
Abstract
Objective:
To evaluate and validate the medically necessary and time sensitive score by testing the variables, in order to create a surgical preoperative score for procedure prioritization in COVID-19 pandemic in Colombia.
Methods:
A multicenter retrospective cross-sectional study of instrument validation with a cultural adaptation and translation into the Spanish language was carried out in Bogota, Colombia. Patients over 18 years of age who had undergone elective procedures of general surgery and subspecialties were included. The translation of the medically necessary and time sensitive score into Spanish was performed independently by two bilingual surgeons fluent in both English and Spanish. A final version of the Spanish questionnaire (MeNTS Col) for testing was then produced by an expert committee. After translation and cultural adaptation, it was submitted to evaluate the psychometric properties of the medically necessary and time sensitive score. Cronbach’s α was used to represent and evaluate the internal consistency and assess reliability.
Results:
A total of 172 patients were included, with a median age of 54 years; of which 96 (55.8%) patients were females. The vast majority of patients were treated for general surgery (n = 60) and colon and rectal surgery (n = 31). The evaluation of the internal consistency of the scale items in Spanish version was measured, and values of 0.5 for 0.8 were obtained. In the reliability and validation process, Cronbach’s α values in all items remained higher than 0.7. The new MeNTS Col model was analyzed, and a result of 0.91 was obtained.
Conclusions:
The Spanish version of the medically necessary and time sensitive, the MeNTS Col score, and its respective Spanish translation perform similarly to the original version. Therefore, they can be useful and reproducible in Latin American countries.
Introduction
The COVID-19 pandemic forced surgeons to reconsider concepts of “elective” surgery.1–3 Perceptions about the time sensitivity and medical necessity of a procedure have taken on a greater significance during the pandemic. In order to objectify surgical decision-making and to optimize the use of resources at each institution associated with patient risk, in an ethical and efficient manner in the COVID-19 pandemic. 2 During the course of 2020, Prachand et al. 4 quickly designed the MeNTS Score (medically necessary and time sensitive), with the aim of addressing the difficulties of prioritizing surgical procedures. 4 This score was of great importance because perioperative mortality in asymptomatic patients undergoing elective surgery with SARS-CoV-2/COVID-19 can vary according to the reported series from 20.5% to 28%, reaching a morbidity requiring mechanical ventilation and intensive care unit (ICU) of up to 40%.5–7
The evolving ethical and clinical environment requires reappraisal of perioperative factors, such as personal protective equipment conservation; limiting the risk of exposure to COVID-19 for patients, families, and healthcare workers; preservation of hospital beds and ICU resources; and minimizing COVID-19-related perioperative risk to patients.8–10 In low- and middle-income countries, medical aspects with an ethical, economic, social, and outcome focus are more relevant, due to barriers to access to specialized surgical care centers, availability of specialists and high-tech resources, catastrophic spending rate, high demand for medical services, among many others.11,12 According to the objectives of global surgery for the year 2030, it is necessary to develop and validate tools that contribute to the control of surgical diseases and improve surgical care practice, with priority being given to the economization of limited resources. 13
In Latin America, a region composed of low- and middle-income countries, a tool such as MeNTS has never been adapted and validated to objectify the priority of elective surgeries in times of pandemic. This means that there is currently no Spanish version available, even though it is one of the three most widely spoken languages in the world. 14 Given that Latin America is still under the scourge of COVID-19, and that new public health crises due to emerging infectious diseases are expected to continue to appear, 15 a translation, cultural adaptation, and validation of the Spanish version of the MeNTS is required. Then, the aim of this study is to validate the Spanish cross-cultural adaptation of the MeNTS tool, as well offer modifications to the MeNTS criteria for improved application in countries similar to Colombia.
Patients and methods
Study design
A multicenter retrospective cross-sectional study of instrument validation with a cultural adaptation and translation into the Spanish language was carried out in Bogota, Colombia, between April 2020 until August 2020. Four tertiary national referral centers participated.
Subjects and setting
Patients over 18 years of age who underwent elective procedures of specialties of general, breast, head and neck, gastrointestinal, colon and rectum, hepatobiliary, and bariatric and hepatobiliary surgery were included. The data were collected from the databases of each institution. Only those patients who had all the sociodemographic variables and surgical variables necessary to evaluate the MeNTS Score were included for the study analysis. As exclusion criteria, it was defined that patients under 15 years of age, pregnant women, and patients treated surgically in other institutions would not be included.
Cross-cultural adaptation and validation processes
The translation of the MeNTS score into Spanish was performed independently by two bilingual surgeons fluent in both English and Spanish; then a meeting of the two surgeons to resolve the discrepancies was performed. Unresolved queries were cleared. Subsequently, the Spanish versions were translated back into English by two other surgeons, in order to develop a back-translation, aimed to verify the congruence of the translation, that is, conceptual and linguistic equivalence of the original instrument. To assess the equivalence of the translated version to the original scale, a group of two surgeons answer the scale of medical records of 30 patients; then, two different surgeons completed in the English version. A final version of the Spanish questionnaire (MeNTS Col) for testing was then produced by an expert committee composed of three surgical specialists, one methodologist, and the translators and language professionals involved in the process.
MeNTS score
The original MeNTS scoring criteria attempt to objectively prioritize surgeries by grading 21 factors within the broad categories of procedure variables, disease state, and comorbidities (Table 1). 16 The cumulative score ranges between 21 and 105 and serves as a rank in priority, with lower numbers equating to greater priority. Higher scores equate to poorer perioperative outcomes, higher hospital resource utilization, increased risk of COVID-19 transmission, and an increased ability to safely defer surgery.
Original version of the MeNTS score. 16

CAD: coronary artery disease; CF: cystic fibrosis; CHF: congestive heart failure; COVID-19: novel coronavirus; CPAP: continuous positive airway pressure; CV: cardiovascular; GI: gastrointestinal; HTN: hypertension; ILI: influenza-like illness; LOS: length of stay; Med: medication; MIS: minimally invasive surgery; OHNS: otolaryngology, head & neck surgery; OR: operating room; PO: by mouth.
Hematologic malignancy, stem cell transplant, solid organ transplant, active/recent cytotoxic chemotherapy, anti-TNFa or other immunosuppressants, >20 mg prednisone equivalent/day, congenital immunodeficiency, hypogammaglobulinemia on intravenous immunoglobulin, AIDS.
Statistical analysis
Statistical tests were performed in the statistical program STATA® 14.0. Qualitative variables were summarized using frequency and percentages. After translation and cultural adaptation, it was proceeded to evaluate the psychometric properties of the MeNTS score. Cronbach’s α was used to represent and evaluate the internal consistency and assess reliability. The minimum acceptable value was 0.70. Construct validity was assessed using the Spearman correlation test. The statistical significance for the threshold retained for all tests was p < 0.05.
Ethical considerations
Due to the pandemic, this study was reviewed and approved in an extraordinary session by the Ethics Committee of the Hospital Universitario San Ignacio. In addition, it followed the norms established by the Declaration of Helsinki 17 for the guarantee of human rights in medical research.
Results
Population
A total of 172 patients were included, with a median age of 54 years; of which 96 (55.8%) patients were females. Included patients ranged from general surgery (n = 60), breast (n = 19), bariatric (n = 29), colon and rectum (n = 31), head and neck (n = 18), hepatobiliary (n = 4), and gastrointestinal surgery (n = 11). The comorbidities included cardiovascular disease in 83 patients, lung disease in 29, type 2 diabetes mellitus in 79, immunocompromise in 66, and obstructive sleep apnea syndrome in 31 patients (Table 2).
Baseline characteristics of the study population.

BMI: body mass index; CPAP: continuous positive airway pressure.
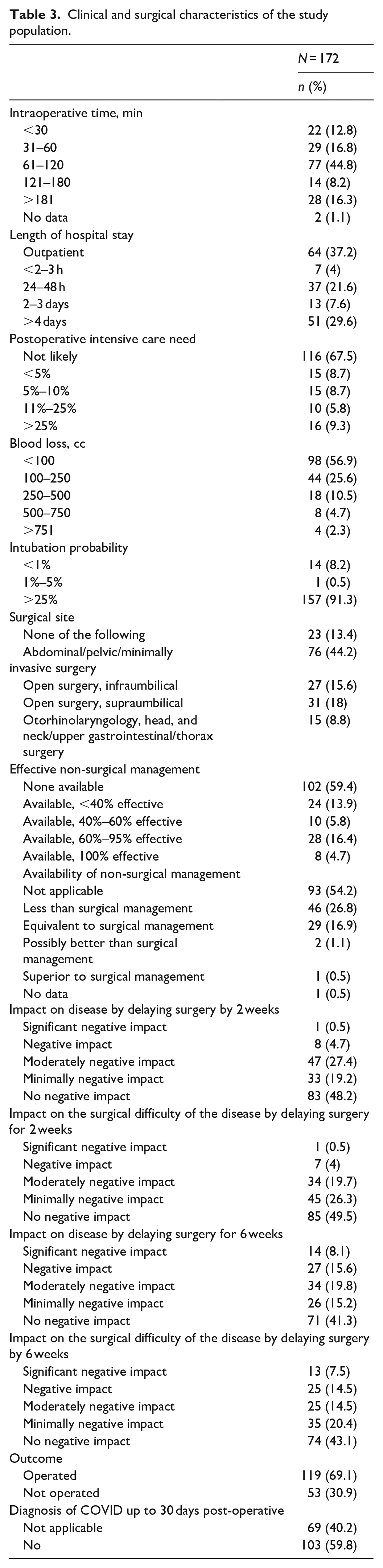
Intraoperative time interval of 60–120 minutes (n = 77; 44.7%), postoperative outpatient management (n = 64; 37%), and no admission to postoperative intensive care (n = 116; 67.4%) were found to be the most frequent surgical variables. It was found that by delaying surgery for 2 weeks, 48.2% (n = 83) had no negative impact, and 49.4% (n = 85) had no surgical difficulty of the disease. By delaying surgery for 6 weeks, predominantly 41.2% (n = 71) had no negative impact, and 43% (n = 74) had no surgical difficulty with the disease. 69.1% (n = 119) of the population underwent surgery, and no evidence of COVID-19 infection was reported at 30 days postoperatively (Table 3).
Clinical and surgical characteristics of the study population.
Cross-cultural adaptation or translation
In the cultural adaptation phase, there was good agreement between the translated and the original English version. The review required only minimal word changes, the limit of 10% of incomprehension was not surpassed, making the final Spanish version of the scale culturally appropriate (Table 4).
Spanish version of the MeNTS score.

UCI: Unidad de Cuidados Intensivos; CPAP: Presión Positiva Continua en la Vía Aérea (Continuous Positive Airway Pressure).
Internal consistency reliability
The evaluation of the internal consistency of the scale items was measured using Cronbach’s α, and values of 0.5 for 0.8 were obtained. In the reliability and validation process, Cronbach’s α values in all items remained higher than 0.7. Because they are categorical variables, intra-observer and inter-observer reliability were evaluated by Spearman’s correlation coefficient, obtaining a value >0.7.
Face and content validity
In the process of understanding and relevance, the scoring averages and minimum and maximum scoring values were considered in all questions assessed by professionals, showing the face and content validity.
Concurrent validity
The comparison between the MeNTS and the MeNTS Spanish version demonstrated a high correlation (Spearman’s correlation > 0.7).
Validity of the construct
Variables that affected decisions on the original MeNTS scale and possible factors that may have been overlooked were explored. The representativeness of all components was evaluated, and only those components that showed representativeness in the described domains were retained.
When evaluating the construct, it was found that some variables affected the total representativeness of the model, decreasing the representative value. For this reason, within the domain of factors associated with the procedure, three variables were eliminated: (1) Surgical time, (2) People on the surgical team, and (3) Need for intubation. In the second domain, two variables were eliminated: (1) Effectiveness of non-surgical management and (2) Availability of non-surgical management. And finally, in the domain of factors associated with the patient, 3 variables were eliminated: (1) Immunocompromised, (2) Influenza-like illness, (3) Exposure to COVID-19 patients in the last 14 days. The new MeNTS Col model was analyzed, and a result of 0.91 was obtained.
MeNTS Col score
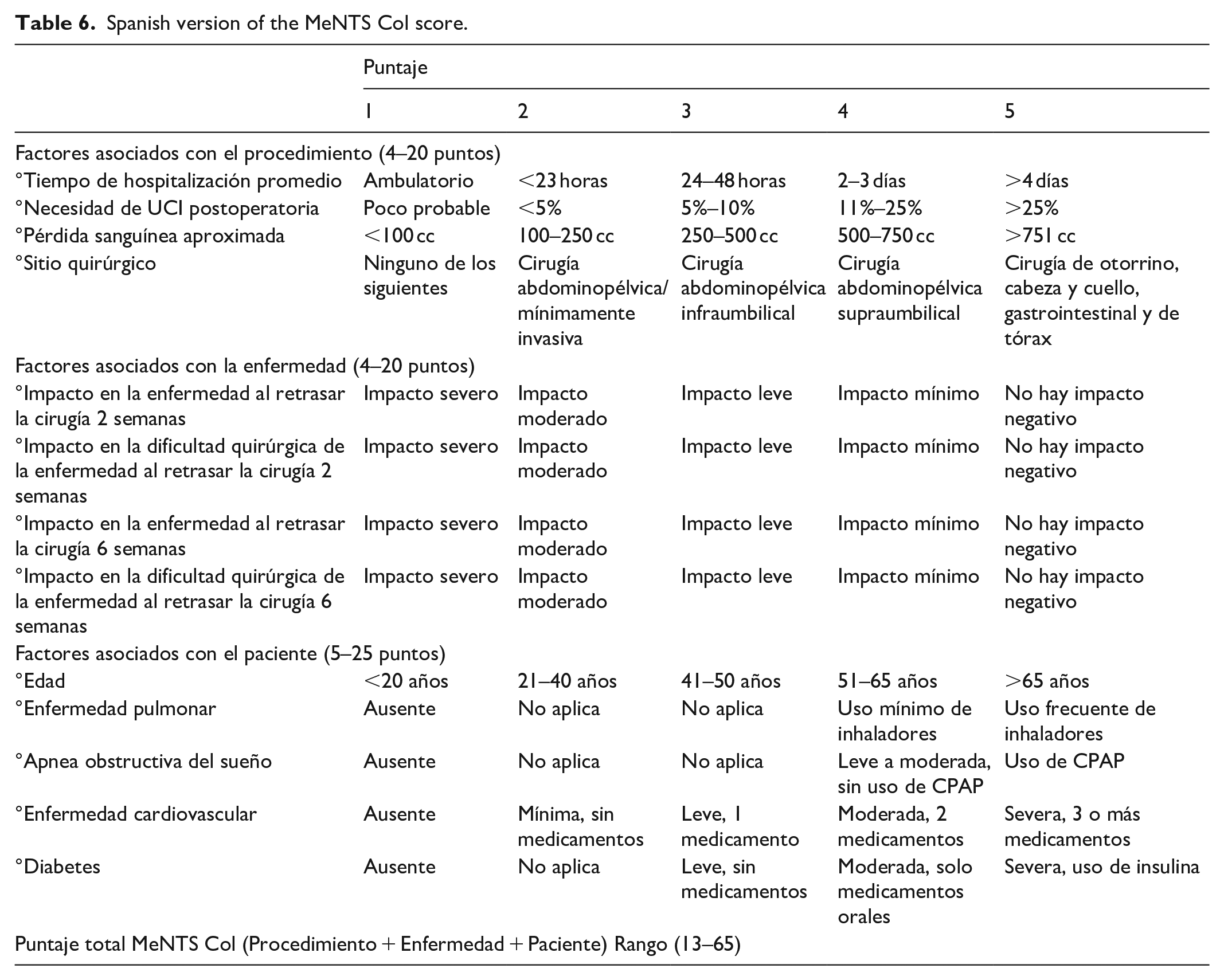
The MeNTS Col score attempts to objectively prioritize surgeries by grading 15 factors within the broad categories of procedure variables, disease state, and comorbidities. The cumulative score ranges between 13 and 65 and serves as a rank in priority, with lower numbers equating to greater priority. Higher scores equate to poorer perioperative outcomes and higher hospital resource utilization. The MeNTS Col score is presented in Table 5, and the final Spanish version in Table 6.
MeNTS Col score.

LOS: length of hospital stay; ICU: intensive care unit; EBL: estimated blood loss; OHNS: otorhinolaryngology and head and neck surgery; GI: gastrointestinal; CPAP: continuous positive airway pressure.
Spanish version of the MeNTS Col score.
Discussion
With the emergence of the COVID-19 pandemic, evidence surfaced recommending rapid modifications in the flow of patients with surgical needs to ensure rational management of the most urgent diseases.18–23 In the initial stage, it was found that a small but significant number of patients who were involuntarily scheduled for elective surgeries during the COVID-19 incubation period, which could have put both the healthcare team and the patient at risk, without accurately assessing the urgency of the surgery. 6
One of the first and most representative analyses that studied this phenomenon was performed by Lei et al., 6 who analyzed clinical data from 34 patients undergoing elective surgeries during the COVID-19 incubation period in Wuhan (between January and February 2020). 6 The authors observed that all patients developed COVID-19 pneumonia shortly after surgery with abnormal findings on chest CT scans. Common symptoms included fever, fatigue, and a dry cough; 15 patients required admission to the ICU during progressive disease, and 7 patients died after admission to the ICU (20.5% mortality). 6 Compared to patients who did not require an ICU admission, those patients who were in need of intensive care were older, more likely to have underlying comorbidities, underwent more difficult surgeries, and more severe laboratory abnormalities (e.g., leukopenia, lymphopenia). The most common complications in non-survivors included acute respiratory distress syndrome, shock, arrhythmia, and acute cardiac injury. 6 Based on this type of findings, the MeNTS score was designed, since some variables such as age, comorbidities, type of surgical procedure, among others, proved to have a high predictive value for mortality. For this reason, it was also used in our scale, adapted according to the performance of the items, and the outcome of the patients was studied.
During the COVID-19 pandemic, there were many examples of the impact that surgical decision-making can have on outcomes in times of crisis. The COVIDSurg study, a well-known international cohort study, which evaluated 1128 surgical patients from 235 hospitals worldwide, served as the basis for the development of tools that could classify and prioritize patients who needed to be operated on within a specific time frame and recovered under strict conditions during the pandemic. 7 This study found that 74% of the surgeries performed were emergency surgeries, with preoperative confirmation that almost 30% had SARS-Cov 2 infection, and that survival was 76%. Pulmonary complications occurred in more than 50% of the cases (n = 577), which accounted for 81.7% of the total number of deaths in the study (n = 219/268). When investigating the factors associated with mortality, it was found that being male (OR 1.75; 95% CI 1.28–2.40, p < 0.0001), age > 70 years (OR 2.30; 95% CI 1.65–3.22, p < 0.0001), having obstetric diagnosis or malignancy (OR 1.55; 95% CI 1.01–2.39, p = 0.046), undergoing an emergency surgery (OR 1.67; 95% CI 1.06–2.63, p = 0.026), and major surgery (OR 1.52; 95% CI 1.01–2.31, p = 0.047) were significantly associated with higher mortality. This gave rise to various recommendations based on available evidence to give priority in times of public health crisis, such as a pandemic or endemic, and to really urgent surgeries. Similarly, the risk of modification of immediate surgical outcomes due to active infection by emerging agents is weighed. But beyond that, it is also a good evidence-based support on the need to adapt priorities according to the health system context and capacity of care, since there are notable differences between high-income versus middle- and low-income countries, which supports the design of scales socially and culturally adapted to the differences in conditions, compared to the original scales.
In our adaptation of the MeNTS score, we identified that the variables operating room time, surgical team size, and intubation needed to perform procedure (probability) did not have a great impact; we considered that procedures without intubation requirement were not relevant for our study since the generation of aerosols will be mainly linked to procedures such as orotracheal intubation. Delighted with the surgical team size despite the economic condition of our country, the necessary personnel will always enter to perform the procedure. In addition, in many centers, the entry of personnel in training was limited (students, interns, and residents).
Regarding the disease variable, non-operative treatment option should be considered in pathologies that medical management has a global validity it is used in the first instance (always evaluate effectiveness versus resource use/exposure risk), and in cases where there is no global standardized concept such as the use of antibiotics, for example, treating acute appendicitis has not had a global acceptance in our environment. Regarding the patient variables, influenza-like illness syndrome (fever, cough, sore throat, body aches, diarrhea) and exposure to known COVID-19 (patient positive or with symptoms within a 14-day interval) did not have a statistical significance, and this is because if these variables were present in any of the centers, they were considered candidates for surgical management for outpatient surgery.
A potential limitation of this study could be the consecutive convenience sampling used. This sampling does not always produce the most accurate results due to a skewed representation, and we are aware that our study group might not represent the Colombian population. Nevertheless, we believe that these limitations do not compromise the results obtained in the validation. 24 Surgeries that did not necessarily require intubation were not evaluated. At a global level, the cases of diagnosis of COVID-19 have been decreasing in some countries. However, in countries like ours, we are still on a plateau with an approximate of 7000 patients diagnosed per day. 25 Apparently on a plateau, so we consider that an adaptation in elective surgery is necessary, and therefore, the MeNTS Col will be of great utility.
Conclusions
The Spanish version of the MeNTS, the MeNTS Col score, and its respective Spanish translation, perform similarly to the original version. Therefore, they can be useful and reproducible in Latin American countries in rational decision-making about the priority of surgical interventions in regional or global public health crisis situations.
Footnotes
Acknowledgements
None.
Authors contribution
L. T., O. G., and C. P. R. contributed to methodology and validation. I. D. L. M., C. S., M. P., S. A., and A. R. N. R., contributed to writing the original draft, reviewing, and editing. L. F. C. V. contributed to investigation and resources.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from *Ethics Committee of the Hospital Universitario San Ignacio*. However, the approval was made in an extraordinary session due to the pandemic period, hence no number or minutes were assigned.
Informed consent
Due to the time of the pandemic, the retrospective nature of the study, and the low risk of the study (as determined by the national legislation), the need for informed consent was waived.
Trial registration
N/A