, and the application of an articulated EF device followed by staged ligament and patellar tendon repair resulted in a favorable outcome for this patient with open knee dislocation and concomitant MLI and PTR.
Conclusion
Staged surgical management is a safe and effective procedure for repair of open knee dislocation with concomitant MLI and PTR.
Footnotes
Acknowledgements
T.T., K.I., and S.H. designed and wrote the article. T.M. participated in the surgery. All the authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.