
Abstract
Ipsilateral hip and knee dislocation is a rare and complex injury that usually results from high-energy trauma. Only 14 cases were reported in the literature so far. We report the case of a 35-year-old man who presented with an ipsilateral right hip and knee dislocation after being involved in a road traffic accident. A contralateral floating knee was associated. The hip dislocation was associated to a posterior wall fracture of the acetabulum and a femoral head fracture. The knee dislocation was compound and associated with a patella fracture. The hip dislocation was reduced. The posterior wall and the femoral head fractures were treated conservatively. The knee dislocation was reduced and stabilized by external fixator. Early postoperative infection occurred and was treated surgically. At the last follow-up, the knee was ankylosed at 5° of flexion with a bony bridge between the femoral condyle and the tibial plateau. The patient described an occasional hip pain on exertion. He had full range of motion of the right hip. No avascular necrosis of the femoral head was seen. Outcomes of simultaneous hip and knee dislocation are very variable and remain unpredictable. The timing of reducing the hip joint and the knee.
Introduction
Hip and knee dislocations are orthopedic emergencies. In isolation, these injuries are of common occurrence in routine trauma practice. However, simultaneous ipsilateral dislocation of both joints is an unusual injury denoting the severity of the trauma.1,2
This injury pattern usually occurs following a high-energy trauma and is often associated with concomitant lesions and secondary complications. Simultaneous ipsilateral hip and knee dislocations not only require urgent treatment but also pose a real challenge for orthopedic surgeons. Decisions need to be taken regarding the appropriate therapeutic strategy to follow in order to achieve proper reduction and stabilization of the dislocations and to prevent any iatrogenic injury that may be caused by the reduction attempts.
We report the case of a patient with concomitant ipsilateral hip and knee dislocations and discuss the literature.
Case presentation
A 35-year-old man, with no personal or family medical or surgical history, was a victim of a high energy motor vehicle accident (head-on collision). The patient was brought to the emergency room with the main complaint of painful and deformed lower limbs.
After applying the Advanced Trauma Life Support principles, 3 vital emergencies were ruled out and isolated injuries to the lower limbs were retained.
On clinical examination, the patient was perfectly conscious and his vital parameters were stable.
The musculoskeletal examination of the right lower limb revealed a 7-cm wound over the anterior aspect of the right knee which was grossly deformed. The distal femur was protruding through the wound and a fracture of the patella was visible (Figure 1(a)). The right hip was flexed, adducted and internally rotated. The dorsalis pedis and tibialis posterior pulses were palpable. Dorsiflexion of the left ankle and sensation along the lateral aspect of the leg and the dorsum of the foot were absent suggesting an injury to the common peroneal nerve.
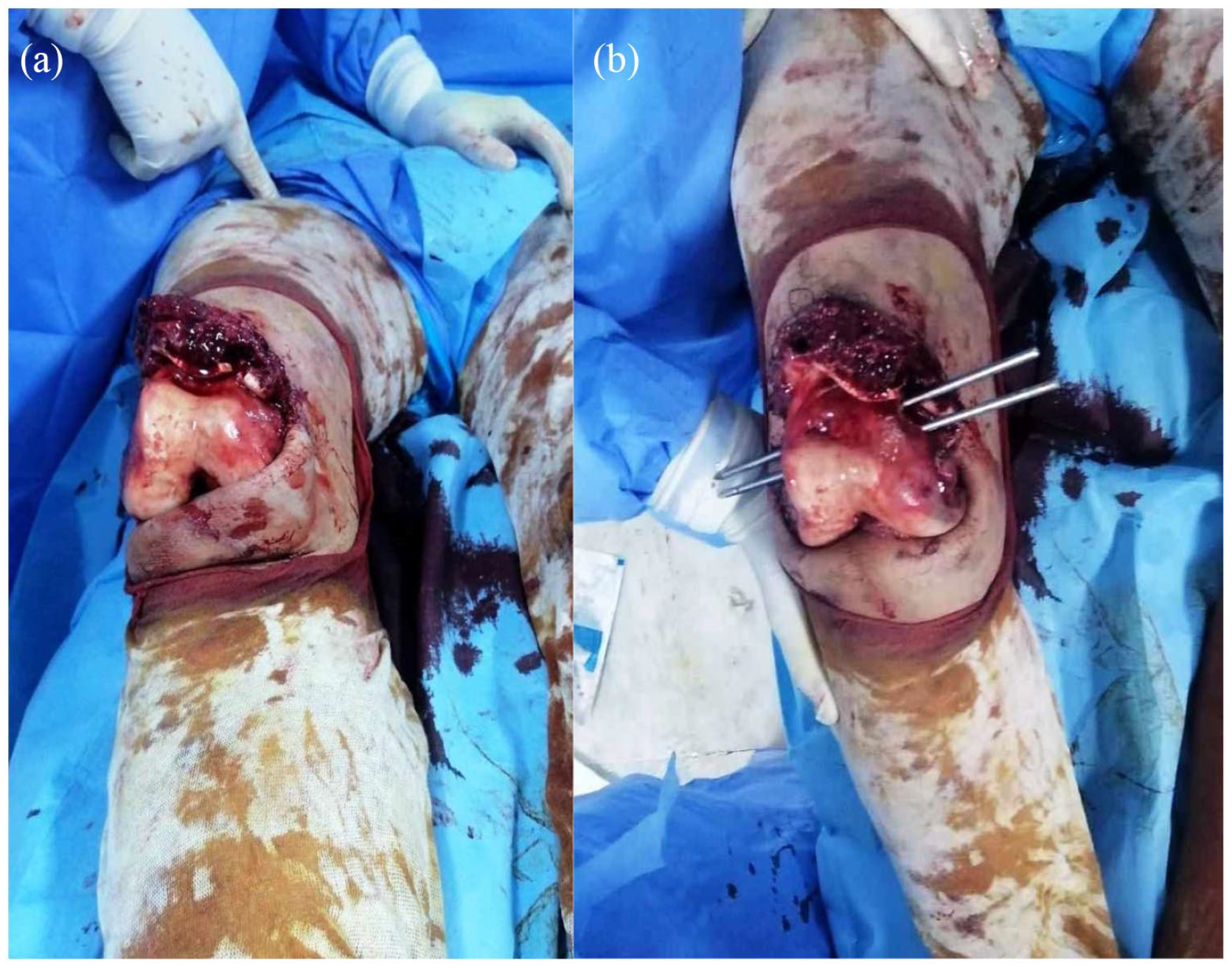
Open posterior dislocation of the right knee with protruding femoral condyle through the wound (a). The reduction of dislocated hip was done using two trans-fixating Steinman pins inserted in the distal femur (b).
On examination of the left lower limb, the left thigh and leg were also deformed. The skin was intact and there was no associated neuro-vascular deficit.
Radiological assessment showed a simultaneous posterior right hip fracture–dislocation and a posterior dislocation of the right knee associated with a comminuted fracture of the patella. On the left side (Figure 2), displaced mid-shaft femur and tibia fractures were noted realizing the so-called floating knee.

Standard X-ray showing a right hip dislocation (a) and an ipsilateral knee dislocation with a patella fracture (b).
The patient was immediately taken to the operating room. In theatre, the patient’s hemodynamics deteriorated and was classified as “Borderline” and the decision of damage control surgery was taken.
The surgical procedures were done by two teams led by a senior orthopedic surgeon each. Under general anesthesia, on an ordinary table, the patient was put supine and a sterile draping of both lower limbs was done.
On the right side, the first step consisted in a closed reduction of the hip fracture–dislocation. To do so, two trans-fixiating Steinman pins were inserted into the femoral condyles (Figure 1(b)). The pelvis was stabilized by the assistant and traction associated to flexion and internal rotation was applied in the direction of the femur using the pins. An audible “clunck” was heard as the hip reduced. Skeletal traction was not performed as the hip felt stable after reduction.
The wound over the anterior aspect of the knee was then debrided. The joint was thoroughly washed and inspected. Joint exploration found a complete tear of the anterior and posterior ligaments. The dislocation of the knee was reduced and stabilized with an external fixator (Orthofix®). The patella was fixed by tension band wiring. In the meantime, a stabilization of the left “floating knee” was achieved by the second team using external fixation devices (Orthofix®) applied to the femur and the tibia under fluoroscopic control.
The patient was then taken to intensive care for further resuscitation.
Analgesia, prophylactic anti-coagulation, and intra-venous antibiotics were prescribed.
Postoperatively, X-rays showed a good reduction of the left hip and knee. Pelvis CT scan showed a congruent hip joint with a minimally displaced posterior wall fracture and a Pipkin type I undisplaced femoral head fracture (Figure 3).
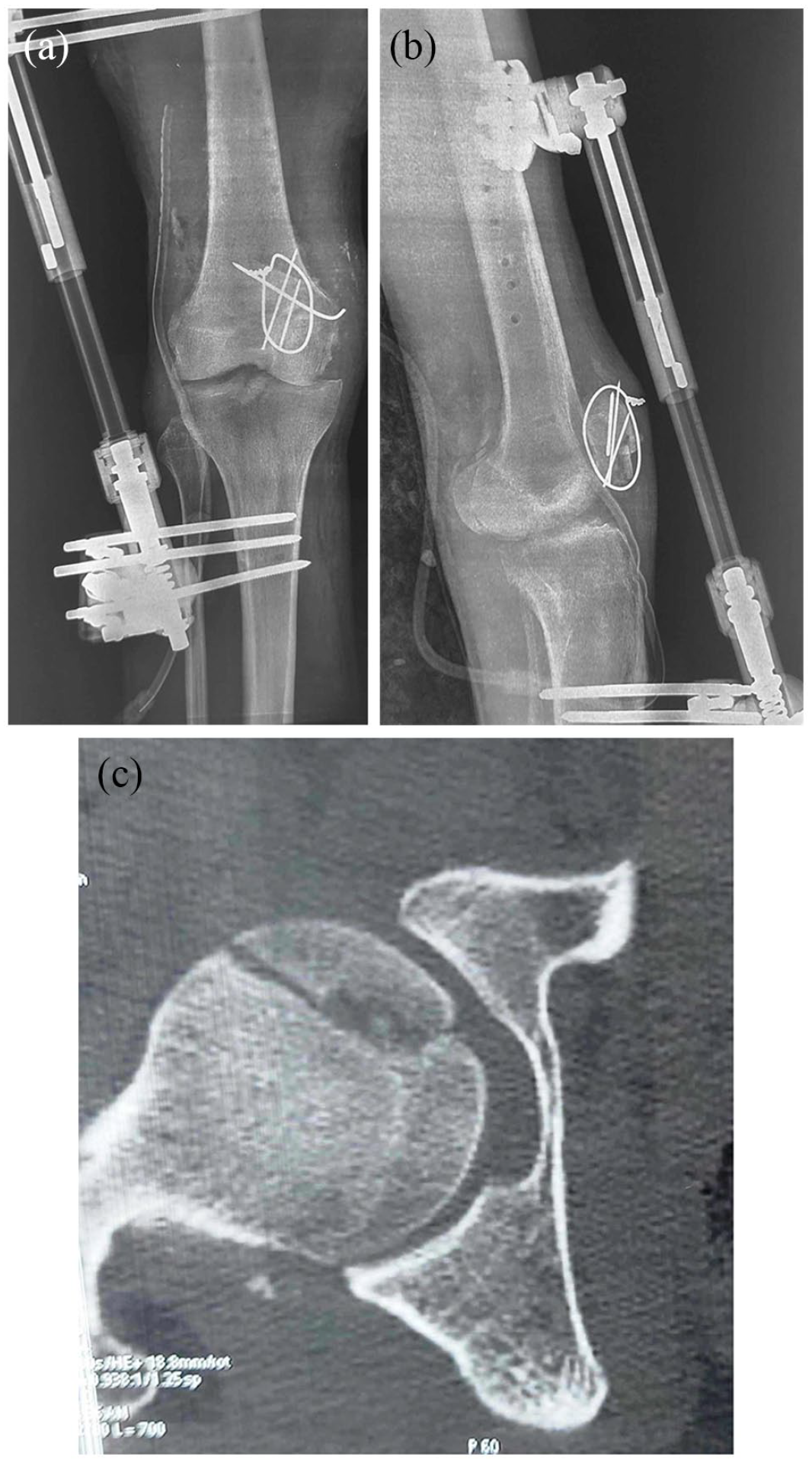
Postoperative X-ray of the knee (a and b) showing an acceptable reduction of the knee dislocation. CT scan of the hip (c) showing a congruent hip joint with undisplaced femoral head fracture.
The patient was stabilized. However, he had to be taken to theatre on day three for an early sepsis in the right knee requiring a second-look surgery with irrigation and drainage of the knee. The joint infection could be controlled after several surgical debridement and prolonged antibiotics.
MRI of the knee was discussed to identify the other ligament injuries. However, the presence the metallic hardware as well as the recurrent infection prevented us from any further exploration.
Across knee fixator was removed at 13 weeks postoperatively.
At 18 month follow-up, the right knee was stiff at a fixed 5° flexion contracture (Figure 4). There were no signs of active infection. Standard X-ray showed an ankylosis of the knee joint, this can be explained by the chondral lesions due both to the initial trauma and the recurrent infection. The right hip, however, was fully mobile with occasional pain and no signs of avascular necrosis (AVN) (Figure 5). There was a slight recovery of his neurologic fallout, the patient refusing any further surgery.

Clinical results at the last follow-up.

Standard X-ray of the knee at the last follow-up (a and b): a bone bridge joining the medial femoral and tibial condyle. No avascular necrosis of the femoral head was seen on the X-ray of the pelvis (c).
The left side fractures went on to consolidation with the external fixators with some residual knee stiffness that improved with rehabilitation.
Discussion
Ninety percent of hip dislocations are posterior. The most common causes are either a fall from a height or an axial force loaded on the flexed hip (dashboard mechanism). 4 Furthermore, hip dislocations are often associated with knee injuries, secondary to either direct or indirect trauma. 5 For this reason, in posterior hip dislocations, a rule of thumb is to always proceed with a thorough physical examination of the knee to identify any associated ligamentous injuries.
Simultaneous ipsilateral hip and knee dislocation is an extremely rare injury. It usually is related to high energy trauma.
To the best of our knowledge, only 14 cases of this entity have been reported in the English literature. A summary of the published cases can be found in Table 1.1,2,6–17
Reported cases of ipsilateral hip and knee dislocation.

P: posterior; PW: posterior wall; FH: femoral head; FN: femoral neck; (C): vascular injury; CR: closed reduction; OR: open reduction; #: fracture; LFC: lateral femoral condyle.
Eight of the 14 reported patients,1,6,8,14–17 including the present case, had associated injuries. Some of these injuries can be serious such as chest trauma, ipsilateral femoral shaft fracture, or contralateral floating knee as our case. This confirms that the mechanism is usually violent and often secondary to high velocity accidents. For this reason, a full clinical and radiological examination must be carried out to rule out any life-threatening emergencies.
Ipsilateral hip and knee dislocation may be associated with serious acute complications. Three of the 14 patients (21.5%) had popliteal artery injury.1,11,16 Arterial repair was successful only in one case 16 ; however, the remaining two patients ended up with limb amputations.1,11 Four patients including our case had common peroneal nerve fallout.2,7,12 Three patients ultimately recovered, but in our case recovery was only partial. Cornwall and Radomisli 18 reported a 10% incidence of nerve complication following traumatic hip dislocation. Generally, exploration of the nerve was not recommended when this complication was associated with traumatic hip dislocation. Traumatic knee dislocations, on the other hand, were associated with nerve injury in up to 40% of the cases. 19 The management of this neurological fallout was controversial. However, most of the authors recommend a common peroneal nerve neurolysis when posterolateral corner repair or reconstruction was done.
Simultaneous hip and knee dislocation represents an extremely uncommon injury pattern, with a high risk of neurovascular compromise. For this reason, all the cases including ours were considered as therapeutic emergencies. The management should be done as soon as possible after the injury.
Several reduction techniques for the hip dislocation were described in the literature. Closed reduction was done by most of the authors. Freedman et al. 9 reduced the hip with manual traction over the thigh. Dubois et al. 12 described the use of Schanz pins inserted in the femoral condyle as well as lateral aspect of the proximal femur to affect the reduction. Our technique was similar with the use of two Steinman pins placed in the distal femoral condyle. Waterman et al. 16 described a technique where the traction force was applied on the flexed knee through the distal femur. We think that the use of pins inserted through the distal femur is safer than pulling over an instable knee to prevent possible iatrogenic vascular complications.
Open reduction was indicated when closed reduction was unsuccessful.7,8 Once the hip is reduced, the knee dislocation can be reduced in the same way as isolated dislocations.
Knee dislocations associate a various multi-ligamentous injuries. The best treatment remains surgical. Many studies discuss the advantages and drawbacks of early or delayed reconstruction of the involved structures in order to reach better clinical outcomes. 2
In patient with knee dislocation, Ma et al. 20 found better functional and clinical outcomes when a two-stage strategy is adopted consisting in peripheral structures reconstruction in phase I followed by anterior and posterior cruciate ligaments reconstruction in phase II. Most of authors believe that lateral collateral ligament integrity is paramount for the stability of the knee joint. Early repair involving a simple suture of the broken ends should be performed, and it is preferable to delayed complex reconstruction. 21 In our case, the septic complication prevented any further ligamentous reconstruction of the affected knee until the last follow-up.
Function and clinical outcomes of hip and knee dislocations can vary widely from restitutio ad-integrum of the limb function to through or above the knee amputations. Several factors can affect the functional outcomes such as the timing of hip reduction, the presence of neurovascular complications, and the management of multi-ligament knee injury.1,2,13 In our case, the patient had good functional and clinical results for the hip; however, infection was deleterious for the final result of the open knee dislocation.
Conclusion
Ipsilateral hip and knee dislocation is a serious and rare emergency. Proper management is necessary for good functional outcomes. The timing of hip joint reduction and knee ligament reconstruction are the most important prognostic factors. The outcomes are very variable and remain unpredictable.
Footnotes
Acknowledgements
The authors would like to thank Ms Slim Jerbi and Ms Mohamed Gannar for their kind assistance in the elaboration of this article.
Author contributions
All the authors participated in the design, performance, analysis and drafting of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.