
Abstract
Background:
Informed consent, grounded in the ethical principle of autonomy, represents a patient’s agreement to undergo a procedure. Given its critical role in protecting human rights and autonomy, obtaining informed consent before any surgery or procedure is now a mandatory practice. However, many studies question whether informed consent is conducted genuinely, ensuring proper understanding of the information disclosed, or merely serves as a medicolegal formality. This has led to increased malpractice, misunderstanding, anxiety, and overall postoperative dissatisfaction.
Objective:
This study aimed to explore patients’ perceptions and experiences regarding the informed consent process for elective surgeries, identifying key challenges and areas for improvement.
Methods:
This descriptive qualitative study was conducted at Aga Khan Hospital using individual in-depth interviews. Fourteen patients who had undergone elective surgery were recruited. Baseline data were presented in tables, and inductive thematic analysis was used to interpret the qualitative data.
Results:
Seven themes emerged from the data: Consent as a legal formality, autonomy, and decision-making, insufficient information, time constraints and lack of opportunities for questions, use of medical jargon, patients’ desired information, and overall satisfaction with care. Despite patients’ higher levels of education and the hospital’s patient-centered care approach, many felt the information provided was insufficient, superficial, and difficult to understand.
Conclusion:
The study found a significant gap between the information patients desired and what was provided. Insufficient information, coupled with the use of medical jargon and time constraints, adversely affected the informed consent process. Enhancing clarity in communication and allowing adequate time for discussions could improve patient understanding and satisfaction.
Keywords
Introduction
Patient-centered care is a fundamental aspect of modern medical practice, underscoring the importance of involving patients in decisions about their own health. This approach is deeply rooted in the ethical principle of autonomy, which asserts that individuals have the right to make informed choices about their medical treatments. 1 Informed consent is a critical mechanism designed to uphold this autonomy by ensuring that patients are fully informed about the nature of their medical procedures, including the potential risks, benefits, and available alternatives, before giving their consent. 2
Informed consent is meant to be a thorough and transparent process that enables patients to make decisions aligned with their personal values and preferences. 3 It involves several key components: disclosure, where all relevant information about the procedure is provided; capacity, which refers to the patient’s ability to understand the provided information; voluntariness, ensuring that the patient’s decision is made without coercion; competence, indicating the patient’s legal and cognitive ability to make the decision; and decision, the patient’s explicit consent to proceed with or decline the intervention. Together, these elements are intended to protect the patient’s autonomy and promote their right to make informed choices. 4
Despite the theoretical importance of informed consent, in practice, the process often falls short of its intended goals. In many healthcare settings, particularly in busy environments or resource-limited contexts, the informed consent process can become a formality rather than a meaningful dialogue. 5 Patients may sign consent forms without a comprehensive understanding of the procedure or its implications. This issue is compounded by various factors, including time constraints faced by healthcare providers, varying levels of patient education, and cultural differences that can influence communication and understanding. 6
In developing countries, including Tanzania, additional challenges further complicate the informed consent process. These challenges include limited healthcare resources, high patient volumes, and diverse cultural practices that can affect how information is communicated and received. Research from other developing countries, such as India, Nigeria, and Pakistan, has shown that patients often view informed consent primarily as a legal obligation rather than a genuine process of protecting their autonomy.7–10 These studies highlight a widespread issue of insufficient understanding among patients about the informed consent process, suggesting that improvements in communication and education are needed.
In Dar es Salaam, Tanzania, there is a notable lack of research specifically addressing patients’ perceptions and understanding of informed consent. Existing studies primarily focus on Western populations, which may not accurately reflect the unique challenges faced in Tanzanian healthcare settings. Given the cultural, educational, and systemic differences, it is crucial to conduct localized research to better understand how patients in this context perceive and engage with the informed consent process.
This study aims to bridge this gap by exploring patients’ perceptions and understanding of preoperative informed consent at Aga Khan Hospital in Dar es Salaam. By assessing patients’ comprehension of the information provided during the consent process, identifying factors that influence their decision-making, and determining their preferences for the information shared, this research seeks to enhance the effectiveness of informed consent practices. The findings will contribute to improving patient care, reducing misunderstandings, and ensuring that the informed consent process better aligns with patients’ needs and expectations in the local context.
Materials and methods
This study utilized a hospital-based descriptive qualitative design, employing semi-structured individual interviews to explore patients’ perceptions and understanding of the preoperative informed consent process at Aga Khan Hospital, Dar es Salaam, Tanzania. The design was chosen to deeply investigate patients’ subjective experiences and views on how informed consent was communicated and perceived. The research, conducted between 2nd February and 6th May 2022, focused on understanding these perspectives without imposing the researchers’ assumptions and biases.
The study was conducted at Aga Khan Hospital, a Joint Commission International Accreditation (JCIA)-accredited tertiary and teaching facility located on Barack Obama/Ufukoni Road in Dar es Salaam, Tanzania. The hospital, known for its surgical specialties in General Surgery and Obstetrics and Gynecology, performs over 1500 surgeries annually, including same-day, emergency, and elective procedures. The informed consent process at the hospital involves two components: anesthesia consent and procedure consent, each requiring separate forms and typically handled by different members of the medical team.
The study targeted postoperative patients who had undergone elective surgical procedures in the departments of Surgery and Obstetrics and Gynecology. Inclusion criteria were patients aged 18 years and older, who were fit for discharge after an elective operation and consented to participate. Exclusion criteria included patients who could not speak English or Swahili and those with mental illness.
Our sample size was determined based on the principle of data saturation, which is commonly used in qualitative research to identify the point at which no new themes or insights emerge from additional data collection. We continued conducting interviews with participants until we observed a consistent repetition of themes, and no novel information was identified in subsequent interviews. The decision to conclude data collection after 14 participants was based on the analysis of the data during the interview process, which indicated that no further significant themes were emerging, and redundancy in responses became evident.
This approach is in line with qualitative research standards, where saturation is a key criterion for determining an adequate sample size rather than relying on statistical calculations. Our study’s sample of 14 participants was deemed sufficient, as it aligns with the sample sizes used in similar studies on informed consent, where saturation was achieved with comparable or smaller numbers of participants.
To minimize bias and enhance the credibility of the findings, we employed purposive sampling to ensure diversity in the participants, including individuals with varying levels of education, socioeconomic backgrounds, and experiences with elective surgeries. Participants were recruited voluntarily, and data triangulation was employed by using multiple data sources (i.e., in-depth interviews) to validate and cross-check the findings.
While qualitative studies do not require statistical sample size calculations, our approach ensures that the findings are transferable to similar settings, thereby offering valuable insights that may be relevant to other healthcare institutions with comparable patient populations.
Participants who consented were invited for individual interviews with the principal investigator, with demographic and background information collected using a data checklist. A semi-structured interview guide was used, developed based on the existing consent forms, and allowed for dynamic adjustments throughout the study. Topics covered included familiarity with informed consent, communication of procedure information, risks and benefits, alternatives, and overall satisfaction with the consent process.
Data collection involved interviews conducted by the principal investigator and a trained research assistant. Interviews were held in patient rooms or a private conference room to minimize interruptions, with each interview lasting 15–30 min. Recordings were made using a Samsung Tab S4 tablet and backed up on an external hard drive. Interviews were conducted in English or Kiswahili based on patient preference. After each interview, participants could ask questions or provide feedback about the study and consent process.
Data were stored on a password-protected tablet and backed up on secure devices. Interviews were transcribed verbatim, with Kiswahili transcriptions translated into English and verified for accuracy. Thematic analysis was employed to analyze the data, following steps of immersion, transcription, code generation, theme development, and refinement. The principal investigator performed the coding independently, with triangulation used to ensure consistency and minimize bias. Final results were presented in a descriptive summary, supported by verbatim quotations to illustrate key themes.
Consent for publication
Written consent for the publication of the research findings has been obtained from all participants included in this study. Participants were informed about the purpose of the study, the nature of the data that would be collected, and the potential implications of publication. Confidentiality has been maintained, and any identifying information has been appropriately anonymized to protect the privacy of the participants.
Results
The participants’ ages ranged from 27 to 69 years, 8 were females, and 6 were males; all participants had a university education, and the majority were employed. A small number of the participants came from other regions outside of Dar es Salaam. It was noted that those from rural had traveled to seek better care as they had been operated on previously in their local hospitals without getting improvement. This is summarized in Table 1 below.
Participants’ demographics.
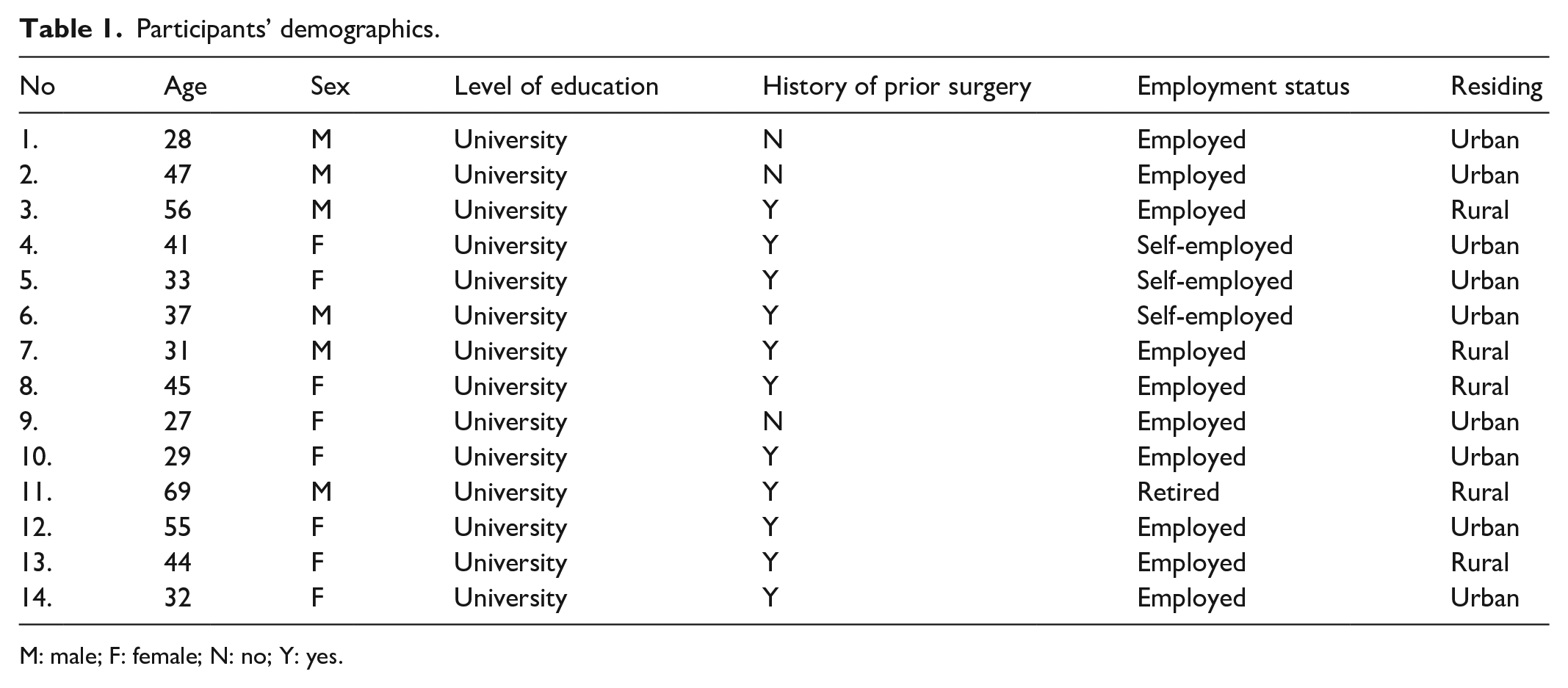
M: male; F: female; N: no; Y: yes.
Themes and subthemes
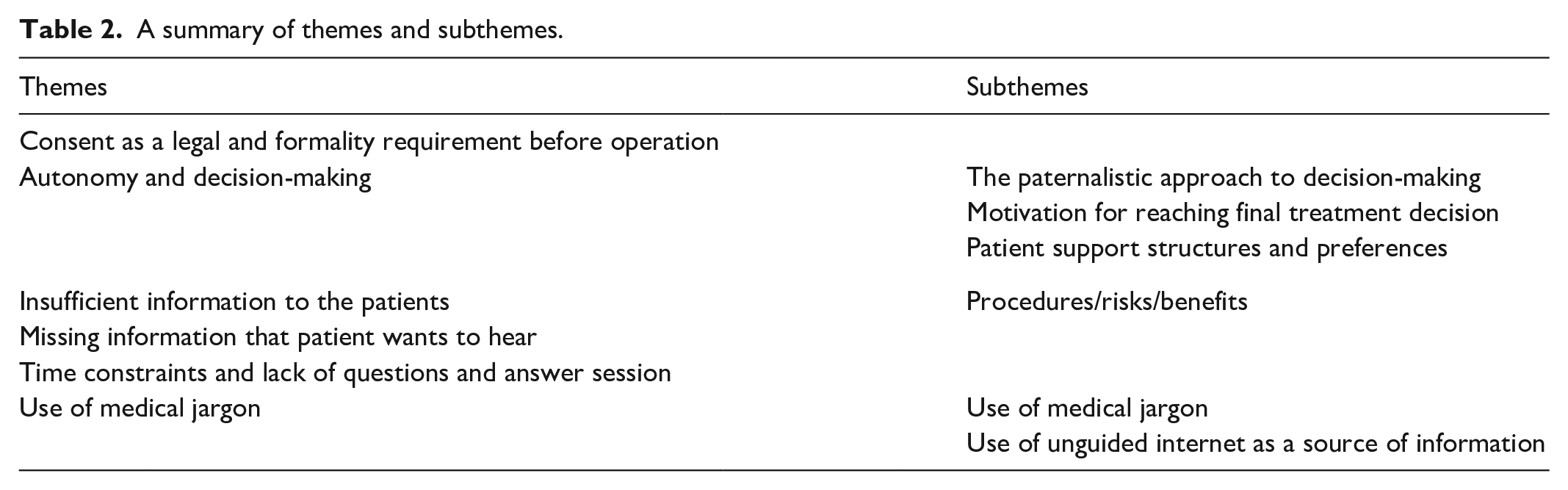
Analysis of the responses from the interviewed participants revealed seven themes. These themes and their corresponding subthemes are summarized in Table 2 below:
A summary of themes and subthemes.
Consent as a legal and formality requirement before operation
Most patients interviewed were aware of the need to consent and complete consent forms before undergoing surgery, particularly those who had undergone previous operations. However, there were varied perceptions regarding the informed consent and the consenting process. Some patients saw informed consent as a necessary step for receiving care, feeling compelled to grant permission to proceed with the planned treatment. As one participant stated, “Well, to be honest, I felt like it was a must process that I had to go through before the surgery. . .participant 2” Another noted, “By consenting means, I am agreeing to what’s going to happen and any outcomes that may come. Like in a way, it reduces your accountability. . . participant 4” A third participant expressed, “Maybe if I had signed the form while I was with my doctor talking, maybe the form would have felt like more of a consent, but it just felt like a formality, just a legal document that you just need to sign-off and proceed. . . participant 10”
Conversely, some patients recognized the importance of understanding the information and risks associated with the treatment before giving consent. One participant described it as, “This is the process which shows that someone has agreed to receive treatment that he/she has understood the procedure, the risks associated. . . participant 7” Another elaborated, “Well, informed consent is an agreement that a doctor shares with you, which elaborates the treatment that is going to he or she is going to, doing and what I should expect the risk factors that I should expect, and where we could reach an agreement, where I would say that I give my consent, with a full understanding of what is going to happen. . . participant 14”
There were also participants who were unaware of the informed consent process prior to their admission, discovering it only after being admitted to the hospital. One participant said, “I have never heard of it before; this is the first time. . . participant 1” Another added, “I have never heard it before, but from the word itself, I can try to explain. It is a process whereby one grants permission for a certain treatment to be done on him. participant 8”
Some patients viewed informed consent as a means of protecting both the patient and the doctor from legal issues if complications arose. One participant remarked, “Consent is very important because it ensures safety for both the patient and the doctor just-in-case of any complication intra-op or post-operatively both parties are accountable to their decisions. It helps to prevent and reduce misunderstanding between patients and health personnel. participant 3.” Another noted, “Signature in consent is all about making sure no harm comes to the doctor. Whatever happens during surgery, it is the patient who suffers. participant 11”
Autonomy and decision-making
Paternalist approach to decision-making and reverence to the doctor
Although autonomy is central to patient decision-making, some participants felt that the doctor should make the final decision regarding their treatment. As one participant stated, “The doctor is the final decision maker because it is their area of expertise, so they will always choose the best solution for my problem. participant 5.” Another noted, “It depends on the situation. There are situations where one is not aware of or has a clue; it’s important to give the doctors the chance to decide for us based on their qualifications. participant 7”
Patients also felt that the limited information provided by doctors left them without alternatives to consider. For instance, one participant mentioned, “Well, like with me, if I did have a second thought at that point, I probably would have just gone ahead and told the doctor. If I really want to, no one could actually keep me here against my will, aahm, if I were adamant that no I have changed my mind, I would leave, then obviously you don’t have the power to force me to have the operation. . . participant 13.” Another participant shared, “Yes, I had a second thought. I remember I refused the surgery initially, and the doctor brought the form leave against medical advice forms (LAMA) to sign that I have refused surgery, which I did sign; but after critically thinking about the situation and condition of my unborn baby. I decided to accept the surgery. . . participant 11.” Conversely, one participant felt that changing their mind could be disruptive, stating, “Changing mind after signing the form is like disturbance both to the doctor and the patient him/herself. A doctor cannot force a patient, so it’s a loss to the patient because the problem will not be solved on time. . . participant 4”
Motivation for reaching final treatment decision
Patients often base their final decision on various factors, including support from the primary doctor, delays in healing, and fear of complications. One participant said, “I accepted because the wound didn’t look so well, and what I wanted was to be treated and get done with this. . . participant 12.” Another stated, “This is my life, so if I refuse the surgery, I will end up with another problem, so it is better to proceed with the operation as to how the doctor proposed, so as to get rid of the problem for good. . . participant 9.” Some participants indicated that their decision was driven by the urgency to find a solution rather than the information provided. One explained, “No, not really; my decision to have the surgery done was mainly because of the condition I had and not the information provided. I wanted an immediate solution. . . participant 10”
Patient support structures and preferences in making their decision
Patients expressed varying preferences regarding who should be present during the information-giving process. Some preferred to receive information alone and decide if and with whom to share it, as one participant mentioned, “My own opinion is that I would like to receive the necessary information regarding my operation alone, and if I feel or need to share, then I can decide who to share with. . . participant 1.” Others valued having family members present for support and to assist with understanding and postoperative care. One participant noted, “Yes! I would love my wife to be there because she is the one who will be there during my recovery. To know which kind of food I am supposed to eat because she is the cook. participant 9.” Another shared, “It is better if a family member is present when the doctor gives details about the surgery because, as a patient, I am already distressed. At that moment, I might not comprehend what’s being told by the doctor. participant 12”
Insufficient information to the patients
Inadequate information provision, including lack of information on diagnosis, risks, benefits, and alternatives
Many patients felt they received insufficient information about their operation. Some did not understand their diagnosis or the details of their procedure, as illustrated by one participant who said, “The doctor just told me about his decision; he has never explained what my disease is neither the operation that I underwent. Up to this moment, I don’t know what they have done to me; no one has told me anything apart from their daily plan of giving me medicine, antibiotics, and not to eat. I am looking forward to finding out when I come back to my clinic visit. I hope the doctor will tell me everything. . . participant 14.” Another participant expressed dissatisfaction with the superficial explanation provided, stating, “Nah! They didn’t explain much, and of course, the explanation was superficial; they only asked the few things on the form.”
Patients also reported a lack of information about postoperative care and recovery. One participant mentioned, “Yeah! So I don’t think I am leaving with questions about the surgery, maybe just about the aftercare like when will I resume work, start my normal routines and other things which I am not aware of. participant 5” Another added, “Mostly about the surgery itself and if life changes after the surgery in terms of, you know I am an exercise person, so I would have appreciated the information on how this might be affected by the surgery. participant 6”
Missing information that the patients want to hear
Patients identified several key areas they felt were often neglected during the informed consent process. They wanted more detailed information on risks, complications, aftercare, and the recovery process. One participant suggested, “Eeh, maybe there is need to sit with the patient, ask about their understanding, provide information regarding the operation, how it will be, how long it will take, how the recovery process will be like, any side effects during and after the operations, after the operation what will happen, if you experience something whether it will be normal or needs to seek care. Things like these need to be discussed. participant 8.” Another participant wished for more detailed explanations, saying, “Well, as you can imagine, there are things that everyone has, going through their mind, being body insecurities and stuff. And I really wish I could get more information on what I would expect after the surgery, the impact of this scar. Is there something that could have been done differently, a better surgery than this that could leave me a bit more scarless? Is there an alternative where I wouldn’t have to do open surgery that would just be the medical treatment? I wish I could also know how that impacts my daily routine and how it would affect with exercising, sex, eating and going to work and not just facing them as a surprise after. . . participant 11”
Use of medical jargon
Use of medical jargon during explanation
The use of medical jargon during the informed consent process created a significant barrier to patient comprehension, as highlighted by participants’ responses. The complexity of technical terms often made it difficult for patients to fully grasp the nature of their procedures, leading to frustration and a sense of exclusion from the decision-making process.
One participant expressed their struggle, stating, “What I needed, a little bit more information, explanation of the words, the medical terms that I couldn’t understand. . .” (Participant 1). This statement underscores the fact that patients desire more than just procedural consent; they seek a deeper understanding of the information provided. However, the presence of unfamiliar medical terminology hindered their ability to do so.
Similarly, another participant voiced their frustration, saying, “Sometimes I wanted to shout to the doctor, ‘please speak a normal language’ because our conversation was so strange.” (Participant 10). This quote illustrates not only the communication gap but also the emotional toll it took on the patient. The use of complex terminology created a disconnect between the patient and the healthcare provider, making the interaction feel alienating rather than informative.
The implications of this issue are far-reaching. When patients struggle to comprehend medical explanations, they may feel uncertain, anxious, or even coerced into making decisions without fully understanding the risks and benefits. This can impact their trust in the healthcare system and reduce their overall satisfaction with care. In some cases, patients may resort to alternative sources of information, such as the internet or nonmedical advisors, which may further contribute to misinformation or misinterpretation.
To address this issue, healthcare providers should prioritize clear and patient-friendly communication. Simplifying language, using analogies that relate to patients’ everyday experiences, and encouraging questions can significantly improve comprehension. In addition, involving trained interpreters or visual aids may further enhance patient understanding, particularly for those with lower health literacy levels. By adopting these strategies, the informed consent process can become more inclusive, ensuring that patients are truly informed and actively engaged in their healthcare decisions.
Unguided use of the internet as an alternative source of information for patients
The use of medical jargon led some patients to seek information from the internet. One participant mentioned, “They didn’t say much; the explanation was more confusing because she introduced some medical terminologies in her explanation that I didn’t understand. As a result, I had to search online to find out more about my condition and the procedure. . . participant 9.” This unguided use of the internet as an alternative source of information reflects a gap in communication and highlights the need for healthcare providers to simplify their language and offer clearer explanations to avoid patient confusion and misinformation.
Discussion
The findings from this study reveal significant gaps between the theoretical expectations of the informed consent process and the practical experiences of patients. Despite the assumption that the consent process was being conducted effectively in line with Joint Commission International guidelines and hospital policies, many patients reported that the information provided was inadequate, superficial, and difficult to understand. This disconnect is consistent with research from Sri Lanka and China, where medical jargon and technical language often hinder patient comprehension.11,12 Such complexity in communication undermines the goal of informed consent, which is to enable patients to make well-informed decisions. There is a clear need for healthcare providers to simplify their language and ensure that the information is presented in an accessible manner.
The study also highlights the tension between patient autonomy and paternalism. While modern bioethics advocates for patient autonomy and shared decision-making, some patients in this study felt that doctors, as authoritative figures, were better positioned to make treatment decisions. This paternalistic approach seems to be influenced by cultural and religious factors, where doctors are viewed as having the ultimate authority in decision-making. This phenomenon reflects similar findings in other studies conducted in comparable cultural contexts.7,13,14 Despite the emphasis on patient autonomy, many patients still defer to their doctors’ expertise, indicating a persistent paternalistic attitude in medical decision-making. 15
Interestingly, the primary motivations behind patients’ final decisions were not solely based on the information provided but were also influenced by practical concerns such as delays in healing, support from attending doctors, and fear of complications. This suggests that while information is crucial, other factors play a significant role in shaping patient decisions. This aligns with findings from Pakistan, where practical and emotional considerations were more influential than the information itself. 16 The presence of family members during the consent process also emerged as a significant factor, with patients who had relatives present feeling more supported and able to make informed decisions. This is consistent with research from Taiwan, which found that family involvement increased decision-making support. 17 In cultures where family involvement is integral, ensuring that family members are included in the consent process can enhance the overall experience and decision quality.
The study also identified issues related to the timing of consent and the role of junior medical staff. Patients reported feeling rushed and inadequately informed, particularly when consent was obtained by residents or medical officers who may lack the detailed knowledge necessary to explain procedures comprehensively. This observation aligns with other studies highlighting challenges in consent timing and delegation.18,19 Ensuring that consent is obtained well in advance and by experienced professionals can improve the quality of the informed consent process.
Moreover, the study found varied perceptions of informed consent, with some patients viewing it as a mere formality required to receive treatment. This contrasts with the ethical principle of informed consent, which should empower patients to make autonomous decisions based on a comprehensive understanding of their options. This finding echoes previous research indicating that many patients see informed consent primarily as a legal safeguard rather than a tool for empowerment.20,21 Addressing this perception gap through better education and communication about the purpose and importance of informed consent is crucial for bridging the divide between patient expectations and actual practice.
A historical perspective on informed consent provides valuable insights into the evolution of medical ethics and patient rights. In the 16th–17th century Ottoman Empire, informed consent was documented as a formalized process in surgical procedures, highlighting an early recognition of the necessity for patient involvement in decision-making. 22 A study by Degerli 22 on informed consent practices in 17th-century Ottoman Istanbul revealed that surgeons performing hernia surgeries sought explicit patient agreement before proceeding, reflecting an early model of patient autonomy and medical ethics. While contemporary healthcare systems have advanced significantly, the fundamental principle of obtaining voluntary and informed consent remains unchanged. Understanding these historical practices can inform present-day improvements, particularly in ensuring that informed consent is not just a bureaucratic requirement but a meaningful process of shared decision-making.
In terms of strengths, this study’s detailed methodological approach and qualitative methods provide a comprehensive view of patient perspectives. The use of raw participant quotes and rigorous analytical methods enhances the credibility and transferability of the findings. By focusing on patients’ views in a Sub-Saharan African context, the study adds valuable insights to the global discourse on informed consent.
Limitations
One significant limitation of this study is the potential for selection bias, as participants were drawn from a specific hospital setting in Sub-Saharan Africa, which may not fully represent the broader population or other healthcare contexts. In addition, the reliance on patient self-reports for assessing understanding and satisfaction with the informed consent process may introduce subjective biases. Patients might have different thresholds for what they consider sufficient information or satisfactory consent, which could affect their responses. Furthermore, the study’s cross-sectional design limits the ability to capture changes in patient perceptions over time, particularly in relation to evolving consent practices and patient education.
Conclusion
This study highlights critical gaps in the informed consent process, particularly concerning patient comprehension and satisfaction. Many patients reported receiving insufficient information, often conveyed in complex medical jargon that hindered their understanding. In addition, time constraints and a lack of structured discussions further compromised the quality of consent. Cultural influences and lingering paternalistic attitudes also shaped patient experiences, affecting their sense of autonomy in decision-making.
To enhance the informed consent process, healthcare providers should prioritize the use of clear, simple language, avoid medical jargon, and allocate adequate time for thorough discussions and patient questions. Implementing these strategies will not only improve patient understanding but also foster greater trust, autonomy, and overall satisfaction with their care.
Supplemental Material
sj-doc-1-smo-10.1177_20503121251331122 – Supplemental material for Patients’ perceptions and understanding of preoperative informed consent: A qualitative thematic analysis from Tanzania
Supplemental material, sj-doc-1-smo-10.1177_20503121251331122 for Patients’ perceptions and understanding of preoperative informed consent: A qualitative thematic analysis from Tanzania by Steven Michael, Willbroad Kyejo, Allyzain Ismail, Sunil Samji, Eric Aghan, Columba Mbekenga and Athar Ali in SAGE Open Medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.