
Abstract
Introduction:
There are high incidence and mortality rates of cervical cancer among females in East Africa. This is exacerbated by limited up-to-date data on premalignant lesions and associated factors in this setting. In this study, we determined the prevalence of cervical intraepithelial lesions and associated factors among women attending the Mbarara Regional Referral Hospital cervical cancer clinic in Southwestern Uganda.
Methods:
In this cross-sectional study, 364 participants were recruited from among women attending the Mbarara Regional Referral Hospital cervical cancer clinic from 1 April to 30 June 2023. On consent, the study nurse collected demographic data and Pap smears, which were microscopically examined and reported by a laboratory scientist and a pathologist following the Bethesda grading system (2014). Statistical analyses were done in STATA version 17, using proportions, Chi-square, bivariate, and multivariate logistic regression analysis to determine associated factors at ⩽0.05 significance level.
Results:
The mean age of participants was 41.9 years. A third of all study participants (37.6%, 132/351) were contraceptive users, mostly hormonal contraceptives (87.1%, 115/132). Almost 88% (307/351) had an unknown Human Papilloma Virus status. The prevalence of cervical intraepithelial lesions among our study participants was 6.6% (23/351), of which 73.9% (17/23) were low-grade squamous intraepithelial lesions. More than half (9/17, 52.9%) of low-grade squamous intraepithelial lesions were active hormonal contraceptive users. Use of hormonal contraceptives (OR: 3.032, p: 0.0253), use of intrauterine devices (OR: 6.284, p: 0.039), and any family history of cervical cancer (OR: 4.144, p: 0.049) were significantly associated with cervical intraepithelial lesions.
Conclusion:
The prevalence of cervical intraepithelial lesions was 6.6%, lower than global estimates. Use of hormonal and intrauterine device contraceptives, as well as family history of cervical cancer, were significantly associated with cervical intraepithelial lesions among our study population. Prospective studies are recommended to further understand associations between different types of intrauterine devices and hormonal contraceptives, and cervical lesions.
Introduction
Globally, cervical cancer is number four among the most common malignancies affecting women. 1 About a million incident cervical cancer cases and 307,000 mortalities were reported in Sub-Saharan Africa in 2020, 2 with low and middle-income countries recording increasing incidence and mortality rates.3,4 Incidence and mortality rates stand at 40.1/100,000 and 28.6/100,000, respectively among females in East Africa. 2 Cervical cancer is, however, ranked as the commonest cancer among women, responsible for death of more women than any other cancer in Sub-Saharan Africa, Asia (including India), as well as some countries in Central and South America. 5 On a similar note, 569,847 incident cases of cervical cancer were reported worldwide in 2018 by Bray et al., 6 with an age-standardised incident rate in East Africa being 40.1 per 100,000. South Africa had the highest age-standardised incidence rate of 43.1 per 100,000. Majority of African countries, including Uganda, have been reported to have an age-standardised incidence rate of at least 40 per 100,000. 1 In 2019, it was reported that 2784.9 million women worldwide aged 15 years and older were at risk of developing cancer of the cervix. 7 The prevalence of cervical precancerous lesions around Africa has been reported to be in the range between 3.7% and 22.6%.8–16 From the Ugandan perspective, Eilu et al. 17 showed that the prevalence of cervical intraepithelial neoplasia stands at 38.6%.
Human papillomavirus (HPV) is a well-established necessary but not sufficient cause of cervical lesions.18,19 Development of cervical cancer occurs through several stages, starting with chronic infection with high-risk HPV (HrHPV) genotypes, through premalignant stages (cervical intraepithelial neoplasia (CIN)), and finally culminates into invasive cervical cancer (ICC).20,21 HPV16 and HPV18 have been implicated to be HrHPV subtypes highly associated with around 70% of all cervical cancers. 22 After a persistent infection with HrHPV genotypes, epithelial cells undergo a series of changes, typically epithelial-mesenchymal transition, 23 turning epithelial cells into mesenchymal cells which can metastasise; a property that is thought to contribute to the metastatic nature of human cancer cells. 24 During the productive stage of infection, the viral genome is relatively maintained at a low number of copies in the basal cells.25–28 The viral episomes remain maintained in basal cells by being replicated alongside the host cell chromosomes.29–31 Thereafter, the viral life cycle goes on along with the differentiation program in keratinocytes and it is dependent on several cellular and viral factors and proteins. 29 Interactions of various viral and cellular pathways involving mainly proteins and other biomolecules like micro RNAs, E6 and E7, contribute towards progression of cervical epithelial cells to a cancerous state. Outgrowth of dysplastic lesions is said to be facilitated by increasing expression of viral oncogenes, E6 and E7, which themselves interact with various proteins that regulate the cell cycle. 31
A number of factors, including HIV infection, age at sexual debut, Chlamydia trachomatis infection, oral contraceptives, smoking, gravidity, use of multiple sexual partners, and other forms of immunosuppression, are associated with cervical cancer.21,32–36 There is limited information regarding the current magnitude of cervical cancer or its premalignant lesions and associated factors in resource-limited settings, which is normally attributed to poor data collection and reporting systems.37,38 Available information 39 is too old to be relied on for decision making. Uganda is experiencing a very low cervical cancer screening rate,40–42 and this might increase the burden due to cervical cancer or its premalignant lesions as a result of late detection and treatment. 43 The low screening rate for cervical cancer is said to be driven by scarcity of knowledge on cervical cancer and its screening services, religious barriers, community misconceptions, fear of embarrassment during screening procedures, fear of screening outcomes, and long distances travelled to reach screening centers among others.44,45 There is still a lot of unknown information regarding prevalence and factors associated with cervical intraepithelial lesions, as well as barriers to screening. This study, therefore, aimed at determining the prevalence of cervical intraepithelial lesions and associated factors among women attending the Mbarara Regional Referral Hospital (MRRH) cervical cancer clinic in South Western Uganda.
Materials and methods
Study design
A cross-sectional study was conducted, including all women who presented at the MRRH cervical cancer clinic from 1 April to 30 June 2023, seeking cervical cancer screening, testing, and treatment services. Results of this study have been reported following the STROBE guidelines for cross-sectional studies.
Study setting
We conducted this study at the MRRH cervical cancer clinic from 1 April to 30 June 2023. MRRH is a public and free access tertiary health facility and is the primary teaching hospital for the medical school of Mbarara University of Science and Technology (MUST); and serves the entire Southwestern Uganda. The distance between MRRH and Kampala, the Ugandan capital, is about 260 km. At this clinic, an average of 15 women are screened for cervical lesions per day, and the clinic runs 5 days a week. Being the only cervical cancer screening and treatment center in the region of Southwestern Uganda, it receives women from all districts of Southwestern Uganda plus the neighbouring countries, including Tanzania, Rwanda, Burundi, and the Democratic Republic of Congo. Staff at the clinic include nurses, midwives, medical officers, and residents, and all are supervised by a gynecologic oncologist. Screening for cervical cancer is voluntary and free of charge, although some women get referred to the clinic by lower health facilities. There is no role played in cervical cancer screening by any insurance service provider. Primary screening tests at the clinic are visual inspection with acetic acid (VIA) and Pap smear cytology, while diagnostic tests include colposcopy and histology. Patients who get diagnosed with cervical lesions either get treatment onsite or get referred to radiotherapy or chemotherapy at the Uganda Cancer Institute. At the clinic, cervical cancer screening services are available to all women aged 21 years and above, following national guidelines. Conventional Pap smear cytology and general histology are performed at the histopathology laboratory in the pathology department of MUST. This laboratory is the regional histopathology laboratory for the Ministry of Health, and it is run by qualified and certified histotechnologists together with pathologists and participates in external quality assurance.
Variables
The main outcome of this study was the prevalence of cervical lesions. The independent variables for this study included age, district, and village of residency, history of blood pressure, diabetes history, marital status, the highest educational level attained, HIV status, smoking status, contraceptive use, type of contraceptive being used, family history of cervical cancer, age at first sexual encounter, total number of lifetime partners, and number of full-term births. For those who reported to be HIV positive, we captured HIV viral load and CD4 count.
Sampling procedure
We used simple random sampling to recruit study participants among all women who sought cervical cancer screening and testing services at the cervical cancer clinic of MRRH. This was adopted to avoid selection bias.
Sample size determination
For this cross-sectional study, the sample size of 364 participants was estimated using the formula by Kish Leslie 1965. For this calculation, we considered d = 0.05, the level of precision which is assumed to be ±0.05, Z(1−α) = 1.96 (Score of normal standard variance curve corresponding to 95% level of confidence) for a two-sided test (1.96); and a prevalence of CIN of 38.6%. 17 Thirteen participants were excluded from data analysis because their Pap smears were non-diagnostic on examination.
Data collection
Upon arrival at the clinic, participants were assessed for eligibility to participate in the study and then after, written informed consent was sought. After the provision of written informed consent, participants were taken through a description of the study and its objectives. Pap smears were then collected, and VIA and other tests were performed thereafter.
Demographic data collection
The midwives from the cervical cancer clinic served as study assistants and administered a pretested questionnaire to gather demographic data. This questionnaire had been used previously35,46 and was pretested at the Uganda Cancer Institute among women seeking cervical cancer care. After the provision of written informed consent, participants were assisted in filling out the questionnaire to capture their demographic data, including age, district, and village of residency, history of blood pressure, diabetes history, marital status, the highest educational level attained, HIV status, smoking status, contraceptive use, type of contraceptive being used, family history of cervical cancer, age at first sexual encounter, total number of lifetime partners, and number of full-term births. For those who were reported to be HIV positive, we captured HIV viral load and CD4 count results from clinic files.
Cytological evaluation
Pap smear collection was performed by midwives at the clinic following a routine standard procedure. The patient was placed on an examination table, and the midwife used a cytobrush or spatula to delicately remove cells from the surface of the cervix while a speculum was gently pushed into the vagina to allow a clear view of the cervix. Smears were created on glass slides, promptly fixed with 95% alcohol, and then stained using the Pap staining technique in accordance with standard operating procedures in laboratories. Smears were examined microscopically by the principal investigator, together with a qualified and certified pathologist. All the examinations and grading followed the Bethesda grading system (2014). 47 The results were categorised as follows: squamous cell carcinoma (SCC), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), atypical squamous cells of undetermined significance (ASCUS), and negative for intraepithelial lesion or malignancy (NILM).
Statistical analysis
Data was collected by the principal investigator with the help of research assistants. It was then entered into an Excel spreadsheet (Microsoft Office Professional Plus 2013, version 15.0.4675.1003, Microsoft Inc, USA) and then imported into STATA 17 (Stata Corp LLC, College Station, TX, USA) software. Descriptive statistics were employed to describe the population using frequencies, means ± standard deviations (SDs), and median values for continuous variables. We also employed Chi-square tests, frequencies, and proportions to describe categorical variables. The prevalence of cervical intraepithelial lesions was presented as proportions. We used bivariate and multivariate logistic regression analysis to arrive at factors associated with cervical lesions. Bivariate analysis was done first, and we purposively selected variables (p < 0.2) for multivariate analysis. We considered a p-value of <0.05 as being significant.
Ethical considerations
Prior to participating in the trial, each subject gave their written informed consent. On all instruments used for gathering data and on laboratory specimens, we used study numbers rather than names. During data analysis, we disconnected all participants’ personal information. All interactions between research assistants and participants happened in a quiet, cosy side room of the clinic that was only available to one person at a time. This study received ethical approval from the Mbarara University of Science and Technology Research Ethics Committee (MUST-REC) (MUST-2022-612) as well as the Uganda National Council for Science and Technology (UNCST) (HS2722ES). We also sought administrative clearance from the MRRH Director before commencing the study. All women whose results indicated a diagnosis of cervical intraepithelial lesions received the standard package of care available at the cervical cancer clinic, and all participants received their Pap smear results.
Eligibility criteria
This study included all women of 21 years and above who reported to the MRRH cervical cancer clinic during the time of the study and provided written informed consent to participate. All women were recruited regardless of their family or personal history of cervical cancer. We excluded all those women who were too ill, as well as those who were undergoing treatment for cervical lesions.
Results
The response rate for this study was 100%, and recruited a total of 364 participants following our inclusion criteria. Thirteen participants were excluded from analysis because they had nonsatisfactory Pap smears, and hence, they were considered to have missing information. We eventually included 351 in the analysis. The mean age of study participants was 41.9 (±12.2). The majority of our participants (63.8%, 224/351) were residing in districts other than Mbarara city, were married (65.2%, 229/351), and were non-smokers (98.3%, 345/351). More than half (58.1%, 204/351) of the study participants were HIV positive, and their mean CD4 count as well as viral load were 493.392 cells per µl and 4719.833 copies per µl, respectively, as shown in Table 1.
Socio-demographic characteristics of study participants at Mbarara Regional Referral Hospital, 1 April to 30 June 2023.

Continuous variables, age, HIV viral load, and CD4 count are presented as mean (standard deviation).
We assessed our study participants for other reproductive characteristics. The most common gynaecological complaint was vaginal discharge, with a prevalence of 12.8% (45/351). More than a third (37.6%, 132/351) were contraceptive users, specifically hormonal contraceptives (87.1%, 115/132). A big proportion (80.3%, 282/351) of our participants reported to have had their sexual debut at an age between 12 and 20 years. Almost 88% (307/351) had an unknown HPV status, while 69.1% (242/351) reported to have had multiple sexual partners, as shown in Table 2.
Reproductive characteristics of study participants at Mbarara Regional Referral Hospital, 1 April to 30 June 2023.

All data was categorical, and the total number of participants was 351, except for type of contraceptive (N = 132).
Prevalence of cervical lesions
We observed a total number of 23 participants with positive cytology results out of 351 participants. These participants were LSIL+, 24 and one participant who was ASCUS but got treatment following an earlier positive VIA test. This makes a prevalence of 6.6%. More than half (73.9%, 17/23) of all positive cases were LSILs. All participants (23/23) with positive Pap smears reported no history of high blood pressure. A good number of participants (19/23) with cervical lesions were married: 100% for ASCUS, 80% for HSIL, and 82.4% for LSIL. More than half (52.9%, 9/17) of participants with LSIL had attained a maximum of primary school education. The same proportion of participants (52.9%, 9/17) were HIV positive and had suppressed viral load, as shown in Table 3.
Prevalence of cervical lesions across selected socio-demographic characteristics of study participants at Mbarara Regional Referral Hospital, 1 April to 30 June 2023.
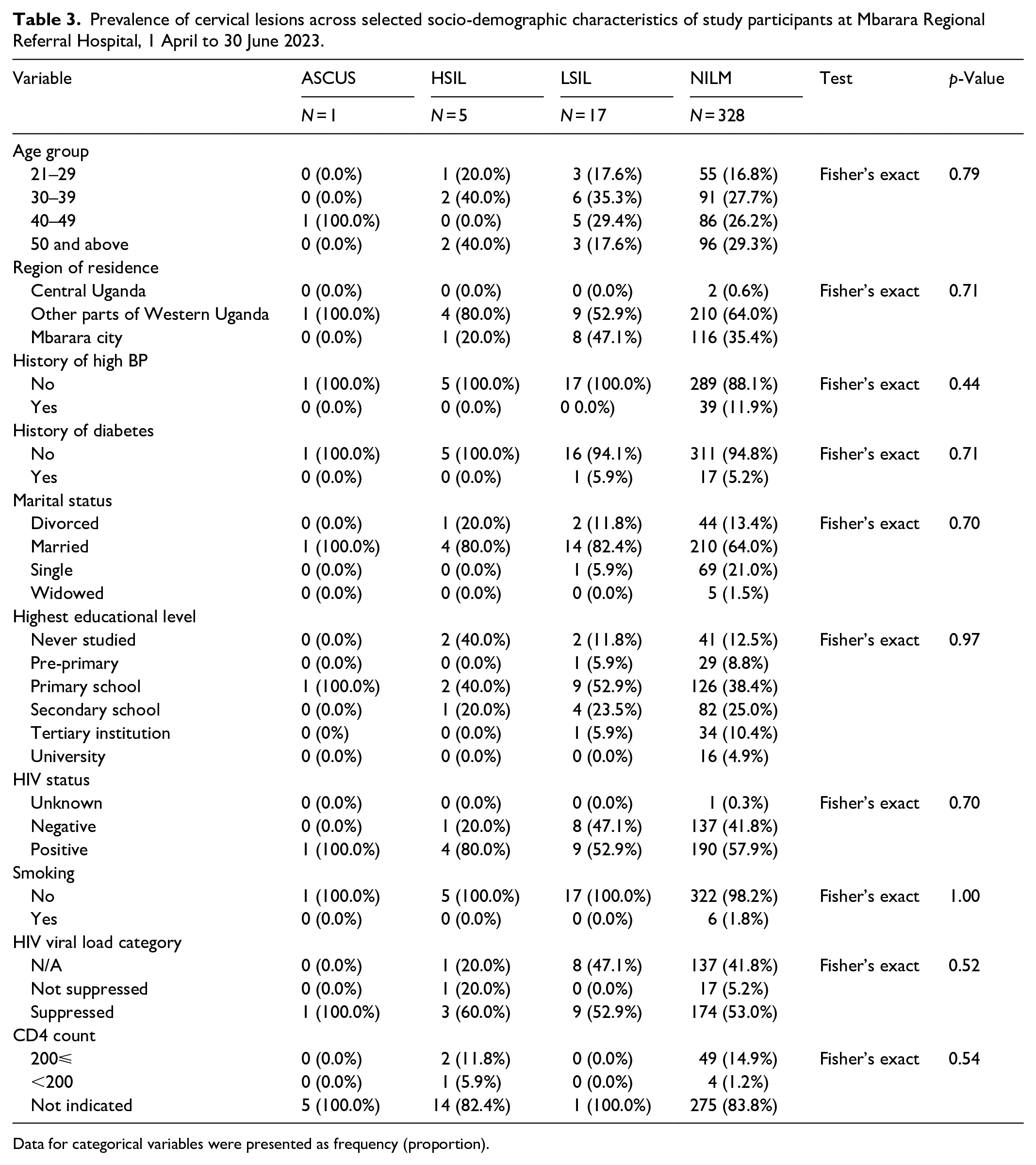
Data for categorical variables were presented as frequency (proportion).
Of all participants who had LSIL, 82.4% (14/17) reported to have had their sexual debut at 31 years and above. Still, for those with LSIL, more than half (58.8%, 10/17) were active contraceptive users, especially hormonal contraceptives (52.9%, 9/17). Additionally, whereas 60% (3/5) of people with HSIL reported having two or more lifetime sexual partners, more than half (70.69%, 12/17) of participants with LSIL did the same. A big proportion of participants (80%, 4/5) with HSIL reported to have had 4 or more full-term births, as shown in Table 4.
Prevalence of cervical lesions across reproductive characteristics of study participants at Mbarara Regional Referral Hospital, 1 April to 30 June 2023.

Data for categorical variables were presented as frequency (proportion).
Factors associated with cervical lesions
Several variables were considered for multivariate analysis after their bivariate analysis revealed p values of less than 0.2, as well as being biologically plausible in cervical cancer. These variables included the number of full-term births, lifetime sexual partners, age at sexual debut, HIV status, type of contraceptive used, family history of cervical cancer, and highest educational level. After adjusting for number of full-term births, type of contraceptive used, HIV status, age at sexual debut, CD4 counts, HIV viral load, highest educational level, and number of life-time sexual partners, the results of the multivariate analysis showed that the likelihood of cervical lesions was three times higher in those who reported using hormonal contraceptives than in those who had not used any form of birth control. This difference was statistically significant (OR: 3.032, p-value = 0.025, 95% CI: 1.150–7.989). Also, participants who reported to have used IUDs as contraceptives were six times more likely to develop cervical lesions compared to those who had not used any contraceptive, and this observation was also statistically significant (OR: 6.284, p-value = 0.039, 95% CI: 1.094–36.095). Participants who reported a family history of cervical cancer were also four times more likely to have cervical lesions than those who reported not to have such a family history of cervical cancer. This observation was statistically significant (OR: 4.144, p-value = 0.049, 95% CI: 1.004–17.101), as shown in Table 5.
Logistic regression analysis showing association between cervical lesions and selected variables of study participants at Mbarara Regional Referral Hospital, 1 April to 30 June 2023.

Data were adjusted for number of full-term births, type of contraceptive used, HIV status, age at sexual debut, CD4 counts, HIV viral load, educational level, and number of life-time sexual partners.
COR: crude odds ratio; AOR: adjusted odds ratio; 95% CI: 95% confidence interval.
Statistically significant (p ⩽ 0.05).
Discussion
In this study, we found that 6.6% of all participants recruited were positive for cervical lesions. This prevalence was lower than is reported in most studies. Studies in other low-resource African countries have reported higher prevalence rates, such as 26.7-37% in Kenya. 48 There was a reported prevalence of 18.2% in Bangladesh 49 and 22.1% in Ethiopia. 50 Previous studies that have been conducted among HIV-positive and negative populations have reported prevalence rates of 22.9% and 5.79%, respectively, in Swaziland. 51 This difference could be attributed to the fact that most of these studies were conducted among HIV-positive people, bearing in mind that HIV is a risk factor for cervical lesions.52–54 However, other studies in Cameroon have reported lower prevalence rates of 3.33%. 55 A case-control study in Nigeria documented a slightly higher but comparable prevalence of abnormal Pap cytology results (8.0%). 56 This observation could be attributed to the comparability of study populations in terms of socioeconomic status and sexual behaviour. Increased prevalence of cervical neoplasia in our study was found among participants who were married and less educated (primary education). This pattern of prevalence was earlier reported in similar studies by Bayo et al. 57 in Mali and Palacio-Mejía et al. 58 in Mexico. These women may have developed cervical neoplasia as a result of their early sexual experience and multiple sexual partners, both of which are significant risk factors for HPV infection.
We found that all participants (23/23) with positive Pap smears reported no history of high blood pressure. This is in agreement with other studies, which have shown that cervical lesions are significantly associated with other metabolic syndrome components except high blood pressure.59–64 It would be imperative to think of an indirect link between high blood pressure and cervical lesions. For instance, from our recent studies in Ugandan populations, we also observed significant associations between other metabolic syndrome components with cervical lesions.36,46 Besides, high blood pressure being associated with inflammation likely impairs one’s immune system, 65 which would eventually predispose one to reduced ability to clear infections, including HPV.
This study presents a higher prevalence of cervical lesions among married women. This contradicts the commonly perceived notion about marriage as a protective factor against cervical lesions 66 and that single women are at increased risk of cervical cancer. 67 This indicates that married women in this study population are likely exposed to HPV or other risk factors for cervical cancer. In fact, population dynamics and trends indicate that 8.3% of all women in Uganda are married or cohabiting in polygamous relationships. 68 Such observations in this population could explain the increased prevalence of sexually transmitted infections, including Chlamydia Trachomatis and HPV, which are associated with cervical lesions. 35 However, an equally high prevalence of cervical lesions among married women was reported in a hospital population in Cameroon. 69
We found out that usage of IUDs and hormonal contraceptives, as well as having a family history of cervical cancer, were significantly associated with cervical lesions in this study population. Although it deviates from many of the risk factors that have been widely accepted, this provides new information regarding risk factors for cervical intraepithelial lesions. For instance, many authors from previous studies reported smoking, HIV positivity, contraceptive use, and a family history of cervical cancer as possible risk factors for cervical cancer.7,52,53,70–78 Furthermore, in a study on the risk factors for cervical neoplasia, Kjellberg et al. 41 discovered a substantial correlation between higher grades of CIN and HPV, smoking, and prolonged contraceptive usage. In addition, our previous study showed that obesity is significantly associated with cervical intraepithelial lesions. 79 For family history of cervical cancer, it is crucial to acknowledge the role of genetic and epigenetic factors in cervical carcinogenesis. For instance, the apolipoprotein B mRNA editing enzyme catalytic polypeptide like DNA-editing protein is said to play an important role in molecular pathogenesis of cervical cancer as well as other cancers.80–82
We observed no association between smoking and cervical lesions. This could be explained by the fact that there were very few cases of smokers in the study population. In fact, smoking has been found not to be associated with any grade of cervical lesions, as evidenced in previous studies by Castellsagué et al. 83 However, smoking has been shown to be associated with cervical precancerous lesions.69,84 and other malignancies.85–87 In our population, age was not associated with cervical lesions, though it was earlier proposed by Bhatla et al. 88 that the age group of 21–40 years could be a risk factor based on the high prevalence of HPV and other factors in the same age group.
We found that usage of IUDs is significantly associated with cervical lesions among the study population. Previous studies have reported contradicting results in regard to IUDs and cervical lesions.89–92 A systematic review by Cortessis et al. 93 reported that cervical cancer is less frequent in women who have used IUDs, and hence, IUDs may be apparently protective against cervical lesions. This protective nature of IUDs against cervical lesions is based on observations that IUDs reduce HPV infection risk and also trigger immune system responses that tend to fight viral infections, including HPV. 94 From the case-control study, nested within the European Prospective Investigation into Cancer and Nutrition (EPIC) Study, non-significantly decreased risk of both CIN3/CIS and ICC was observed among IUD users. 73
However, in agreement with our findings, recent evidence from a case-control study by Averbach et al. 95 showed that IUD usage is associated with CIN2+ but not with CIN3+ In some populations, including those in less developed countries, usage of IUDs is thought to increase the risk of sexually transmitted infections (STIs), including HPV, whose association with cancer of the cervix is well known. 96 A study among Kenyan sex workers found that usage of IUDs was significantly associated with increased incident C. trachomatis infection. 97 This is in agreement with our earlier study, which demonstrated that a co-infection of C. trachomatis and HPV is associated with cervical lesions. 35 Certain types of IUDs, including LNG-IUS, which may not be popular in our study population, have been shown to increase HPV acquisition and persistence. 98 Lekovich et al.’s 99 comparative study, which examined the differences in cervical cytology and high-risk human papillomavirus (HPV) infection clearance between levonorgestrel- and copper-containing IUD users, also supported the findings of our study by showing that levonorgestrel-containing IUDs may be linked to higher risk of high-risk HPV infection acquisition and lower clearance when compared to copper-containing IUDs.
We found a significant association between cervical lesions and usage of hormonal contraceptives. This is in agreement with results from a systematic review by Deese et al., 100 who provided evidence that is supportive of an increased risk of many other STIs, including HSV-2 infection among users of other contraceptive methods, depot medroxyprogesterone acetate (DMPA). Iversen et al.’s 101 reported observations have also demonstrated that the risk of cervical cancer remains strongly correlated with the use of currently available contraceptives, particularly for women who have not received the HPV vaccine. We note that HPV vaccination among our study participants has a very low coverage.102,103 Moreover, with a low cervical cancer screening uptake.41,42 The usage duration of hormonal contraceptives could also have a significant correlation with cervical lesions. To further understand the potential impact of the usage duration of hormonal contraceptives on cervical lesions, a case-control study by Kusmiyati et al. 104 revealed that exposure to hormonal contraceptives for more than 5 years can increase one’s risk of cervical cancer by 4.2 times.
It is well known that hormonal contraceptives change the way cells metabolise their substances, which can lead to long-term HPV infections and the eventual development of cervical cancer. The expression of the oncogenes E6 and E7 of HrHPV genotypes may be encouraged by oestrogen and progestin. This process triggers the destruction of the p53 tumour suppressor gene and the incorporation of viral DNA, resulting in cellular transformation and the development of cancer.105–107 Hormonal contraceptives are also known to bind to certain HPV-DNA sequences within transcriptional regulatory areas, which may control cellular death and promote HPV-DNA integration into the host cell genome.108–114 With increased availability and usage of hormonal contraceptives in our population, there is an increased risk of cervical cancer as a result of hormonal contraception in a predominantly unvaccinated population.102,103 This is based on recent observations that hormonal contraceptive use is also associated with a number of STIs, including HIV, HPV, and Chlamydia Trachomatis, 115 which are known risk factors for cervical lesions.
Recent evidence from a review by Anastasiou et al. 116 showed no evidence of an association between hormonal contraceptive use and cervical lesions. However, this study was limited by sample size that is, very few included studies. Additionally, case-control research conducted in Nigeria by Ajah et al. 56 had previously found no link between cervical neoplasia and hormonal contraception. This study did not reveal any significant association between oral contraceptive use and cervical cancer or any grade of cervical lesion. On the contrary, a recent systematic review has shown that longer duration of oral contraceptive pills use has an associated risk for developing cervical cancer, especially for Adenocarcinoma. 117
Our study is limited by the inherent weaknesses of a cross-sectional study. This design is non-ideal for studying associations between population variables. Therefore, associations presented here may not be easily extrapolated to the wider population. We also acknowledge that classic Pap smear testing could have lowered the diagnostic power compared to liquid cytology. Another limitation of this study is that we only included women who visited the cervical cancer clinic. This could have caused a selection bias. However, the major strength of this study is its statistical power, which we considered while calculating the sample size. We also employed standard methods during collection, processing, examining, and reporting methods for Pap smear specimens. The results of our study could be generalised to the entire Ugandan population as well as other populations in resource-limited countries. This is so, considering the fact that screening uptake rates are said to be between 30.3% 41 and 44%, 42 with a low HPV vaccine completion rate of 43.3%. 102
Conclusion
Based on Pap smear cytology, the prevalence of cervical intraepithelial lesions was 6.6%, which was lower than global estimates. Use of hormonal and IUD contraceptives, as well as family history of cervical cancer, showed significant associations with cervical intraepithelial lesions among our study population. Prospective studies are recommended to further understand associations between different types of IUDs, hormonal contraceptives, and cervical lesions.
Policy implications
The current burden of cervical lesions indicates the need to develop and maintain a national cervical cancer program and to put in place efforts that increase cervical cancer screening towards the World Health Organization targets.
Supplemental Material
sj-doc-1-smo-10.1177_20503121241252265 – Supplemental material for Prevalence of cervical intraepithelial lesions and associated factors among women attending a cervical cancer clinic in Western Uganda; results based on Pap smear cytology
Supplemental material, sj-doc-1-smo-10.1177_20503121241252265 for Prevalence of cervical intraepithelial lesions and associated factors among women attending a cervical cancer clinic in Western Uganda; results based on Pap smear cytology by Frank Ssedyabane, Nixon Niyonzima, Josephine Nambi Najjuma, Abraham Birungi, Raymond Atwine, Deusdedit Tusubira, Thomas C Randall, Cesar M Castro, Hakho Lee and Joseph Ngonzi in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241252265 – Supplemental material for Prevalence of cervical intraepithelial lesions and associated factors among women attending a cervical cancer clinic in Western Uganda; results based on Pap smear cytology
Supplemental material, sj-docx-2-smo-10.1177_20503121241252265 for Prevalence of cervical intraepithelial lesions and associated factors among women attending a cervical cancer clinic in Western Uganda; results based on Pap smear cytology by Frank Ssedyabane, Nixon Niyonzima, Josephine Nambi Najjuma, Abraham Birungi, Raymond Atwine, Deusdedit Tusubira, Thomas C Randall, Cesar M Castro, Hakho Lee and Joseph Ngonzi in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241252265 – Supplemental material for Prevalence of cervical intraepithelial lesions and associated factors among women attending a cervical cancer clinic in Western Uganda; results based on Pap smear cytology
Supplemental material, sj-docx-3-smo-10.1177_20503121241252265 for Prevalence of cervical intraepithelial lesions and associated factors among women attending a cervical cancer clinic in Western Uganda; results based on Pap smear cytology by Frank Ssedyabane, Nixon Niyonzima, Josephine Nambi Najjuma, Abraham Birungi, Raymond Atwine, Deusdedit Tusubira, Thomas C Randall, Cesar M Castro, Hakho Lee and Joseph Ngonzi in SAGE Open Medicine
Footnotes
Acknowledgements
We acknowledge our study participants, the nurses, midwives, and clinicians of Mbarara Regional Referral Hospital, especially the cervical cancer screening and prevention clinic.
Author contribution
The corresponding author, FS, conceived the idea and developed the first draft of the manuscript. Co-authors TCR, DT, NN, and JN supervised the whole project, from data collection to analysis, and reviewed the manuscript. HL and CMC reviewed and provided overall guidance in the entire write-up and approved the final version prior to submission. JNN, RA, and AB participated in data analysis. All authors reviewed and approved the final version of the manuscript. All authors are accountable for all aspects of this manuscript.
Availability of data and materials
All the data from which this article was generated is available from the corresponding author upon meaningful request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was carried out at the clinic, which is supported in part by the National Institutes of Health, under grant number 1U01CA279858. This grant supported cervical cancer screening tests for all women at the clinic, including some study participants.
Ethics approval
Ethical approval for this study was obtained from Mbarara University of Science and Technology Research Ethics Committee (MUST-2022-612) and Uganda National Council for Science and Technology (HS2722ES). We also sought administrative clearance from the Hospital Director, Mbarara Regional Referral Hospital, before commencement of the study.
Informed consent
Written informed consent was obtained from all subjects before the study.
Consent for publication
Not applicable.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.