
Abstract
Background:
In emergency situations, patients and their next of kin must make complex medical and ethical decisions in a quick and timely way.
Objectives:
To describe the decision-making process during informed consent for emergency surgery among patients and the next of kin of patients who have undergone emergency surgery.
Methods:
Consecutive sampling of 39 participants and in-depth semi-structured interviews were conducted at two tertiary teaching hospitals in Uganda. There were 22 patients and 17 next of kin of patients who had undergone emergency surgery within 24–72 h. Responses about decision-making were coded into themes using the social constructivist theory and phenomenological approach
Results:
There were four emergent themes; decision-makers, people consulted, documentation of the consent and factors influencing decision-making. Most patients and next of kin made decisions on their own and documented the consent for themselves. Other family members and doctors were consulted during the decision-making process. Decision-making was influenced by reassurance of good outcomes of surgery and disclosure by the doctors.
Conclusion:
Decisions were made collaboratively with the patient at the center but with input of health personnel, the next of kin and other family members. A communitarian approach combined with shared decision-making between the doctor and the patient and next of kin with adequate discussion and disclosure of information in simple language would improve decision-making for patients and their next of kin.
Introduction
Informed consent is a process of constant dialogue between the clinician or investigator and the patient or their next of kin (NOK). The purpose of this dialogue is to respect a patient’s wishes and values (autonomy) and to ensure that the treatment is according to the patient’s choice and what the patient would like to be achieved from the treatment.1,2 Informed consent involves continuous communication throughout the care of the patient and is not simply “an event or a signature on a form.” 3 Informed consent process involves alternative options, adequate disclosure of risks, benefits, nature of the procedure, confidentiality, understanding, decision-makingand ends with documentation of the consent. The decision-making process culminates in the documentation of the decision in the form of a signature on the consent form. The consent form may be designed using an autonomy-enhanced model of consent where the patient’s autonomy and understanding are sought, or a harm-avoidance model where the physician seeks to avoid any liability or litigation. 4 In an emergency setting the goal of consent might be a combination of these two models and the signature represents an individual’s decision or that of the NOK/surrogate decision-makers for patients who do not have the capacity to consent.
Decision-making by patients undergoing emergency surgery and their NOK typically involves the patient’s healthcare providers discussing the patient’s condition and treatment options with the patient and or their NOK and seeking their consent for the recommended course of action. Autonomous decision-making during the informed consent process relies on the patient understanding the information given and making an informed choice. 5 Often, shared decision-making in which patients or their NOK discuss the options available, the risks and the benefits and a decision is made based on adequate disclosure and continuous communication between the patient and the surgeon is used.6–9 Shared decision-making emphasizes the patient’s understanding of the different treatment options based on the patient’s values and lived experiences.10,11 The patient or their NOK must have the competence and the capacity to understand and therefore come to an informed decision about the patient’s care.
The decision-making process for patients and their NOK in an emergency can be challenging because of a myriad of complex medical and ethical considerations that must be made in time-pressure situations as well as challenges in accessing emergency and critical care. Emergency care in low-income countries like Uganda has inadequate human resources and a lack of access to health care services because of poor road infrastructure, poorly equipped emergency units and overcrowded health facilities. Healthcare financing in the form of health insurance is often non-existent for most of the population who seek care at public hospitals, while a few who have health insurance may seek care at private institutions, which are less crowded and better resourced.
In addition to the above, the patient’s capacity to consent in an emergency setting may be impaired by one’s medical condition, pain and anxiety, and yet one must make decisions that have significant and far-reaching consequences for the patient’s well-being and quality of life. When the patient does not have the capacity to consent, decisions may be made by the NOK, surrogate decision-makers, legally appointed representatives, or the health care providers with the guidance of hospital ethics boards. The NOK is defined according to what role they have to play in making decisions about healthcare, decisions following the death of an individual and sometimes being appointed by the patient prior to the situation. 12 The NOK is required to do the following during decision-making: respect the patient’s wishes, ensure that the best interests of the patient are represented and that the decision made is what the patient would most likely have done. Sometimes the patient’s best wishes are unknown or have not been expressed previously to the NOK and this may result in the NOK’s decisions not accurately representing the patient’s best wishes.13–15 The NOK may therefore consult other stakeholders like other family members or the community to avoid making decisions contrary to the patient’s best interests.
In an emergency setting, a patient who does not have the capacity to consent may consult one’s NOK, who in turn may consult key members in society and other caregivers for the patient through “a communitarian approach” to obtain consent. 16 The communitarian approach is whereby ethical problems are analyzed based on the individual good versus the common good, the effect on societal welfare and involves the participation of the community in finding solutions to the problem. 17 The communitarian approach to decision-making, though sometimes in conflict with the patient’s autonomy, may provide a more holistic treatment context in an emergency setting.
A scoping review on shared decision-making found that patients and surgeons prefer shared decision-making during informed consent for surgical care although there was no evaluation of shared decision-making in an emergency setting. 18 However, an international survey among surgeons from mainly high-income countries in Europe on shared decision-making in emergency surgery highlighted the need for shared decision-making practices to be included in clinical guidelines to improve understanding of shared decision-making among surgeons. 19 Other studies noted that poor patient comprehension of informed consent during an emergency affects the patient’s decision-making process and proposed a more interactive structured informed consent process to enable patients to make decisions for themselves without relying blindly on doctors.19,20 These studies have tackled the aspect of shared decision-making from the perspectives of the patient and clinician but have not considered other concepts of patients or their NOK use in decision-making that may arise in an emergency setting of a low-income country. This qualitative study explored the decision-making process of patients undergoing emergency surgery and their NOK in one public and one private tertiary teaching hospital in a low-income African country. We aim to describe how decision-making by patients and their NOK in the two emergency settings is done while considering concepts of shared decision-making and a communitarian approach that may be employed to address the challenges of decision-making during informed consent for emergency surgery. Using PICO, the population under study were patients and the NOK of patients who had undergone emergency surgery within 24–72 h, the phenomenon of interest was informed consent, the context was in private versus public hospitals and the outcome was decision-making following the informed consent.
Methods
This was a qualitative study where in-depth interviews were conducted among patients who had undergone emergency surgery and the NOK of patients who had undergone emergency surgery at the emergency units of two tertiary teaching hospitals: one public Mulago National Referral Hospital and one private Nsambya Hospital.
Study design and setting
The study was based on the social constructivist theory and used a phenomenological approach to explore how the patients and their NOK made decisions during the informed consent process for patients undergoing emergency surgery. The social constructivist theory in decision-making refers to decision-making within a specific social context and holds that behavior is a result of social interaction.21,22 Meaningful understanding acquired for decision-making is through social interpersonal interaction and developed jointly by individuals. 23 Meaningful understanding is not inherently possessed in an individual’s mind but is rationalized from their experiences in the social world. It was a qualitative study using in-depth interviews of patients and the NOK of patients who had undergone emergency surgery within 24–72 h from the time of recruitment into the study. The interviews were conducted at the Accident and Emergency units of Mulago National Referral Hospital and Nsambya Hospital. Mulago National Referral Hospital is a 1750-bed public tertiary hospital in Uganda that receives an average of 50 patients a day in its Accident and Emergency department. Nsambya Hospital is a 300-bed faith-based private-not-for-profit hospital and receives an average of 20 patients a day in its Accident and Emergency unit. Both are urban university teaching hospitals located in Kampala, the capital city of Uganda. There were other patients with surgical emergencies, emergency staff, relatives of other patients, ambulatory care staff and police officers who were bringing in patients with surgical traumatic injuries in the accident and emergency units. The study was conducted between July 2021–January 2022.
Participants and sampling
Participants were patients and the NOK of patients who had undergone emergency surgery within 24–72 h. There was convenience consecutive sampling of study participants because it was the most appropriate sampling method of collecting qualitative data quickly and at a low cost from specific study participants who had undergone emergency surgery at the emergency units.
Inclusion criteria for patients
Patients had to have undergone emergency surgery within 24–72 h. Patients had to be 18 years and above, and patients had to be able to communicate and provide consent for the study.
Exclusion criteria for patients
Patients who were too ill to communicate or provide consent. We excluded those who could not communicate in the common local language Luganda, English, or Kiswahili.
Inclusion criteria for NOK
The NOK had to be 18 years and above. They had to have had a patient who had undergone emergency surgery within 24–72 h. They had to have been present at the time of consent for surgery for their patient.
Exclusion criteria for NOK
We excluded those NOK whose patients had been interviewed as patient participants in the in-depth interviews. We excluded those who could not communicate in the common local language Luganda, English, or Kiswahili. We also excluded NOK who did not consent to take part in the study.
Twenty-eight patients and twenty-three NOK were approached for a face-to-face interview. Six patients and six NOK were excluded because of the language barrier whereby the participants did not understand any of the local indigenous languages spoken in Uganda only spoke Arabic and Aramaic, had no interest in participating in the study, or did not feel comfortable discussing their patient’s condition. We therefore interviewed twenty-two patients and seventeen NOK of patients who had undergone emergency surgery.
Study procedure
Data collection
In-depth, interviews were conducted using a semi-structured interview guide by two trained research assistants in a private room adjacent to the Accident and Emergency wards at each health institution. The interview guide was initially piloted among three patients and two NOK of patients in Mulago National Referral Hospital, and two patients and two NOK of patients in Nsambya Hospital which was 21% of the study population. Amendments were made to the probes for each of the questions for better clarity of the responses given. There was no relationship established between the research assistants and the participants prior to the study. The research assistants had experience conducting research in other research groups.
Interviews were conducted in English which is the official language used in Uganda, or Luganda, which is the most widely spoken local language in the capital city Kampala. The interview guide had questions assessing attitudes towards the informed consent process, decision-making in the informed consent process, knowledge and communication of the informed consent process, resources affecting the informed consent process and emergency staff’s role in the informed consent process.
All interviews were audio recorded and lasted 20–30 min. Audio recordings were transcribed verbatim by the research assistants. Interviews that were conducted in Luganda, the most widely spoken local language, were translated into English by the research assistants during transcription. All the transcripts were checked for accuracy with the audio recordings by the principal investigator and corrections were made.
Data analysis
The transcripts were coded and thematic analysis was done using Nvivo version Release 1.0 computer software (manufactured by Lumivero) by two coders OK and a second independent reviewer AT. All responses from patients and the NOK were coded independently by each reviewer and a coding framework using five transcripts from patients and four transcripts from the NOK was developed by OK and AT. The codes were categorized under four emergent themes which were derived following a discussion between the two reviewers and a third independent reviewer EM. The four emergent themes were (1) decision-makers in the informed consent process, (2) people consulted during the decision-making, (3) documentation of the consent (4) factors influencing decision-making. Social constructivist theory was the underlying theory that was applied to code responses that referred to decision-making made with consultation of other family members by the patient and their NOK and who made the decisions. Factors that influenced decision-making were derived from the experiences of the patients and the NOK using a phenomenological approach. Documentation of consent was described under the phenomenological approach from the experiences of the participants. The responses were reviewed by the PI and the research assistants to identify any new ideas before continuing with further interviews. Data saturation was considered achieved when no new insights were identified by the three reviewers after every five interviews. The transcripts were not shared with the participants afterward because it was not feasible to contact some participants after discharge from the health institutions due to some participants having incomplete or inaccurate contact information.
Data quality control
Peer briefing was done with EM, IM and MG to review the responses and provide feedback on the interview process. The responses were reviewed by the PI, and the research assistants after every five interviews to ensure that the information collected was accurate and consistent. A second independent reviewer reviewed the audio recordings and the transcripts for accuracy.
Training of research assistants
The principal investigator conducted two training sessions with the research assistants about responsible conduct of research and how to conduct in-depth interviews before the study begun.
The trustworthiness of this study was ensured by using credibility, dependability, confirmability and transferability as done by Forero et al., 24 in the application of these four criteria in qualitative studies in emergency medicine.
Credibility
The research team underwent training on the research protocol and piloted the interview guide to ensure adequate knowledge about the research study and determine how long the interviews would need to run to collect data accurately and adequately. The research team had adequate engagement with the participants for 20–30 min during which written informed consent was obtained and an interview guide was used to conduct the interviews.
Dependability
We used a pilot-tested interview guide which is attached to this manuscript (Supplemental file). All the audio recordings were transcribed and translated into English for those interviews where the most widely used local language Luganda was used. Both the audio recordings and the transcripts for all interviews were stored in a secure folder on the principal investigator’s computer to keep track of the data collection process. Both audio recordings and transcripts were reviewed by the PI (OK) and an independent reviewer (AT) for accuracy in translation, content and context of the responses. We did a form of back translation of the transcripts in which the research team and the independent reviewer reviewed the transcripts and translated them back to the local language and listened to the audio recordings to achieve better accuracy of information collected. 25 Three reviewers (OK, AT and EM) then coded the transcripts independently, discussed the emergent themes and resolved coding discrepancies. A codebook was then generated in Nvivo software. We however did not assess for or calculate the intercoder agreement.
Confirmability
The research team’s reflexivity is described in the section below. Triangulation of sources of data was achieved by collecting data from the patients and the NOK at the two hospitals so as to get a broader source of data and a more holistic understanding of informed consent in public and private hospital settings. Investigators’ triangulation was obtained by discussing the emergent themes and codes of the transcripts and finding consensus where there were different interpretations and perspectives of the codes of the transcripts.
Transferability
We used convenience consecutive sampling at both low-resourced public hospitals and better-resourced private hospitals in a low-income country to obtain a wide range and variety of patients with different emergency surgical conditions and thus obtain a representative sample population. The findings of this study can therefore be generalized to emergency units of varying resources in low-income countries. We ensured data saturation by the three reviewers assessing transcripts for new codes after every five interviews until no new codes or emergent themes were seen.
Research team and reflexivity
The principal investigator (PI) was a female general and gastrointestinal surgeon who is a PhD Bioethics Fellow. The PI has an interest in ethical challenges with obtaining informed consent during surgery as a surgeon who sometimes conducts emergency surgery in the emergency unit of Mulago National Referral Hospital. She has trained and supervised research by postgraduate students at Mulago National Referral Hospital for the past 14 years and has an interest in how they obtain informed consent during the conduction of research in the surgical emergency unit. This is her second mixed methods qualitative research study and has conducted and supervised several quantitative studies in surgery. The research assistant at Mulago National Referral Hospital was a female university student with 2 years of experience in conducting research. This study was her third experience in conducting qualitative research while the research assistant at Nsambya Hospital was a male year II postgraduate/surgical resident with 3 years of experience conducting research. This was his second experience in conducting qualitative research. Both research assistants have participated in conducting research as part of the research teams of other researchers in the university and the teaching hospitals where they are studying. We acknowledge that there might have been some selection bias because of the investigators recruiting from their workplace and training institutions. Research assistants may have been more likely to interview participants who had a positive experience which would reflect positively on the institution they were working in. The research assistants with less experience in conducting qualitative research may have resulted in giving the participants leading questions which would have affected the responses that were given by participants. This was mitigated by training the research assistants to use the interview guide which had specified probes to avoid leading questions.
Ethical considerations
Ethical approval to conduct the study was obtained from the School of Biomedical Sciences Research and Ethics committee of Makerere University College of Health Sciences reference number SBS 831. Administrative clearance was also obtained from both Mulago National Referral Hospital and Nsambya Hospital. Written informed consent was obtained from the patients or the legally authorized representatives or NOK of the patients. Consent to audio recording of the interviews was consented to separately. Audio recordings were on a study-approved recording device. Audio recording and transcribed interviews were transferred from the audio recording device to a password-secured laptop accessible only to the PI. Once recordings were transferred to the computer they were also checked for accuracy by the PI.
Emotional and psychological stress was anticipated in this study and was mitigated by interviewing participants 24–72 h after the surgery and also informing the participants about the availability of psychosocial counselling during the informed consent process for this study. During this study, care was taken to inform the healthcare givers about communication and care challenges expressed by the study participants to improve communication and reduce the emotional stress of the participant. If participants showed emotional distress the healthcare team was immediately informed about this and where possible a social worker and a counsellor were assigned to the participants.
Results
A total of 39 interviews were conducted (22 patients and 17 NOK). Of the 22 patients interviewed, 13 were from the public Mulago National Referral Hospital, and 9 were from the private Nsambya Hospital. Of the 17 NOK interviewed, 9 were from the public hospital and 8 from the private hospital. The patients who were interviewed mainly had undergone neurosurgery (n = 13), orthopedic procedures (n = 10), abdominal surgery (n = 10) and wound management procedures (n = 6; Table 1). The NOK ranged from the patient’s spouse, adult children, siblings and in one case a co-worker.
Demographic characteristics of study participants.

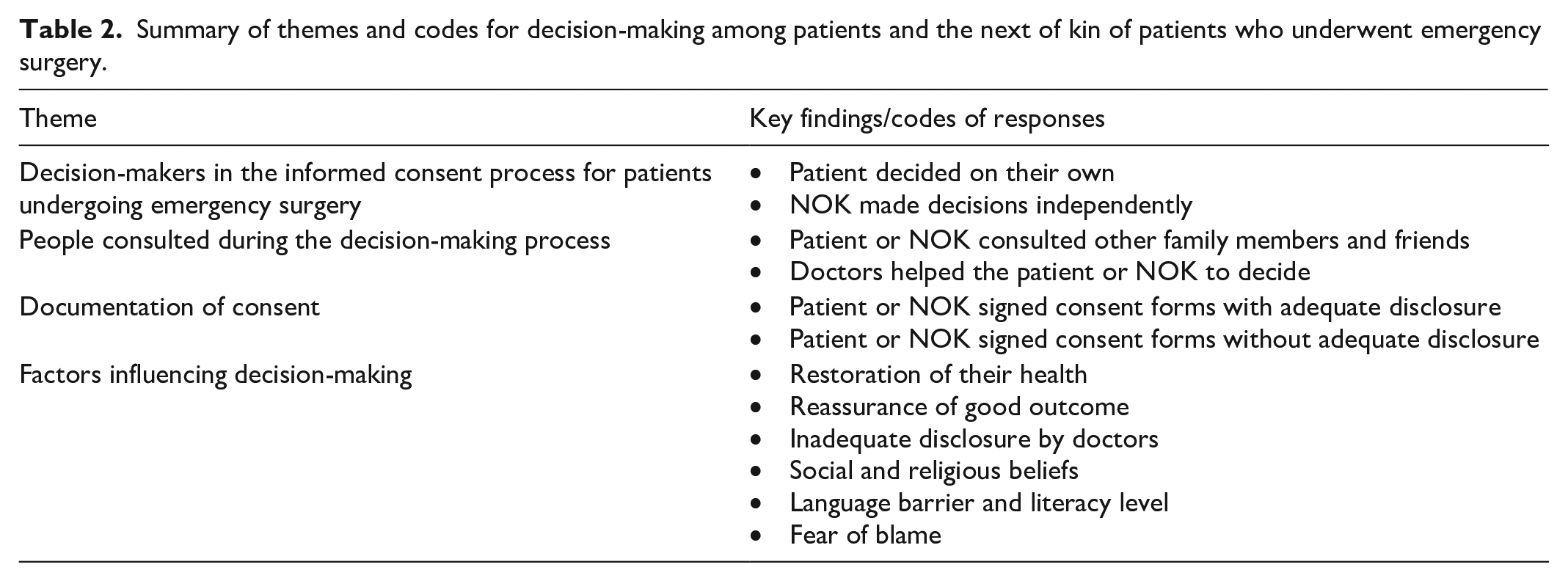
Data saturation was achieved after 39 interviews because no new insights were identified from the responses. Responses were coded under 4 emergent themes these being (1) decision-makers in the informed consent process, (2) people consulted during the decision-making, (3) documentation of the consent (4) factors influencing decision-making. The four emergent themes and the codes are summarized in the table below (Table 2).
Summary of themes and codes for decision-making among patients and the next of kin of patients who underwent emergency surgery.
Theme 1: Decision-makers in the informed consent process for patients undergoing emergency surgery
Most patients (n = 15) with capacity to consent reported that they made a voluntary decision for emergency surgery. They noted that it was because they wanted relief from their ailment and that it was within their power to make the decisions on their own without any assistance from other family members or NOK.
No one helped me. I made the decision on my own without undue influence since I was the victim here. In fact, I had been influenced by various people to be bear with the leg and not amputate it, but I got fed up (Patient 4, Private hospital). Nobody helped me, I decided because I was told “the only option is surgery, no surgery you’re just going to die.” (Patient 39, Private hospital).
Some NOK (9/17) of patients who underwent surgery made a unilateral decision on behalf of the patient, without consulting other family members. They contended that this was done to save the lives of their patients and also opined that this was in the best interest of the patient.
Nobody helped us but what forced us to decide was the condition that our patient was in because we were convinced that the operation was the only method that could help our patient to get out of the problem. (NOK 20, Public hospital).
Theme 2: People consulted during the decision-making process
The patients and their NOK (n = 14) at both institutions made decisions with the aid of other family members at both institutions. This was a form of a communitarian approach to decision-making in a challenging emergency situation. The other family members that were consulted included siblings of the patient and the NOK,
4
parents of the patient,
3
spouses of the patient,
5
and extended family members.
2
The other person(s) consulted was at times higher in the family hierarchy for example, the father, an older sibling who would give the NOK permission to consent on behalf of the patient.
The father is the one who decided for me because he is the one who gave birth to the child. He told me that the boy should go for surgery and then I decided to accept. (NOK 21, Private hospital) My sister because I stay with her, and we had to be together to finish this since it was concerned with our mum. (NOK 13, Public hospital)
Most (n = 28) patients or their NOK sought the advice of the doctors or health professionals during the decision-making of the informed consent process. Even though they made the decision on their own they acknowledged that it was based on the recommendation of the doctor. In some cases (n = 4), the NOK felt that the doctors made the decision for them based on the authority and expertise of the doctor and that they could not go against the doctors’ recommendations.
Basically, the doctor’s advice is always the best. So, I also had to agree with it since I cannot disagree with the instructions of the doctor (NOK 14, Private hospital). The doctor is the one who made the final decision because he is one who is more experienced than me, I do not know (patient 21, Public hospital).
The decision-making process by patients and NOK was a network with the healthcare providers and the community members and other family members. This is represented in Figure 1 below.

Decision-making diagram.
Theme 3: Documentation of consent in an emergency
Participants were asked to describe how informed consent was documented. Some participants pointed out that they signed the consent form themselves after understanding the information disclosed to them. For some participants, it is the NOK who signed the consent form. However, two NOK reported that they were just instructed to sign the form without any clear explanation as illustrated in this quote,
I[NOK] was just told to sign here and I signed, and they asked for my names and I placed my names on the form and then I was asked and I said it was okay and that’s where I stopped, (NOK 14, Public hospital).
One NOK of a patient who had an amputation reported that she was not sure of the person who signed the consent form because doctors told her that someone had already done so.
I[caretaker] wasn’t here I was the other side, and the doctors to work on the surgery told me that a certain doctor had already written in the file and permission was not asked for. They found when the file had already been signed, the patient’s leg really had to be amputated (NOK 12, Public hospital).
On the other hand, one patient made their own decision however, they requested their NOK to sign the informed consent form on their behalf.
Yes, I decided for myself. I’m the one who told my wife to sign so that I can be operated. (Patient 12, Private hospital).
Theme 4: Factors influencing decision-making
Almost all participants (patients and NOK) said that they consented to surgery because they perceived it as the best treatment option. Several participants indicated that they did not hesitate to consent to emergency surgery because most patients had life-threatening conditions that in the opinion of the doctors, could only be managed surgically.
We were convinced, and we saw that an operation was the only method that could help our patient get out of that problem. . . There is a doctor who had a scan and came up with a report confirming that the patient had no other alternative other than operation. So, we had to follow the doctor’s advice. . . (NOK 2, Private hospital). The doctor told me that the patient was severely injured. . . .So, the doctor told me that if the hand was not amputated, it could result into other health problems. The doctor told me that her kidneys and other organs would be affected. So, the only option was to amputate her. . . No, I decided, and I had to inform my patient about it, and since we wanted to rescue life, it was a better option for us to make. (NOK 37, Public hospital).
Some participants consented to surgery because of the pain they had endured, and the realization that nothing else could be done about their health condition.
Therefore, they told me that they had to amputate my lower limb and I too could see the necessity since the leg had turned black and unsalvageable. So, I had to accept it within my heart and consent to the surgery. . . I do not want anything else because I was in much pain. I did not have any other option after receiving the information that blood could not flow in my leg. I had no other option but to accept that which they told me. (Patient 4, Private hospital) The doctor is the one who made the final decision. I did so because he is the final person—okay, he is the expert in that area. I personally know nothing about medicine (NOK 21, Private hospital)
Other participants (n = 8) expressed that their decision was influenced by the reassurance from the doctors that there was going to be a good outcome of the surgery.
The doctor told me that he can be operated very well and he can easily recover and the doctor said it’s however my own consent to agree that he must be operated and indeed I accepted, he talked me (NOK 18, Public hospital). Doctors reassured me that my patient needed the operation and that gave me confidence (NOK 7, Private hospital).
There was a knowledge gap about informed consent. Most participants said they did not receive sufficient information about surgery
Anyway, I expected more information to be informed about the information so that am aware so much yeah. But I went there with scanty information, about the operation (Patient 10, Private hospital). They did not tell me anything. May be, there was language barrier, but they did not tell me anything. They gave me a book to sign because he was going to be operated (Patient 6, Private hospital).
In addition to a knowledge gap, one participant noted that their decision-making was influenced by their low literacy level and would have preferred that the informed consent was read to them and explained in a language they could understand.
oh first of all okay read to me, after reading to me, then you can explain to me in the language I understand [Yes]. Am just taking for granted that am not what? [illiterate] or am literate but somebody is talking to me in Luganda [Hmmm, yes] which is not good. I think it’s better first of all to ask me, which language can you communicate better? so that we can understand (Patient 10, Private hospital).
Two participants’ decisions were influenced by their beliefs, whereby one participant mentioned that she initially declined to consent to surgery because she thought her condition was a result of sorcery and the second participant was worried about blood transfusion because the patient was a Jehovah’s witness.
When I arrived at Nsambya Hospital, the truth is I had refused to be operated upon because I had the mentality that it was witchcraft, but a friend of mine assured me that I must be operated. I later agreed and my wife signed and on that exact day I was taken to the theatre (Patient 12, Private hospital). Concerning the issue of operation, the doctors told me that the patient may lose a lot of blood and may require a blood transfusion but basing on my patient’s beliefs he did not want a blood transfusion and we agreed with the doctors and the doctors said that if a blood transfusion is necessary, we will continue talking on that issue (NOK 19, Public hospital).
One attendant signed as NOK because there was no NOK available even though he felt that he did not have the legal capacity to make decisions on behalf of the patient. He expressed anxiety about taking on the responsibility for whatever was to be done for the patient and the possible outcomes. He reported fear of blame by close family members when the patient’s limb was amputated.
Then I told the doctor that I am not the one supposed to sign for him because the siblings are far from here, the relationship I have with him is very minimal and I have just come here to help him because he has no caretaker. . ., but I said that doctor that I did not want this leg to be amputated when the relatives are not the ones who have signed, they will think I am the one who decided. (NOK 12, Public hospital)
One participant mentioned that they did not have adequate time to decide although the participant had about 2 h to decide, which from the perspective of the patient was inadequate time.
What I didn’t like is that like I was just given about 2, 3 h for surgery to be done, so time was so short (Patient 39, Private hospital)
Discussion
Emergency and critical care in low-income countries in Sub-Saharan Africa like Uganda is a challenge because of inadequate human resources, inaccessibility of health care services due to poor road infrastructure, poorly equipped emergency units and overcrowded health facilities. Healthcare may be financed by the government in the public hospital or by private health insurance or the individual in the private hospital. In spite of government financing health care in the public institution, there are several shortages in the form of drugs and sundries whose costs are met by the patient. Those who have health insurance may seek care at private institutions which are less crowded and better resourced. The above challenges further make decision-making more complex for patients or NOK of patients requiring emergency surgery because, in addition to these challenges, patients and the NOK must make critical decisions for themselves or on behalf of the incapacitated patient in a limited time. The decision-making process involves evaluating the risks and benefits of various treatment options and navigating complex ethical dilemmas by the patients, NOK and healthcare providers while considering the resources available for them to be able to access the required care. It also involves understanding what care needs to be given, and voluntary decision-making without coercion or undue influence. Decision-making during informed consent for emergency surgery for some of the participants in this study was communitarian with the patient at the center but with input from the NOK, other family members and the emergency staff. There was a discussion between the patient or NOK and the healthcare provider to help in the decision-making process.
Decision-making by patients
A patient is said to have decision-making capacity when one can understand, communicate their choice, appreciate risks and benefits and can reason about the various options. 26 Most patients in this study reported that they made a voluntary decision for emergency surgery. Voluntariness in decision-making demonstrates patient autonomy, which is a key component of informed consent and should be accompanied by adequate disclosure of information by the clinician to the patient. In this study, patients felt there was inadequate information given to them which was similar to findings in a study among patients who had undergone elective surgery in the same hospital in which patients perceived that their decision-making capacity was impaired by inadequate information disclosure. 27 Much as the patients in this study had conditions requiring emergency surgery, some of them were able to make decisions personally on their own. In other studies, patients relied on their clinicians to help them make a decision in an emergency setting and sometimes left the decision-making to others like the NOK, or others who had accompanied them to the hospital even when they were competent to make decisions.20,28 Although patients in this study expressed that they had the capacity to understand and the confidence to make decisions for themselves, they did so after consulting with the doctors, their spouses, siblings and other friends. This perception of autonomy by the patient during decision-making could probably be because patients were required to document their consent by signing for themselves.
People consulted and decision-making by NOK
In this study, some patients did not have the capacity to consent and the NOK made decisions on their behalf. This is similar to other studies where the patient does not have the capacity to consent, the NOK or other surrogate decision-makers must make decisions in the best interest of the patient. 2 The NOK in this study were mostly blood relatives or spouses of the patient, and they were pivotal in the decision-making process because they were responsible for ensuring that whatever was done was in the best interest of the patients. However, there were instances where the NOK was not a family member but was a friend or workmate to the patient. There was neither clear definition of who should be a next of kin nor were there standard protocols to guide emergency medical personnel on the identification of the NOK at both hospitals. The NOK in the Western setting is defined according to what role they have to play in making decisions about healthcare, decisions following the death of an individual and sometimes being appointed by the patient prior to the situation. 12 In an emergency setting, the NOK may not be a person appointed prior to the emergency by the patient and is often inadequately prepared for this role. Some of the NOK in this study reluctantly took on this role even though they felt that they did not have the capacity to represent the patient’s best wishes, and this placed a significant emotional burden on them.
There are three hierarchal standards that must be met when decisions for health care are made by a surrogate or NOK. Firstly, the patient’s wishes should be known by the surrogate. Secondly, the decision made should be in the patient’s best interest. Lastly, the surrogate’s decisions align with what the patient would most likely have done. 29 In this study, some of the NOK felt they did not have the capacity to represent the patient’s wishes and consulted with other family members. Some NOK in this study sought a family decision which introduced the concept of family autonomy. In other studies, the concept of family autonomy has been described in some cultures in Asia and the Middle East where culturally, families are integrally involved in decision-making on behalf of a patient and sometimes override the patient’s wishes.30,31 In a study in China, decisions were made by the family and not by a single individual NOK thus demonstrating the concept of family autonomy versus patient autonomy in the decision-making process. 32 Though this study did not explore the influence of culture on decision-making in-depth, it demonstrated the role of the family in the informed consent process in these settings. Some NOK reported that they sought the approval of other family members before deciding whether the patient should undergo emergency surgery. In an emergency setting, it is possible that the family’s autonomy may outweigh the patient’s autonomy, especially when the patient’s wishes are not known a priori. In an analysis of decision-making, Baron noted that autonomy is not absolute and a Utilitarian approach may be considered to discuss the preferences of one principle over another during the decision-making process. 33
Most patients and NOK in this study used a communitarian approach during the decision-making process of informed consent. A communitarian model of decision-making during the consent process is described by Mendel, 34 in which the patient, family and other stakeholders in the patient’s outcome discuss with healthcare providers and own the decisions. It has also been recognized that the decision-making by surrogates or NOK especially for patients whose wishes are not known may be improved if it is a group decision versus individual decision-making. 35 In this study, the participants had more confidence in the decision they made by consulting, and this helped to allay anxiety and stress caused by the probability of making a decision that did not represent the wishes of the patient and the broader family at large. Studies have shown that decision-making during critical emergencies by family members may be hierarchal in nature with a key family member making the decisions even when they are not physically present to provide consent. 36 In this study, the patients and the NOK sought the help of other family members who were considered at a higher hierarchal level like parents, older siblings and spouses of the patient. The Western approach to informed consent is more individualistic, where the focus is on the patient’s autonomy and understanding following a discussion between the patient and the physician, also described as an autonomy-enhancing model. 4 In some African settings informed consent is more communitarian based on socio-cultural norms where authorization of consent is sought by the patient from a community leader or an older member of the clan or family.36,37
Patients and their NOK in this study discussed with the doctors, which aligns with the concept of shared decision-making in which healthcare providers through the patient-physician relationship jointly make decisions on the best treatment options for a patient.6,18,38,39 Patients and NOK in this study appreciated the fact that some doctors took time to explain the need for the emergency procedures acknowledging that this helped them in the decision-making process. In this study, some patients complained that they did not have adequate information disclosure and preferred that more time was given to discuss with the doctor to better understand the care that was being offered. However, sometimes shared decision-making in an emergency may not be feasible because of the time constraints involved in having dialogue with patients and their NOK. 19 There is a need to therefore strike a balance between adequate disclosure and discussion to aid understanding and decision-making by the patients and their NOK during the informed consent process in an emergency, and the limited time required to effect emergency care by the surgeons.
Surrogate decision-makers often face challenges of the pressure to represent a patient’s wishes which might not be known. They may express fear about deciding alone and the repercussions of the decisions that they have made for the patient and the rest of the family members. In such instances, quality communication between the NOK and the healthcare providers is necessary to allay anxiety and give the surrogate decision-makers more confidence that they are making an informed decision that is best for the patient. 40
Documentation of the decision-making process
In this study, some participants signed the consent form merely following the instructions of the doctors or the nurses but, in essence, had not understood the content. This was similar to findings from a study in Australia which showed that patients undergoing emergency surgery were more likely to sign the consent form without considering the content. 41 The consent forms used in the emergency units of the two health institutions are based on the autonomy-enhancing model. Documentation of consent on the instructions of the doctors may be a reflection of the paternalistic doctor-patient relationship where patients feel the doctor knows best and therefore they have to do what he or she tells them to do. In this study documentation of consent in the form of a signature assumed that the patient made the decision individually and did not document the input of other people consulted during the decision-making process. The consent form needs to capture consultations made with other stakeholders and family members thus showing that the communitarian approach was used during the decision-making aspect of informed consent.
Factors influencing decision-making
Although most participants were satisfied with the information they were given, some participants in this study felt that there was inadequate disclosure of information on the risks, benefits and alternative treatment options which affected their decision-making. There was a possibility that some participants made decisions that were not informed but just had to accept to undergo surgery to save lives. Conversely, in this study, participants had more confidence in deciding when they felt that they had adequate disclosure by the doctors. They then decided after discussions with the doctors and asserted that decisions were eventually made by them even though they expressed the view that the doctors knew what was best for the patient. In other studies, shared decision-making in the emergency setting was done with patients, surrogate decision-makers and healthcare providers to ensure that there was adequate disclosure. This enabled them to make the best decision for the patient according to the patient’s wishes and other relevant concerned parties in the community or the extended family.18,38,42
Socio-cultural and religious beliefs influenced decision-making in this study. One participant initially attributed their illness to sorcery and witchcraft and thus could not make an independent decision. He reported that he had to consult other family members and friends before deciding to undergo emergency surgery. Studies have shown that religion and cultural beliefs have an influence on decision-making during the informed consent process.31,43,44 In cultures, where there is belief in traditional medicine as in our setting, many patients initially seek care for their illness from traditional healers because they attribute their illness to a spell that has been cast upon them by their enemies or their ancestors. One of the assumptions in the African theory of personhood is the belief that some of the misfortune or illness that happens to an individual is influenced by ancestors or spirits and one requires spiritual cleansing to get well.45,46 When traditional medicine fails to address their problem, they seek medical care in the hospitals. Therefore, they may still have these ideas about their illness in the background as they decide on their care during informed consent. Cultural leaders might be consulted before they make a decision as has been seen in some Asian and North American populations where cultural beliefs have a significant influence on decision-making during informed consent for medical care and research.47,48 Another participant in this study was influenced by their religious beliefs toward blood transfusion. This is common for patients who are Jehovah’s witness believers and are against blood transfusion. Blood transfusion may be required for emergency surgery and patients have to consent to blood transfusion as part of the emergency surgery they need. Their religious belief then conflicts with their need to get life-saving treatment and influence their decision-making during the informed consent process. The role of religious beliefs in decision-making during informed consent has been recognized and has to be taken into consideration and respected when seeking consent, especially for emergency life-saving medical care.49,50
Another factor that influenced decision-making in this study was the reassurance that the patient or NOK received from the doctors that the patient would recover from their illness. This gave the patient and NOK more confidence and hope that the decision they were making was the right one that would benefit the patient. The patients and the NOK made decisions based on the need to have a good outcome and alleviation of their symptoms. The post-operative outcomes and likelihood of survival from the surgery have been shown to be a major factor that patients and NOK considered during the decision-making process for informed consent for emergency surgery.41,51 It has also been found in studies about surrogate decision-making in emergency and life-threatening situations that the NOK may make decisions based on whether the outcome of the care is going to save the life of the patient even more than the possible consequences of death or disability. 52
Finally, although one participant in this study reported that language used and low literacy level influenced their ability to understand and therefore to decide during the informed consent process, this is similar to other studies which have noted that language is a factor in understanding and decision-making during the informed consent process. 47 The language used by physicians during the informed consent process should not be complex to enable better understanding of the information disclosed to the patient. Informed consent forms should also be written in simple language that a patient of a low literacy level is able to understand. Explanation of the consent form can also improve understanding for patients who are unable to read the consent form.
Strengths of the study
This study was conducted among patients who were undergoing emergency surgery, unlike previous studies which assessed decision-making in an elective setting. Furthermore, the study was conducted in low-resourced emergency units of a low-income country which highlights the challenges of decision-making in such a setting compared to previous studies conducted in high-income better-resourced units. A more in-depth understanding of decision-making and emergent concepts in the decision-making process was captured based on the experiences of the patients and NOK in response to the open-ended semi-structured interviews.
Study limitations
The interview guide we used was not a validated tool but was piloted among nine patients and the NOK of patients who had undergone emergency surgery. This could have resulted in interviewer bias because of leading questions and inability of participants to understand the questions and therefore capture the appropriate relevant information from the participants. Participant feedback was not obtained, and transcripts were not returned to the participants to confirm that the information obtained was accurately captured because this was not feasible since patients and their NOK were not followed up after discharge from the health institutions. The audio recordings were translated from the local language by the PI and the research assistants and transcribed into English. Back translation and reporting findings to the participants were not done hence some information may not have been accurately captured in their context. Inaccuracies in translation were mitigated by the audio recordings being transcribed and reviewed by three authors, an independent reviewer and the research assistants for accuracy of translation.
Conclusion
Decisions were made collaboratively with the patient at the center but with input from health personnel, the NOK and other family members. Decisions made were driven by the need to save the life of the patient. The documentation of consent represents a decision made through a communitarian approach rather than by an individual patient or NOK. The concept of the NOK is not clearly understood in our setting and needs to be clearly defined to aid in the identification of an appropriate representative for the incapacitated patient. A communitarian approach combined with shared decision-making between the doctor and the patient and NOK with adequate discussion and disclosure of information in a simple language would improve decision-making for patients and their NOK.
Best practices
We recommend that healthcare workers should employ a shared decision-making approach during the informed consent process for patients undergoing emergency surgery. Healthcare workers should engage and discuss with the patients as well as the NOK whenever they are available so that decisions are made with adequate disclosure and less strain for all the stakeholders. The aim of this engagement is to ensure that not only are the patient’s best interests considered but also consensus is achieved as much as possible for better decision-making and understanding during the informed consent process. Documentation of the people involved in the decision-making would be useful in confirming the parties involved in this process in case of future litigation or medicolegal challenges.
Research agenda
Further research to identify whether decisions made by the NOK correlate and represent the patient’s interests would help identify how to address these challenges in an emergency setting, especially where the patient’s wishes are not known. The definition of the NOK, their role in an emergency setting and legal implications need to be better defined to consider non-traditional NOK like work colleagues, other caregivers and extended family who are sometimes the only people present to provide consent during an emergency. The role of the healthcare workers in decision-making for incapacitated patients who require emergency surgery and have no NOK needs to be defined and institutional protocols put in place to guide healthcare workers on how to handle this challenge.
Educational implications
Patients need to be educated on the need to have a designated NOK, while the NOK needs to be made aware of their role in representing the patient’s wishes and interests. Healthcare workers ranging from nurses, intern doctors, trainee surgeons and surgeons need to be conversant with the options they have when obtaining informed consent in an emergency setting. Emergency unit healthcare workers should be trained in adequate disclosure and discussion with both the patient and the NOK to promote shared decision-making. Institutions need to provide guidelines on the healthcare worker’s role in emergency consent and identification of the NOK.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241259931 – Supplemental material for A qualitative study on informed consent decision-making at two tertiary hospitals in Uganda: Experiences of patients undergoing emergency surgery and their next of kin
Supplemental material, sj-docx-1-smo-10.1177_20503121241259931 for A qualitative study on informed consent decision-making at two tertiary hospitals in Uganda: Experiences of patients undergoing emergency surgery and their next of kin by Olivia Kituuka, Erisa Sabakaki Mwaka, Ian Guyton Munabi, Moses Galukande and Nelson Sewankambo in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241259931 – Supplemental material for A qualitative study on informed consent decision-making at two tertiary hospitals in Uganda: Experiences of patients undergoing emergency surgery and their next of kin
Supplemental material, sj-docx-2-smo-10.1177_20503121241259931 for A qualitative study on informed consent decision-making at two tertiary hospitals in Uganda: Experiences of patients undergoing emergency surgery and their next of kin by Olivia Kituuka, Erisa Sabakaki Mwaka, Ian Guyton Munabi, Moses Galukande and Nelson Sewankambo in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241259931 – Supplemental material for A qualitative study on informed consent decision-making at two tertiary hospitals in Uganda: Experiences of patients undergoing emergency surgery and their next of kin
Supplemental material, sj-docx-3-smo-10.1177_20503121241259931 for A qualitative study on informed consent decision-making at two tertiary hospitals in Uganda: Experiences of patients undergoing emergency surgery and their next of kin by Olivia Kituuka, Erisa Sabakaki Mwaka, Ian Guyton Munabi, Moses Galukande and Nelson Sewankambo in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge the management and staff of the emergency units of the two tertiary institutions, who enabled the research to be conducted at these institutions. We acknowledge the research assistants who conducted the interviews and audio recorded and transcribed the interviews. We also acknowledge Adeline Tumwijukye (AT) and Andrew Lakica (AL) who independently reviewed the transcribed interviews and coded the responses.
Authors’ contributions
OK designed the study, analyzed the data and drafted the manuscript. IGM designed the study, reviewed and edited the manuscript. ESM designed the study, reviewed and edited the manuscript. NS reviewed and edited the manuscript. MG reviewed and edited the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Research reported in this publication and funding for data collection, data analysis and manuscript writing were supported by the Fogarty International Center of the National Institutes of Health under Award Number D43TW010892 through the Makerere University International Bioethics Research Training Program.
Ethics approval and consent to participate
Ethical approval to conduct the study was obtained from the School of Biomedical Sciences Research and Ethics committee of Makerere University College of Health Sciences reference number SBS 831. Administrative clearance was also obtained from both Mulago National Referral Hospital and Nsambya Hospital.
Consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from all participants in the study these being patients, their next of kin and or their legally authorized representatives.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.