
Abstract
Enchondromas are benign tumours that may become symptomatic due to expansive pressure on the surrounding bone. In this case, a 27-year-old male developed a symptomatic enchondroma within the proximal phalanx of his left fourth toe. Resection and insertion of a bone graft were considered optimal management. Histopathology testing confirmed the diagnosis of an isolated enchondroma. The patient was monitored closely for 3 months postoperatively and reported full satisfaction at his 12-month review. Enchondroma resection and insertion of a tibial bone graft may provide an effective long-term solution for a symptomatic enchondroma of the toe.
Introduction
Enchondromas are the second most common benign tumours of the bones of the foot after osteochondromas, 1 and are the most common tumours in the long bones of the hand. 2 They arise from cartilage cell nests that have fragmented from the central physis during development. 1 Enchondromas arise between the first and fourth decades of life and are usually found as incidental radiographic findings. 3 In some cases, they become symptomatic, requiring conservative or surgical management.
Radiographically, enchondromas present as well-defined lucent lesions within long bones.4–6 As they grow, the surrounding cortical bone thins, leading to bone stress and potential fracture. 2 Enchondromas are classified into five types with varying degrees of occurrence:2,7 central (58%), eccentric (19%), combined (21%), polycentric (11%) and giant (3%). A rare variant is enchondroma protuberans, involving a lesion that protrudes outward from the side of the affected bone and can mimic other osseous tumours.2,8
Microscopically, the structure of enchondromas is similar to normal cartilage, with comparable amounts of chondrocytes that are spread in hyaline matrix lacunae. 2 Their structure is nodular, due to the varying connective tissue septa and calcifications present. Phalangeal enchondromas often exhibit increased mitotic activity, yet their behaviour is benign.2,9,10 An important differential diagnosis is chondrosarcoma, a relatively rare malignant lesion.1,11,12
Herein, we present a case report of a symptomatic enchondroma within the proximal phalanx of the left fourth toe. Management involved resection of the lesion and replacement with an autogenous tibial bone graft. Success was defined as the resolution of symptoms and acceptance of the graft.
Case report
A 27-year-old male, interior designer, presented to our clinic reporting a 4-month history of chronic pain within his left fourth toe that had been resistant to conservative management. He described his pain as sharp and continuous, and he was no longer able to wear closed shoes nor participate in his weekly indoor soccer games.
His medical history included type I diabetes mellitus controlled with a NovoRapid Flexpen® (insulin aspart) 100 U/mL (1 U/10 g administered by an insulin pump). His most recent HbA1c was 6.5%. He also experienced clinical depression treated with Zoloft® (sertraline hydrochloride), 50 mg each morning. He reported no allergies or sensitivities.
Physical examination identified moderate oedema affecting the left fourth toe in toto. Tenderness was elicited with palpation of the whole length of this digit and to a lesser extent the metatarsal head. This digit remained in normal alignment.
Diagnostic ultrasonography showed a small amount of soft tissue oedema within the digit. No evidence of a ganglionic cyst, tenosynovitis or bursitis was seen. X-rays exhibited a lucent lesion within the proximal phalanx measuring 15 mm × 7 mm (Figure 1(a)). Magnetic resonance imaging (MRI) (Figure 1(b)) showed an expansile lesion breaching the inferior and lateral cortical bone. No soft tissue mass or definite stigmata suggestive of a chondrosarcoma was observed.

The X-ray (a) shows a well-defined lytic and expansile lesion measuring 15 mm × 7 mm of the left fourth proximal phalanx. The MRI (b) shows a moderate to hyperintensive lesion at the same location.
Surgical technique
The lower limbs were prepped and draped in typical fashion. After anaesthesia was achieved, a thigh tourniquet was inflated to 350 mmHg following the exsanguination of the leg. Local anaesthetic blocks of the left distal tibia and fourth digit were administered using a total of 29 mL, 0.75%, ropivacaine hydrochloride combined with 4 mg dexamethasone sodium phosphate, diluted with 10 mL sterile saline solution. The enchondroma was resected using a sagittal saw and rongeur forceps via a dorsal-linear incision (Figure 2(a) and (b)) and sent for histological examination.

The enchondroma before (a) and following (b) resection.
At the level of the tibia, a lineal incision was used (Figure 3(a)) and a cortical and cancellous bone graft was harvested from the distal metaphysis (Figure 3(b)). This was cut to size using a sagittal saw (Figure 3(c)) and inserted into the osseous gap left from the resection (Figure 4(a)). A 1.6-mm Kirschner wire was inserted through the bone graft material and intermediate and distal phalanges of the toe, then retrograded back into the metatarsal head. The transverse tenotomy of the extensor digitorum longus tendon was repaired using absorbable suture material. Both wounds underwent layered closure using 2-0 and 3-0 Vicryl (polyglactin 910) and 3-0 Monocryl (poliglecaprone 25) sutures (Figure 4(b)).

An autologous bone graft harvested from the distal tibia before (a), during (b), and after (c) resection.

The inserted autologous bone graft before (a) and after (b) closure.
Following the first dressing change at 7 days postoperatively, good anatomical alignment was demonstrated on his X-rays (Figure 5), no pain was reported and only minimal local oedema and bruising were observed.
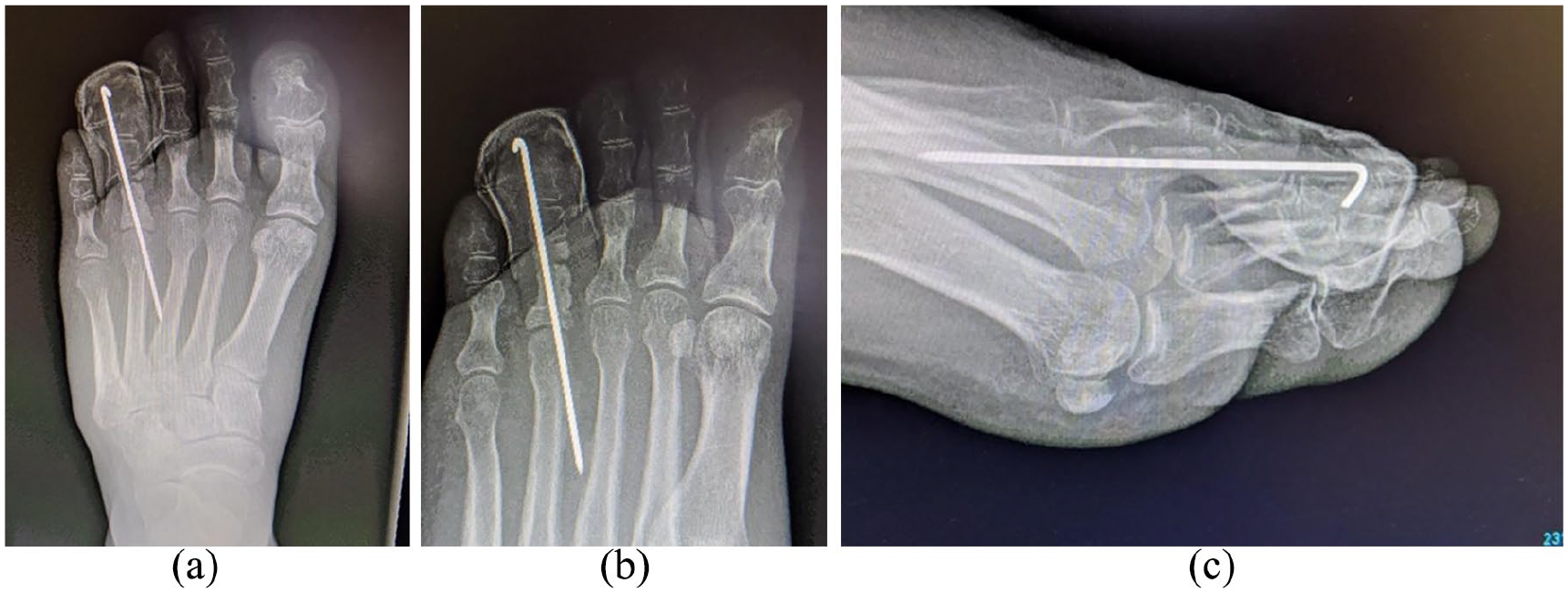
Postoperative anterior-posterior (a), medial oblique (b), and lateral (c) X-rays showing fixation of the graft with 1.6 mm percutaneous Kirschner wire.
Histology showed a well-circumscribed tumour composed of lobules of hyaline cartilage encased in bone and covered by fibrous tissue (Figure 6). No significant multi-nucleation, atypia or mitotic activity was exhibited, and no evidence of malignancy was identified. These findings were reported as in keeping with an isolated enchondroma.
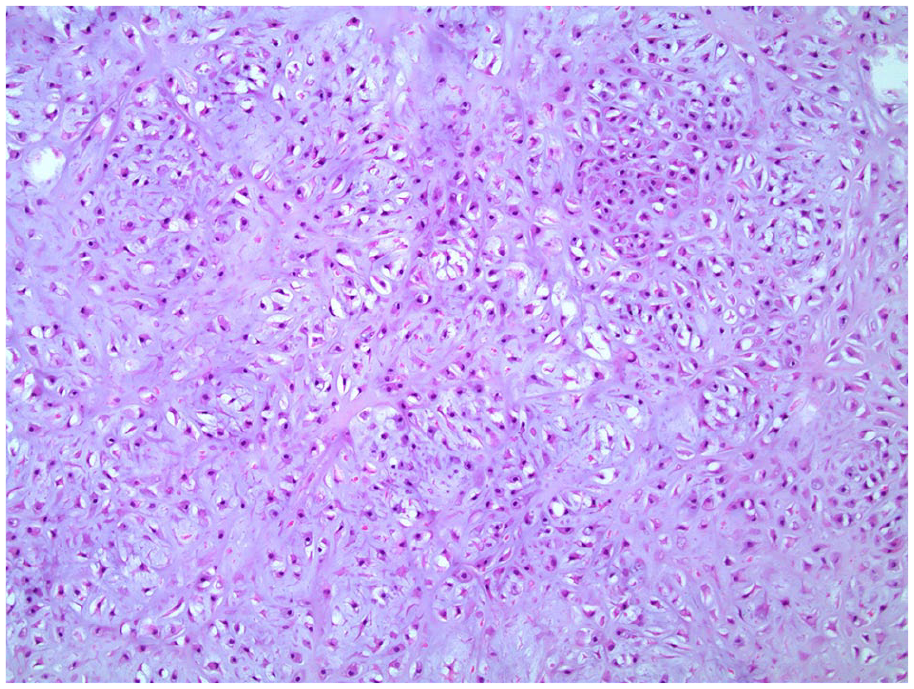
Enchondroma micrograph. The 15 mm × 10 mm × 10 mm cylindrical fragment was submitted for decalcification before processing and then processed as four transverse slices in two blocks. The section exhibited a well-circumscribed tumour composed of lobules of hyaline cartilage encased by bone and covered by fibrous tissue. There was no significant multi-nucleation, atypia, or mitotic activity. Focal haemorrhage and reactive vascularisation was seen within the lesion. No evidence of malignancy was identified.
At his 12-month review, the wounds had fully matured without scar tissue hypertrophy. No rubor, oedema, nor pain was exhibited or reported. He had returned to all activities, including his indoor soccer games, for over 6 months.
Discussion
Enchondromas account for about 10% of all benign osseous tumours 13 and are the second most common benign tumour of the foot after osteochondroma. They have a predilection for the small bones of the hand, with only 6% of enchondromas developing in the foot.5,9,14 They are typically found within the medullary cavity of the bone 12 with 80% of cases within the proximal phalanx. 1 Enchondromas occasionally present as multiple lesions, such as those that occur in multiple enchondromatosis (Ollier’s disease) and multiple enchondromatosis with associated haemangiomas (Maffucci syndrome). 13
The pain associated with enchondromas appears due to the increasing pressure of the expansion of the enchondroma on the surrounding bone, 13 the pathologic fracture of the surrounding bone, malignant conversion and the gradual enlargement of the digit. 15 Radiographically, they present as lytic lesions with well-defined borders and varying degrees of stippled or punctate calcifications 13 without the soft tissue involvement characteristic of chondrosarcomas. 1
This differentiation between enchondromas and chondrosarcomas is important. Mirra et al. 16 found that patients with chondrosarcoma were 12 years older than those with enchondroma and that 97% of patients with a chondrosarcoma reported pain, compared to only 44% with enchondromas. Radiographically, the margins of enchondromas are sharp and well-delineated compared to the indistinct expansive borders of chondrosarcomas. Murphey et al. 17 reported that deep endosteal scalloping, destruction of the cortices, soft tissue involvement and periosteal reactions suggest a chondrosarcoma. The malignant transformation of enchondromas into chondrosarcomas has been reported to be between 5% and 50%. 1
Most current knowledge regarding the management of enchondromas comes from hand literature. Tang et al. 18 reviewed the outcomes of surgical curettage, curettage without augmentation, curettage with augmentation by bone graft and curettage with augmentation by cement injection for the treatment of hand enchondromas. They did not recommend curettage due to the high rates of non-union (67%). A technique using cement injection into the cavity of the lesion did not appear to improve outcomes. They reported surgical augmentation with a bone graft as most appropriate, as it involved a similar recovery time to curettage, albeit with the inevitable additional wound that requires healing. 18 They recommended six monthly radiographic checks for small asymptomatic enchondromas and that questionable lesions be graded by the Enneking et al. 19 staging system and that biopsies be taken when there is a question of diagnosis. 18
Usually, chondrosarcoma and enchondroma are microscopically similar, with the presence of bi-nucleated chondrocytes required to diagnose a chondrosarcoma. 20 Also, enchondroma lobules are regular and their fibrous tissue consists of mature connective tissue, whereas chondrosarcoma consist of irregular lobules with cellular fibrous tissue encircling the tumour. 21 Histopathological analysis of our specimen showed minimal protuberance with well-circumscribed lobules of hyaline cartilage encased by bone and covered with fibrous tissue.
Multi-modal treatment methods were implemented in our case. These included careful surgical technique and preparation of wound edges, even wound approximation with minimal tension, careful resection and insertion of the autograft fragment, and postoperative antibiotics with antiseptic dressings to reduce the risk of infection. Early compression therapy 22 was employed. He was allowed to weight-bear immediately but remained in his postoperative shoe until 1 week after the wire was removed at his 3-month review.
Conclusion
We present a case of a symptomatic enchondroma and its surgical management. The tumour was confirmed as an enchondroma based on radiographic and histopathologic results. Close postoperative monitoring was implemented. The patient reported the complete resolution of his symptoms at 6 months that continued until his final review at 12 months postoperatively. Enchondromas are generally asymptomatic incidental radiographic findings, yet can be symptomatic when there is stress and fracture of the surrounding cortical bone. Resection of the enchondroma and insertion of an autogenous bone graft can provide excellent and reliable long-term outcomes.
Footnotes
Acknowledgements
The authors thank Dr Ali Moghimi for reporting the histopathology results.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.