
Abstract
Introduction:
Cervical cancer is one of the severest risks to women’s life. It is the main reason for more than half million of morbidity and 266,000 deaths worldwide annually.
Objective:
The aim of this study was to assess the level of cervical cancer screening service utilization and associated factors among women of the reproductive age group coming for health care service to public health facilities of Ilu Abba Bor zone, southwestern Ethiopia, 2019.
Methods:
An institutional-based cross-sectional study design was employed from 1 May to 30 May 2019. Participants were selected by systematic random sampling technique. Data were collected using a pretested questionnaire and entered into Epi data 3.1 and exported to SPSS version 23 for analysis. Multivariable logistic regression was used to observe the factors associated with cervical cancer screening utilization service. An adjusted odds ratio with a 95% confidence interval was used. Variables with a p-value of <0.05 were considered to be statistically significant.
Results:
From a total of 259 women involved in the study, about 19 (7.3%) of the study participants had been screened for cervical cancer at least once in the past 3 years during the study period. Educational status: primary (grade 1–8) (adjusted odds ratio = 3; 95% confidence interval = (1.15–7.91)), secondary (grade 9–12) (adjusted odds ratio = 4.21; 95% confidence interval = (1.04–7.46)), and tertiary (grade 12+) (adjusted odds ratio = 6.01; 95% confidence interval = (3.01–11.35)), nulliparous (adjusted odds ratio = 0.256; 95% confidence interval = (0.105–0.642)), and looking for information about cervical cancer (adjusted odds ratio = 3.4; 95% confidence interval = (1.8–6.2)) were significant factors associated with utilization of cervical cancer screening service.
Conclusion:
The study revealed that there was low cervical cancer screening service utilization in the study area. Educational status, parity, and looking for cervical cancer information were independently associated with cervical cancer screening utilization service. There is need to improve women’s education, dissemination of information about importance of cervical cancer screening, and focus on nulliparous women to have good practice of cervical cancer screening.
Introduction
Cancer is a disease which is characterized by uncontrolled cell proliferation in the body. Cervical cancer refers to cancer that begins in the cervix. Seventy percent of cervical cancer cases worldwide are caused by two types of human papillomaviruses (HPV): HPV-16 and HPV-18. 1 Cervical cancer is one of the most serious threats to women’s health, accounting for more than half a million cases of morbidity and 266,000 deaths globally each year. Most of the problems (85%) occur in low-income countries around the world. 2
Cervical cancer screening has been recognized to be a very effective prevention strategy for cervical cancer. The recommendations of the United States Preventive Services Task Force (USPSTF), American Cancer Society (ACS), and World Health Organization (WHO) point out that cervical cancer screening once in a lifetime can significantly reduce the risk of death from the disease and the incidence of advanced cervical cancer. 3
Despite government support for health policy, women in underdeveloped nations have a lower rate of cervical cancer screening than those in developed countries: for example, Kampala, Uganda 7%, 4 Bhutan 6%, 5 and Nigeria 8.3%, 6 respectively. Surprisingly, only 1% of Ethiopian women receive cervical cancer screening, with 90% of women receiving no screening at all. 7
More than 80% of cervical cancer identified with advanced stage in low-income countries, resulting in low survival rates after surgery or radiotherapy. WHO investigated and reported a cervical cancer screening technique called visual inspection with acetic acid (VIA) in order to help Ethiopia and other resource-poor countries. 8 In low-income countries, using VIA for simultaneous diagnosis and treatment in a single visit is an effective prevention technique that can reduce complications and mortality. 9
The WHO indicated that the number of health institutions in Ethiopia that provide cervical cancer screening are very low, and it is expected to be used by women greater than 30 years old and women at risk to acquire cervical cancer, such as women with multiple sexual partners, smoking, begin sexual intercourse earlier, have HIV, and other sexually transmitted infections (STIs). 10
According to the Black Lion Specialized Hospital’s Oncology Center, Ethiopia, the majority of cancer cases are diagnosed at a late stage. Treatment options for this condition are limited at this time. This is mainly due to a lack of screening service, early detection and treatment services, as well as inadequate diagnostic facilities and poorly structured referral system. 11
Study conducted in Dire Dawa Ethiopia revealed that age > 40 years, attending private health institutions, occupation, visiting gynecology ward, having good knowledge about cervical cancer screening, counseling from health professionals, and using family planning methods were determinant factors of CC screening uptake. 12 Another study conducted in Arba Minch Ethiopia showed that only 9.6% women have had cervical cancer screening within the past 3 years. There was association between CC screening awareness and utilization of CC screening service. 13
According to studies conducted in Bahir Dar, Saint Paul’s Teaching Hospital, and Bishoftu, the rural residence, low monthly income, history of STIs, frequent health facility visits, providers’ recommendation, and poor knowledge about CC screening were determinants of cervical cancer screening service utilization.14–17 The study conducted in Northern and southwestern Ethiopia also identified that level of education, lack of awareness about CC screening, occupation, having children, and visiting health facilities were the determinant factors associated with the uptaking of cervical cancer screening.18,19
Regular and early screening and treatment as part of targeted interventions is mandatory to reduce the incidence and mortality associated with the cervical cancer. But there are very limited studies conducted in the country, specifically in the study area to assess the utilization of cervical cancer screening service. The aim of this study was to assess the level of cervical cancer screening service utilization and associated factors among women of the reproductive age group coming for health care service to public health facilities of Ilu Abba Bor zone, southwestern Ethiopia, 2019.
Methods
Study setting and period
The study was implemented in Ilu Abba Bor zone, Oromia regional state from 1 May to 30 May 2019. There are 12 districts in the zone and based on the 2007 census conducted by the Central Statistical Agency of Ethiopia, the zone has a total population of 1,271,609 from which 44,124 (3.47%) were females of the reproductive age group. The capital town of the zone is Mettu, located in the southwestern of Ethiopia at 600 km from Addis Ababa. In the zone, there were 20 health centers and 2 public hospitals giving the health services. The study was done at 12 health centers and 1 hospital (Mettu Karl referral hospital). Mettu Karl referral hospital was the only health facility providing cervical cancer screening service using VIA for women of the reproductive age group who were referred from other health institutions and at high risk to develop cervical cancer.
Study design
An institutional-based cross-sectional study design was implemented.
Source Population
All women of the reproductive age group who visited public health facilities of Ilu Abba Bor zone for health care services were the source population.
Study population
All sampled women of the reproductive age group who visited the selected public health facilities of Ilu Abba Bor zone for health care services during the data collection period were the study population.
Inclusion criteria
The women of reproductive age who visited selected public health facilities for health care services such as antenatal care (ANC), family planning, gynecological care, and adult outpatient departments for medical care during the data collection period were included.
Exclusion criteria
Those women who were critically ill and unable to respond for the required information were excluded from the study.
Sample size determination
Single population proportion formula was used to estimate the sample size required for this study with the following assumptions: P = 19.8%, taken from the study conducted in Mekelle 8 (which revealed the prevalence of cervical cancer screening utilization service was 19.8%), at the marginal error of 5% with a 95% confidence level. Accordingly, the sample size was 244 and by considering 10% of calculated sample size for non-respondents, the final sample size was 268.
Sampling technique and procedures
Twelve health centers and one public Hospital, namely Hurrumu, Yayo, Gore, Mettu, Nopa, Becho, Darimu, Uka, Bure, Sibo, Burusa and Alge health centers, and Metu Karl Referral Hospital, were selected randomly by using the lottery method. The final sample size was proportionally allocated for each facility based on 3-month average client flow. Finally, we selected the participants using a systematic random sampling technique after calculating K-interval for each facility until we got the proportionally allocated sample size.
Study variables
Outcome variable. Utilization of cervical cancer screening service measured by asking the respondent’s action toward screening for a premalignant cervical lesion in the past 3 years. Those who ever screened at least once within the past 3 years were regarded as utilized cervical cancer screening service and those who had never screened in the past 3 years were regarded as having not utilized cervical cancer screening service. 2
Independent variables. Age, marital status, religion, ethnicity, participant’s educational status, husband’s educational status, monthly family income, parity, participant’s occupation, source of information, and knowledge about cervical cancer.
Data collection tools and procedures
The data were collected by four female Midwives under the Supervision of investigators using a pretested structured questionnaire. The questionnaire was written in English first, translated into Afaan Oromoo and then back to English to ensure consistency. The Afaan Oromoo version of the questionnaire was pretested on 5% of women seeking health care at unselected facilities. The data collectors were given 2 days of training on the data collection technique, as well as the study’s aim and objectives. The exit interview took place in a separate area set aside for this purpose near each health facility’s waiting room.
Operational definitions
Cervical cancer screening service utilization. Women who are eligible for cervical cancer screening and have ever been screened for cervical cancer during the last 3 years.
Cervical cancer screening. Application of acetic acid to detect cervical tissue abnormalities in an asymptomatic population.
Good knowledge about cervical cancer screening. The women who scored greater than the mean of knowledge measuring questions (9 questions).
Poor knowledge about cervical cancer screening. The women who scored less than the mean of knowledge measuring questions (9 questions).
Statistical analysis
The Epi data 3.1 and SPSS version 23 were used for data analysis. Multivariable logistic regression was used to assess the relative effect of independent variables on the dependent variable to control the possible confounders and to select significant predictors of utilization of cervical cancer screening included in the final model. Finally, the adjusted odds ratio (AOR) with its 95% confidence interval (CI) and a p-value of 0.05 was used to identify significant associated factors of cervical cancer screening service utilization. The findings were presented using text and tables.
Ethical approval
Ethical approval was obtained from Mettu University Research and Ethical Committee with the approval number of MU/67/566/19. The permission letter was provided from Ilu Abba Bor zonal Health Office, and other concerned bodies in the study area. During data collection, each respondent was informed about the purpose, scope, and expected outcome of the research. Informed written consent was obtained from each subject and legally authorized representatives of the subjects who were minors before proceeding data collection.
Results
Socio-demographic characteristics of the study participants in public health facilities of Ilu Abba Bor zone, southwest Ethiopia, 2019
Out of the total 268 participants included in this study, 259 completed the interview making a response rate of 96.6%. The mean age of the study subjects was found to be 27.34 years with a standard deviation, SD ± 6.17 and ranged from 17 to 40 years. Most of the respondents (60.6%, n = 157) were currently married. The highest grade completed by the respondents was primary education (1–8) (40.5%, n = 105) and informal education (19.7%, n = 51) (see Table 1).
Socio-demographic characteristics of the study participants in public health facilities of Ilu Abba Bor zone, Southwest Ethiopia, 2019.

Wolayita, Sidama, and Afar.
House wife, private, shopkeeper.
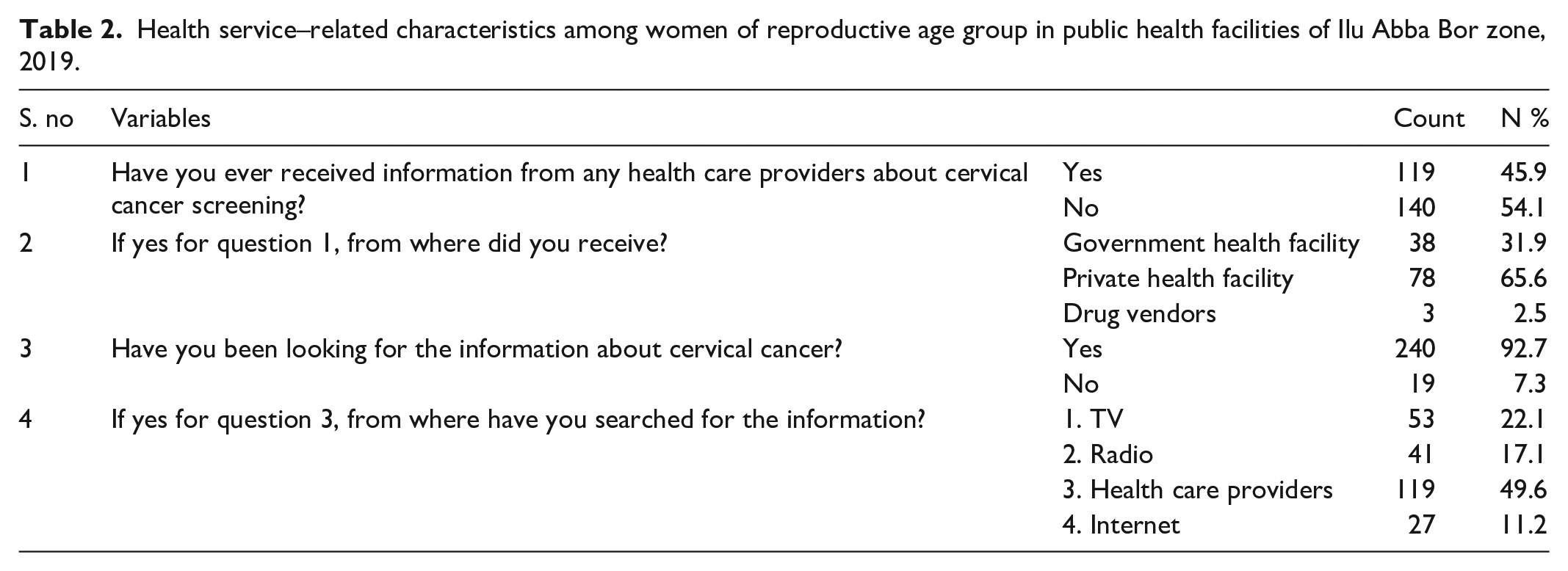
Health service–related characteristics among women of reproductive age group in public health facilities of Ilu Abba Bor zone, 2019
The result of this study indicated that more than half (54.1%, n = 140) of the respondents never received information from any health care providers about cervical cancer screening. The private health facility takes the major (65.6%, n = 78) part to be the source of information. Almost all (92.7%, n = 240) of the study participants have been looking for the information about cervical cancer and nearly half (49.6%, n = 119) of them searched for the information from health care providers (see Table 2).
Health service–related characteristics among women of reproductive age group in public health facilities of Ilu Abba Bor zone, 2019.
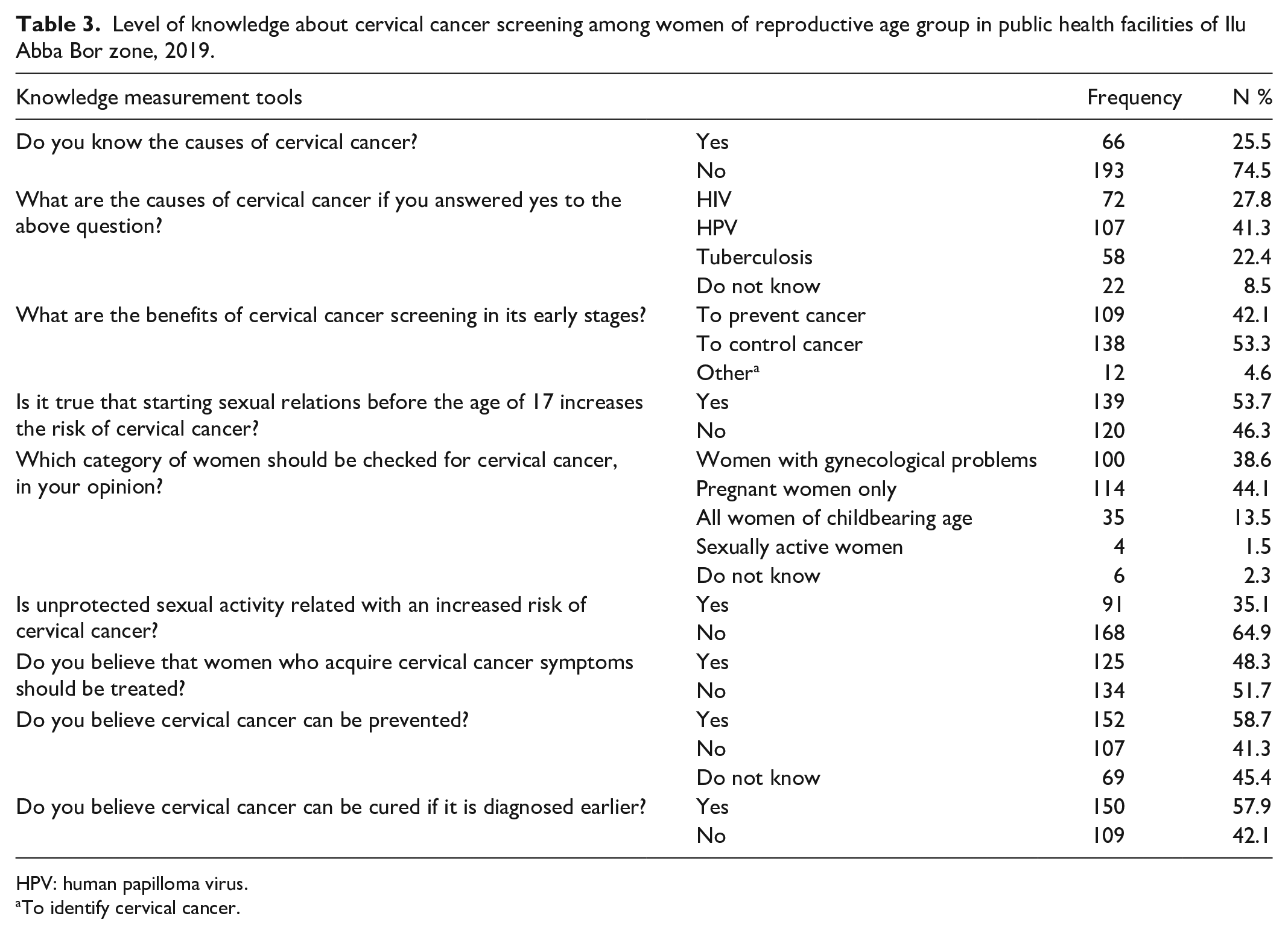
Level of knowledge about cervical cancer screening services among women of reproductive age group in public health facilities of Ilu Abba Bor zone, 2019
About 124 (47.9%) of the respondents (95% CI, 4.21–5.37) had poor knowledge, meaning they scored less than the mean of knowledge measuring scores (4.32; SD = 1.75) and the minimum and maximum knowledge scores were 0 and 9, respectively. Nearly three-quarters of respondents (74.5%, n = 193) were unaware of the causes of cervical cancer. The HPV was the most (41.3%, n = 107) often stated cause of cervical cancer. One hundred nine of study participants (42.1%, n = 109) said that early cervical cancer screening is useful in preventing the disease.
The majority of the study participants (53.7%, n = 139) stated that beginning of sexual relations before age of 17 increased the risk of having cervical cancer for women. Only 13.5% of study participants mentioned that cervical cancer screening is important for women of childbearing age (see Table 3).
Level of knowledge about cervical cancer screening among women of reproductive age group in public health facilities of Ilu Abba Bor zone, 2019.
HPV: human papilloma virus.
To identify cervical cancer.
Utilization of cervical cancer screening among reproductive age women coming to public health facilities of Ilu Abba Bor zone, 2019
According to this study, only 7.3% (n = 19, 95% CI (4.2–10.4)) of cervical cancer screening services were used in the previous 3 years. The main reasons for not being screened for cervical cancer were a lack of availability of the service (54.1%; n = 129) and cost issues (24.3%; n = 58). Other reasons given were not knowing where to acquire the service (14.4%; n = 34), fear of discrimination (3.6%; n = 9), and others (see Table 4).
Utilization of cervical cancer screening among reproductive age women coming to public health facilities of Ilu Abba Bor zone, 2019.

Fear of test result.
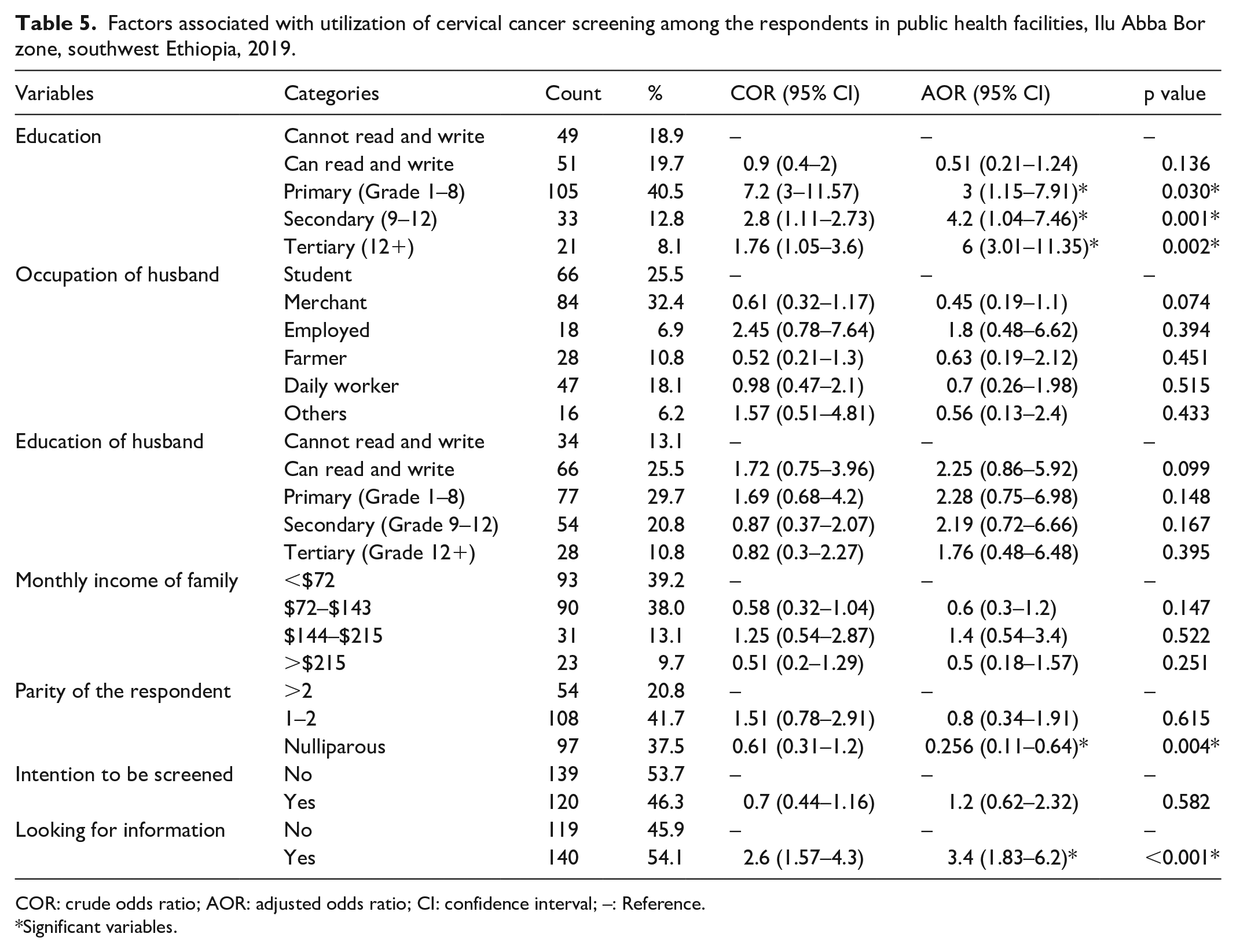
Factors associated with utilization of cervical cancer screening service
Women’s educational status, primary (grade 1–8), secondary (grade 9–12), and tertiary (grade 12+) level of education were 3 times (AOR = 3; 95% CI (1.15–7.91)), 4.2 times (AOR = 4.21; 95% CI (1.04–7.46)), and 6 times (AOR = 6.01; 95% CI (3.01–11.35)) more likely to utilize cervical cancer screening service than women who cannot read and write, respectively. In addition, respondents who were nulliparous were 74.4% (AOR = 0.26; 95% CI (0.105–0.642)) less likely to utilize cervical cancer screening service than women of parity more than two. The odds of utilization of cervical cancer screening was about 3.4 times more among women who were looking for cervical cancer information than their counterparts (AOR = 3.4; 95% CI (1.8–6.2)) (see Table 5).
Factors associated with utilization of cervical cancer screening among the respondents in public health facilities, Ilu Abba Bor zone, southwest Ethiopia, 2019.
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval; –: Reference.
Significant variables.
Discussion
The aim of this study was to assess the level of cervical cancer screening service utilization and associated factors among women of the reproductive age group coming for health care service to public health facilities of Ilu Abba Bor zone, southwestern Ethiopia, 2019. Therefore, the study found that only 7.3% of women had received cervical cancer screening service at least once in the past 3 years. Factors such as education level, parity, and finding information about cervical cancer screening are significantly related to the use of cervical cancer screening.
The finding of cervical cancer screening service use (7.3%) in the current study was in line with the studies carried out in Debre Merkos (5.4%), 3 Arba Minchi (5.9%), 10 Bishoftu (5.8%), 16 and Ghana (7.8%) 20 of participants who had been screened for cervical cancer, respectively. Correspondingly, studies conducted in Kampala, Uganda (7%) 4 and Nigeria (8.3%) 6 support the result of this study.
This finding was found to be lower than results from studies carried out in Hawassa (40.1%), 1 Wolayita (18.6%), 9 Mekelle (19.8%), 8 Kenya (17.5%), 21 and Tanzania, Dare Salam (21%) 22 of participants being screened, respectively.
Compared with participants who cannot read or write, primary education (grades 1–8), secondary education (grades 9–12), and higher education (grades 12+) are 3 times, 4.2 times, and 6 times more likely to use cervical cancer screening services, respectively. Similar findings were observed in studies conducted by Hawassa, 1 Gondar, 18 Wolaita, 9 and Mekelle 8 where the level of education can predict the use of cervical cancer screening services.
Compared with respondents who had given birth twice, those who had never given birth were 74.4% less likely to be screened for cervical cancer. This may be because women who have not given birth before have less access to information, counseling, and cervical cancer screening services. This is consistent with a study conducted at Arba Minchi, which showed that multi-parities are closely related to the use of cervical cancer screening services. 10 Comparable studies conducted in Tanzania indicate that women who have given birth are more likely to use cervical cancer screening services than women who have never given birth. 22
According to the result of this study, those who were looking for information about cervical cancer were about 3.4 times more likely to use cervical screening than those who were looking for information about cervical cancer. This finding was consistent with the result of a study done in Dare Salam, which indicated that the national health system factors influencing the early uptake of cervical cancer screening services include poor flow of information from national to lower level. 23
Limitation of the study
Since the study is facility-based study, it may not represent for all women not visited health institution during the study period. Therefore, we recommend future studies at the community level in the study area. Further research is needed to conduct qualitative research to find unknown reason why not being screened for cervical cancer.
Conclusion
This study has shown that there was low cervical cancer screening service utilization in the study area. In addition, educational status, parity, and looking for cervical cancer information were independently associated with cervical cancer screening utilization. Therefore, stakeholders should improve women’s education, dissemination of information about importance of cervical cancer screening, and focus on nulliparous women to have good practice of cervical cancer screening.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221094904 – Supplemental material for Utilization of cervical cancer screening service and associated factors among women of reproductive age group in Ilu Abba Bor zone, southwestern Ethiopia, 2019: Cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221094904 for Utilization of cervical cancer screening service and associated factors among women of reproductive age group in Ilu Abba Bor zone, southwestern Ethiopia, 2019: Cross-sectional study by Dejene Edosa Dirirsa, Eyosiyas Yeshialem Asefa and Mukemil Awol Salo in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank Mettu University and colleagues for their valuable support throughout the research process. Our acknowledgment also extends to zonal health department and respective health facility officials for permitting us to do so as well as involved data collectors and supervisors for their commitment during the data collection process.
Author contributions
D.E.D. and E.Y.A. originated the idea and participated in the proposal development, questionnaire development, data collection, and analysis. D.E.D. and M.A.S. participated in manuscript writing. All authors read the final version of the manuscript and approved this version of the manuscript to be considered for publication.
Availability of data and materials
Data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Prior to data collection, ethical clearance was obtained from Research and Ethical committee of College of Health and Medical Sciences of Mettu University with the approval number MU/67/566/19. Written permission letter was produced from Ilu Abba Bor zonal Health Office and other concerned bodies in the study area. During data collection, each respondent was informed about the purpose, scope, and expected outcome of the research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The whole required (material and humanitarian) cost for this research work was covered by Mettu University.
Informed consent
Informed written consent was obtained from each subject and legally authorized representatives of the subjects who were minors before proceeding data collection.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.