
Abstract
Background:
Urinary tract infections are the primary factors that cause mortality and morbidity in patients with underlying comorbid conditions and are responsible for most hospital admissions worldwide.
Objectives:
The study aims to identify the common bacterial uropathogens and determine their antimicrobial susceptibility pattern, including multidrug-resistant/extensively drug-resistant bacteria.
Methods:
The descriptive cross-sectional study was conducted among inpatients provisionally suspected of urinary tract infections in the medical ward of Koshi Hospital, Biratnagar, Nepal. Samples were inoculated in a cystine lysine electrolyte-deficient medium, and pure growth of significant bacteria was further subjected Gram staining, biochemical identification, and antimicrobial susceptibility testing as per laboratory standard procedure and Clinical Laboratory Standards Institute guidelines, respectively. Descriptive and inferential statistical analysis was performed to analyze the outcomes and a p-value < 0.05 was considered statistically significant.
Results:
A total of 305 patients urine specimens were examined, of which 251 (82.29%) samples resulted in significant bacterial growth in the culture. Escherichia coli (62.94%) was the most predominantly isolated organism, followed by Klebsiella pneumoniae (12.35%), Staphylococcus aureus (9.16%), and Pseudomonas aeruginosa (8.76%). Among antimicrobials, colistin had shown absolute susceptibility (100%) toward gram-negative uropathogens followed by carbapenem and aminoglycosides in a majority of uropathogens. Escherichia coli was found to be the leading drug-resistant bacteria (70%) among uropathogens. The presence of multidrug-resistant/extensively drug-resistant bacteria uropathogens was found to be significantly associated with diabetes mellitus and those with combined antimicrobial therapies. Diabetic patients were twice (OR~2) more likely to colonize and develop uropathogens as compared to non-diabetics.
Conclusion:
Escherichia coli was the most common uropathogens followed by Klebsiella pneumoniae in urinary tract infection patients. The polymyxin group (colistin) of antimicrobials was found to be effective in all multidrug-resistant and extensively drug-resistant uropathogens. The study recommends the need of optimized antimicrobial stewardship program to develop effective strategies in the management of urinary tract infections in diverse healthcare settings.
Introduction
Urinary tract infections (UTIs) and antimicrobial resistant (AMR) have become major public health problems worldwide, posing substantial health complications and socioeconomic burdens to society. 1–3Escherichia coli is the most prevalent microorganism, followed by Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterococcus faecalis, Staphylococcus aureus, Proteus mirabilis, Candida albicans, Acinetobacter baumannii, and Citrobacter spp. 4 Community-acquired UTIs affects more than 150 million individuals annually and the mortality associated with UTIs is increasing annually by 0.55%.1,5 Furthermore, antimicrobial resistance in UTIs has presented a significant challenge to global health and urological infection treatment strategies. 3 There is a rising concern about UTIs in developing countries. 6 Extensive use of antibiotics in the past has enhanced the survival of resistant strains. 7 In Nepal, around 13%–37% of Nepalese adults were estimated to attend and seek hospital services for UTIs.8 –10 In many cases, microorganism has developed resistance to first-line antibiotics and shows the necessity for second-line antibiotics, which is broad-spectrum, have a less favorable risk-benefit profile, are more expensive, and may be locally unavailable.11,12 Isolated pathogen and prevalence of antibiotic resistance rates may vary on geographical location and regions of the country; therefore, it is prudent to adhere to the most up-to-date evidence and current guidelines when selecting antibiotics to optimize the treatment of UTIs.7,13 To ensure appropriate therapy, updated understanding of the organisms that cause UTI and their susceptibility pattern is essential. Therefore, this study aims to identify common uropathogens and explore antibiotic-resistant patterns of uropathogens in this area of eastern Nepal concerning multidrug-resistant (MDR) and extensively drug-resistant (XDR) uropathogen as well as to explore the associated risk factor that determines the colonization of MDR/XDR. The rationale for conducting this study stems from the growing concern about rising antimicrobial resistance, which poses significant challenges in the effective management of UTIs. The emergence of MDR uropathogens has led to treatment failures and adverse patient outcomes. Understanding the factors contributing to the development of drug-resistant is crucial for implementing targeted interventions and improving patient care. Furthermore, the significance of this study lies in its potential to contribute toward assessing, identification, and detection of prevalent uropathogens and factors associated with drug-resistant UTIs, which could aid healthcare professionals to develop evidence-based strategies for early detection, appropriate treatment, and infection control measures. To address this knowledge gap, our study aims to investigate the antimicrobial resistance patterns of uropathogens in a specific healthcare setting and identify the risk factors associated with MDR profiles. The findings of this study could have implications for clinical practice, infection control policies, and the development of effective treatment strategies for UTIs.
Methodology
Study design, period, and area: A cross-sectional study was conducted from October 2020 to March 2021 among inpatients admitted to medical wards at Koshi Zonal Hospital. The Koshi Zonal Hospital is a 300-bedded tertiary care government hospital located in Eastern Development Region (26.45°N, 87.26°E) at Koshi Province, Nepal. As a prominent healthcare facility in the region, Koshi Hospital serves a diverse patient population.
Study population and criteria: The study population includes adult inpatients irrespective of gender admitted in the medical ward and clinically suspected patients were subjected to routine urine microscopy examination test followed by urine culture and sensitivity test based on the clinician’s reference. The inclusion criteria includes patient who had undergone prior urine routine examination (Urine R/E), and suspected with UTIs and those providing consent for the study was included in our study. Exclusion criterion includes inpatients who had not tested for urine routine examination, as well as all samples from the outpatient department and the specimens from pediatric age groups.
The selection criteria for variables were determined based on their relevance to the research objectives and their potential outcomes. The primary outcome variable was to determine prevalent uropathogens and their drug-resistant profiles from collected urine samples. The evaluation was carried out using standardized antimicrobial susceptibility testing following recent Clinical and Laboratory Standards Institute (CLSI) guidelines.
Sample size calculation and sampling techniques
Sample size calculation was done by application of sensitivity of gold standard from a previous study 14 applying, 5% margin of error and 95% confidence level, and a prevalence of 25.24% estimated from a previous study conducted by Joshi et.al. 9

N = 290.
Q = (1–P)
N = Sample size
Z = Z statics for a level of confidence (At 95% confidence level, Z = 1.96)
SE = Sensitivity of urine culture from the previous study that is, 95%
P = Expected prevalence or proportion population based on previous studies (i.e., 25.24)
d = Margin of error (5%) at 95% confidence intervals (CI).
The required sample size is 292. Adding extra 15 (5%) samples to overcome some unlabeled, mislabeled, leaked containers, contaminated samples, or non-clean catch midstream urine. Therefore, our sample size was estimated to be 290 + 15 (5% of 290) = 305.
Diagnostic criteria: UTIs were diagnosed through a comprehensive approach involving clinical findings, routine urine microscopy examination, and urine culture. The primary suspicion of UTIs in our study population was initially assessed through clinical findings and routine urine microscopy. Patients admitted to the medical ward who were provisionally suspected of UTIs by physicians based on clinical findings were all subjected to routine urine microscopy. Subsequently, symptomatic patients who exhibited no signs of UTI in routine microscopy were also identified as suspected cases. These suspected cases underwent confirmation by urine culture and sensitivity tests. The diagnostic threshold for UTIs was considered met when the culture results indicated the presence of >100,000 colony forming units (CFU)/ml in female patients and >1000 CFU/ml in male patients, following Kar’s semi-quantitative method. This threshold was deemed significant bacteriuria, even in the absence of clinical symptoms. For cases where clinical findings suggested a UTI but routine microscopy did not reveal significant abnormalities were also subjected to urine culture. Therefore, clinical findings and culture played a crucial role in diagnosis of UTI in ruling out false negativity by urine routine examination. Additionally, the isolation of more than three different colonies of bacteria in cystine lysine electrolyte-deficient (CLED) was reported as ‘contaminants’. 15
Data collection techniques
Data were collected in a data collection tool referring to the inpatient’s case sheets and laboratory reports including culture, and sensitivity test of urine samples of participant. Female participants were informed to clean their peri-urethral area with soap and water then cleanse the area applying sterile gauze to collect 5–10 ml of freshly voided midstream urine using sterile and wide-mouthed plastic bottles with a tight cap. Then the collected midstream urine specimens were transferred to the medical microbiology laboratory of Koshi Zonal Hospital. Most of the urine samples were processed within 2 h, and about (0.1 g) of boric acid was used as a preservative and refrigerated at 4°C if the transport of the specimens was delayed.
Ethical considerations and patient consents
Ethical approval was obtained from the Institutional Review Committee of Purbanchal University College of Medical and Allied Science (PUCMAS) (Ref no IRC/014/2020). The study was undertaken during the COVID-19 pandemic surges up period and involves analysis based on routine laboratory culture and sensitivity tests on clinician’s references. Therefore, verbal informed consent was obtained by the researcher and clinical staffs following brief explanation and clarification of objectives and purpose of study.
Laboratory proceeding for urine culture, bacterial identification, antimicrobial susceptibility tests, and quality control
Urine culture was preceded by applying a semi-quantitative method on CLED (HiMedia, India) agar plates with an Andrade indicator. The inoculating loop that possesses standard dimension was calibrated to ensure the volume of urine adjusted in a loop (0.001 ml) for inoculation of a urine sample. The samples were mixed properly so that bacteria remain uniformly suspended before inoculating in CLED. The samples were inoculated to CLED agar and incubated for 24 h at 37°C.
Bacterial identification: Identification tests of both gram-negative and gram-positive bacteria were done by using conventional biochemical tests such as catalase test, oxidase test coagulase test, triple sugar iron, sulfite indole motility test, citrate utilization test, urea hydrolysis agar, MethylRed/Voges-Proskauer test, sugar fermentation tests such as glucose, sucrose, and lactose, alcohol fermentation tests such as mannitol, sorbitol, dulcitol, adonitol as well as amino-acid decarboxylase tests such as Lysine, ornithine, and arginine decarboxylate test. 15
Antibiotics susceptibility test: Antibiotics susceptibility test was performed using Kirby–Bauer disk diffusion test on Mueller–Hinton Agar (MHA) (HiMedia, India) 16 applying following antibiotic disks: For gram-negative bacteria: amikacin (30 µg), gentamicin (10 µg), ampicillin (10 µg), ampicillin/sulbactam (10/10 µg), amoxicillin/clavulanic acid (20/10 µg), ceftazidime (30 µg), ceftriaxone (30 µg), cefotaxime (30 µg), cefixime (10 µg), meropenem (10 µg), ciprofloxacin (5 µg), nitrofurantoin (300 µg), norfloxacin (10 µg), gentamicin (10 µg), tobramycin (10 µg), cotrimoxazole (25 µg), colistin (10 µg), and piperacillin/tazobactam (100/10 µg) (HiMedia, India) were applied. Additionally, the following antibiotics disks were selected based on the availability and recommendations from CLSI guidelines for gram-positive bacteria: ampicillin (10 µg), ampicillin/sulbactam (10/10 µg), amoxicillin/clavulanic acid (20/10 µg), meropenem (10 µg), ciprofloxacin (5 µg), nitrofurantoin (300 µg), norfloxacin (10 µg), linezolid (30 µg), and additionally ceftriaxone (30 µg), amikacin (30 µg), or gentamicin (10 µg) was tested for Staphylococcus aureus. Furthermore, based on CLSI guidelines 2020, 17 to report the susceptibility of colistin (for gram-negative bacteria) and vancomycin (for S. aureus and Enterococcus species), the minimum inhibitory breakpoints (MIC < 2 µg/ml) were determined using micro-broth dilution method by adding bacterial suspension that was adjusted to 0.5 M McFarland in an antibiotic concentration (4, 2, 1, 0.5 and 0.25 µg/ml) in four test tubes following serial dilutions.
Quality control
Strict measures were followed from the pre-test to the post-test phase. The questionnaire was pretested in 15 patients with symptomatic bacteriuria at Koshi Zonal Hospital. All the laboratory tools and reagents were validated before the experiment. Quality control of each agar plate prepared was checked by incubation of the plate in the incubator after preparation. The American Type Culture Collection (ATCC) strains were used to check the efficacy of various prepared biochemical for microbe identifications. For correct interpretation of disk diffusion tests, at first, the thicknesses of MHA were maintained approximately 4 mm as well as pH was adjusted to 7.2–7.4 before preparation based on the manufacturer’s instructions. Freshly prepared media were tested using control species of bacteria (i.e. known organisms to check its indicators performance). For validation of Gram staining kits E. coli (ATCC 25922) and S. aureus (ATCC 25923) were used on slides to ensure proper binding of dye based on organisms. The ATCC strains of E. coli (ATCC 25922) were used to observe the quality control of antibiotics disks to minimize experimental errors. The laboratory equipment was calibrated from time to time for efficacy. The documentation of temperature was done every day for refrigerators and bacterial incubators. The autoclave tapes were applied to validate the temperature (121°C) for the sterilization of culture media.
Case definition
Significant bacteriuria: Significant bacteriuria is defined as the presence of a significant quantity of bacteria in the urine, typically indicating UTI. The presence of a specific threshold of bacteria is considered significant (generally > 105 CFU/ml for a single bacterium). However, the threshold was considered lower than 105 for certain populations such as elderly age groups, males, symptomatic individuals, urinary catheters, low immune status, and urine collected via bladder aspiration. 15
MDR/XDR and pan drug-resistant
MDR bacteria are defined as bacterium resistant to at least three or more categories of antibiotics of different groups. XDR organisms are designated as a bacterium resistant to at least one antimicrobial category of all groups but remains susceptible to fewer (one or two) antimicrobials. Pan-drug resistant (PDR) organisms are known as drug-resistant acquired by bacteria to almost all the commercially available antibiotics. 18
Conditions applied for designating MDR, XDR and PDR in both
Data processing and analysis
The collected data were entered in MS Excel 2019 to record all relevant information such as patient’s demographic details, comorbidities, and culture and sensitivity test report following the outcomes. Descriptive statistics were calculated to summarize the characteristics of the study population and key variables. Frequencies and proportions were used to describe categorical variables, whereas measures of central tendency (mean, median) and dispersion (standard deviation) were used for continuous variables. Bivariate analysis was conducted to explore the relationships between the independent variables and the outcome variable of interest MDR/XDR profile. Chi-square tests were performed to assess associations between categorical variables, such as age, gender, diabetes, hypertension, and multiple antibiotic therapy, with the MDR/XDR profile. Multivariate analysis was conducted using binary logistic regression to examine the independent effects of the variables on the MDR profile while controlling for potential confounding factors. The crude odds ratio (COR) and adjusted odd ratio (AOR), 95% CI, and p-values were reported to quantify the associations. Age, gender, diabetes, hypertension, and multiple antibiotic therapy were included as independent variables in the regression model (bivariate). To address potential confounding effects, known potential confounders identified in the literature and based on biological plausibility were included as covariates in the regression model. These confounders included comorbidities such as diabetes mellitus and other factors such as multiple antimicrobial therapies. In this study, multi-collinearity among independent variables was known using the standard error of regression coefficients and Pearson correlation. Statistical significance was determined using a significance level of p < 0.05. All statistical analyses were performed using SPSS version 17 (IBM Corp., Armonk, NY, USA).
Results
Demographic data and baseline characteristics of the patients
A total of 305 patients participated in our study, of which the majority of participants were female (69.8%) as compared to male (30.2%). The mean ages of the participants were found to be 43.94 years (SD ± 19.11). Most patients were married (79.7%). The most common comorbidity was diabetes mellitus (27.2%) followed by hypertension (13%) as illustrated in Table 1.
Demographic baseline data and characteristics of participants (N = 305).

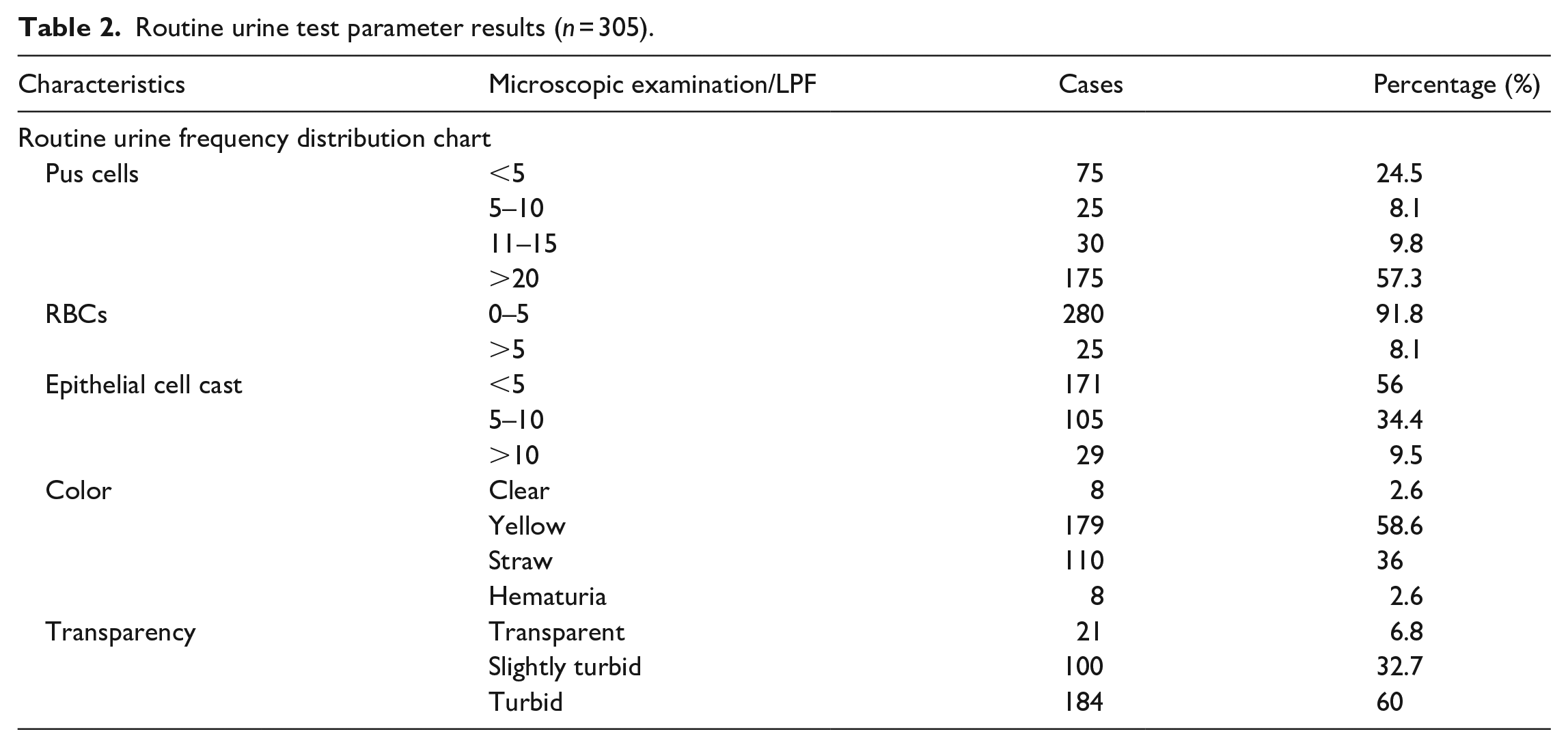
While going through routine microscopic examination of urine specimens, our results showed that the majority of UTI-suspected patients (75.2%) had pyuria (pus cell ⩾5/HPF). Some degree of microscopic hematuria (>5/HPF) was present in 8.19% of patients and 43.9% of patients had high epithelial cell cast >5/HPF. The results are summarized in Table 2.
Routine urine test parameter results (n = 305).
Out of a total of 305 samples processed for urine culture and sensitivity, 54 (17.70%) showed no growth. About 251 (82.29%) samples revealed growth in the culture. E. coli (62.94%) was a highly isolated species from urine culture that caused the majority of UTIs in patients followed by K. pneumoniae (12.35%), S. aureus (9.16%), P. aeruginosa (8.76%), A. baumannii (3.18%), E. faecalis (1.99%), and least UTI cases were caused by P. mirabilis (1.59%). The frequency and proportions of uropathogens are represented in Table 3.
Isolated bacterial frequency distribution from urine culture reports (n = 251).

Antimicrobial-resistant rates of uropathogens
Antimicrobial-resistant rates were observed against five gram-negative bacteria and two gram-positive bacteria. Based on results represented in Table 4, there was no drug-resistant observed in colistin in all tested four gram-negative bacteria (Resistant rate = 0) except P. mirabilis due to intrinsic resistant nature for colistin, and no resistant was observed for vancomycin and linezolid in two isolated gram-positive bacteria (S. aureus and E. faecalis). The least resistant patterns were observed for aminoglycoside group on a majority of tested strains of gram-positive and gram-negative uropathogens. Penicillin group (ampicillin, piperacillin) showed low antimicrobial activity (Resistant rate, >80%) against both gram-positive and gram-negative bacteria, whereas penicillin/beta-lactamase inhibitors (amoxycillin/clavulanate, ampicillin/sulbactam) showed a good spectrum of antimicrobial activities against some gram-positive and gram-negative bacteria such as S. aureus, A. baumannii, and E. faecalis. The results of commonly tested antimicrobials are summarized and depicted in Table 4.
Antimicrobial resistant rates of commonly tested antibiotics on various uropathogens.

IR: intrinsic resistant; NT: not tested.
“0” indicates that there is no resistant observed among tested isolates.
MDR and XDR uropathogens
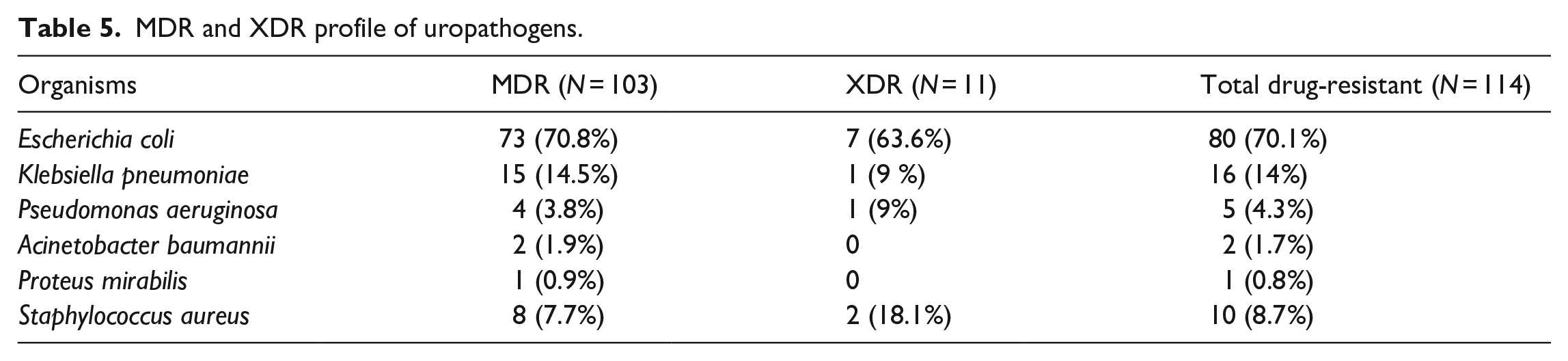
Different groups were tested in both gram-positive and gram-negative bacteria to evaluate MDR and XDR profiles. Out of them, altogether n = 114 (45.4%) bacteria fall under the criteria of MDR bacteria. Based on the number of isolated MDR and XDR strains, the leading proportion of MDR and XDR gram-negative bacteria was noted in E. coli (MDR n = 73 (70.8%) and XDR n = 7 (63.6%)). The majority of MDR E. coli was predominantly resistant to penicillin group (ampicillin), folic acid inhibitors (cotrimoxazole), fluroquinolones (norfloxacin, ciprofloxacin), and beta-lactam/beta-lactamase inhibitors associated antibiotics groups such as ampicillin/sulbactam, amoxycillin/clavulanate, and piperacillin/tazobactam. On the other hand, among two gram-positive bacteria (S. aureus and E. faecalis), MDR and XDR were observed only in S. aureus (MDR, n = 8 (7.7%), and XDR n = 2 (18.1%)). Similarly, there were no PDR urinary pathogens in our study as all the organisms were at least susceptible to one or two antibiotics. The results of MDR and XDR based on uropathogenic organisms are summarized in Table 5.
MDR and XDR profile of uropathogens.
Bivariate and multivariate logistic regression analysis was applied to determine the association between dependent and independent variables. Various independent groups ( gender, age groups, marital status), comorbidities (diabetes mellitus and hypertension) as well as multiple antimicrobial therapies were tested for the outcome of colonization of drug-resistant pathogens. The reference group had an odd ratio adjusted as OR = 1 as shown in Table 6. Based on bivariate analysis independent variables such as diabetes mellitus and combined antimicrobial therapy showed a strong association (p < 0.05) with the outcome that is, drug-resistant uropathogens (resistant acquired to at least three drugs of a different group) and the variables were further subjected to multivariate analysis. Based on multivariate analysis, diabetes mellitus was found to be the leading risk factor (Table 6) for the colonization of MDR/XDR among all the independent variables (OR = 2.0, 95% CI: 0.03–0.28) in our study, but patients who had undergone combined antimicrobial therapy had 90% of lower odds (OR = 0.10, 95% CI: 0.03–0.28) in colonization risk as compared with the patients who did not follow combined antimicrobial therapy which was found to be statistically significant (p < 0.05).
Risk factors associated with the development and colonization of MDR/XDR uropathogens (N = 251).

COR: crude odd ratio; AOR: adjusted odd ratio; ref: reference in a dichotomous variable; NA: not applicable; CI: confidence interval; p-value: probability value.
Discussion
UTIs are common worldwide and range from mild symptoms to severe complications. 19 The treatment of UTI is becoming challenging due to the emergence of MDR microorganisms.2,11 In our study, mostly females (69.8%) had UTIs as compared to males. Females are more prone to UTIs because of several reasons including anatomy based on gender that is, shorter urethra, the proximity of the urethra to the anus in females as well as entry of pathogens promoted by sexual intercourse among females with relationship status in sexually active age group, and other factors like estrogen deficiency. 20 Based on our study, diabetes mellitus 83 (27.2%) was the most common comorbidity among patients with UTI. As UTI cases are more prominent in diabetic patients compared to non-diabetics. 21 The reason for this is not well explained, but two hypothetical explanations are supported by published study that is, dysfunction of the urinary bladder and poor prognosis manifested as glycosuria might increase the risk as explained by De Lastours et al. 22 as the bacteria might replicate utilizing the glucose in urine.
In this study, the urine routine microscopy parameters were taken as a marker in prompt diagnosis of UTI as urine culture takes at least 24 h to diagnose the infection. Routine urine examination shows a significant amount of pyuria (75.2%) in most of the participants. These findings are supported by the study conducted in central Nepal which determined the pyuria as a prime marker for suspecting UTI. 23 Concordantly, the rise in epithelial cells in cases of participants also primarily suggests performing cultures for confirmation of UTIs. This conclusion has been supported by a study conducted at the University of Iowa that had shown some efficacy in predicting bacteriuria. 24
In our study, E. coli was the most frequently isolated uropathogen (62.94%) followed by K. pneumoniae (12.35%). Several reports of uropathogens among UTI-suspected cases in Nepal had similar trends of isolated bacteria consistent with our findings.8,10,11,25 Other isolated uropathogens in this study include two gram-positive bacteria: S. aureus and E. faecalis. S. aureus caused significantly higher UTI cases (9.16%) as compared to E. faecalis (1.99%). These findings were alternative to study conducted in other regions of Nepal9,26 and Srilanka 27 where S. aureus was isolated around 11.63%, 7.55%, and 3.6% of UTI infection, respectively, with a relatively low isolate of E. species. The incidence of non-fermenter gram-negative bacteria in UTI has risen recently. 28 Common non-fermenter bacteria include P. aeruginosa and A. baumannii, which were mostly involved in hospital-acquired infection rather than community-acquired. Consequently, P. aeruginosa had a greater prevalence than A. baumannii in our study setting, respectively. Prevalence of P. aeruginosa exceeding A. baumannii has been documented in several studies.29,30 The least isolated species among gram-negative uropathogens in our study was found to be P. mirabilis (1.55%). A study done by Jamil et al. 31 also concluded that P. mirabilis had the least prevalence approximately 1%–2% after reviewing various studies.
In this study, the results of the antimicrobial-resistant pattern assessed on different antibiograms demonstrate that two groups of antibiotics (cephalosporin and penicillin groups) show higher resistant rates for all isolates, whereas the polymyxin group remains highly susceptible to the drug-resistant uropathogens. Similar studies conducted in Nepal11,12 and another country32 –34 had revealed a higher rate of resistance among penicillin and cephalosporin group of antimicrobials. Nevertheless, the polymyxin group for gram-negative uropathogens still remains 100% susceptible for most of the severe UTI cases that were influenced by MDR/XDR bacterial strains. The outcomes of treatment effectiveness of this drug were also discussed in several recent studies as well.35,36 The glycopeptides and oxazolidinone group (vancomycin and linezolid) showed great antimicrobial potency among gram-positive bacteria in our study. The study from the USA also showed the efficacy of the broad-spectrum drug tetracycline group, glycopeptides, and oxazolidinones group had superior efficacy with low resistant rates to treat gram-positive uropathogens including methicillin-resistant Staphylococcus aureus in UTI. 37 Previous studies also suggest linezolid as an alternative treatment for vancomycin-resistant cases in S. aureus and Enterococcus species. 38
The high prevalence of MDR and XDR in our study among gram-negative uropathogens was reported in E. coli followed by K. pneumoniae, respectively. The MDR burden of E. coli and K. pneumoniae has been documented previously in different studies from Nepal.11,12,25 However, the rise of MDR P. aeruginosa has been a serious challenge to treatment prospects in developing countries.39 –41 The rising threat of MDR E. coli and K. pneumoniae similar to our study has been determined by a study conducted in Pakistan by Iqbal et al. 42 and a study in China elaborated increase in trends of XDR- K. pneumoniae posing a threat to public health. 43 Majority of other studies in MDR- E. coli had revealed drug-resistant characteristics like resistant to multiple antimicrobial group such as penicillin (ampicillin, piperacillin), beta-lactam/beta-lactamase inhibitor (ampicillin/sulbactam, amoxicillin/clavulanate), fluroquinolones (ciprofloxacin, norfloxacin, ofloxacin, etc.), and nitrofuran group (nitrofurantoin)11,25,42 which is concordant to our findings.
Based on the finding of risk factors in our study, the higher incidence of existing comorbidity like diabetes mellitus results in more than twice the greater odds of colonization and development of MDR bacteria as compared to non-diabetic patients. One reason behind it is these types of comorbidity negatively interact with the immune system which leads to develop a greater risk factor for the infection. Similarly, the pharmacokinetics of antibiotics in obese diabetic populations could also lead to suboptimal levels of antibiotic concentrations and increase the risk of antibiotic resistance.44 –46 Moreover, diabetics could acquire the most resistant strain of pathogens due to frequent hospital visits. This finding was supported by a British study on systematic review and meta-analysis that had compiled reports on the high resistant rate of antimicrobials in diabetics patients, particularly in UTIs and respiratory tract infections similar to our findings. 45 Apart from that, our findings also highlight the need for combined antibiotics therapy for the treatment of MDR and XDR bacteria. Patients under combined therapy had lower odds of MDR and XDR bacteria as compared to those who did not receive them. The study conducted in Greece highlights the need for combination therapy to treat XDR infection. 47 Another Japanese study claimed the necessity of combined antimicrobial therapy to combat MDR bacteria. 48
There are several limitations of our study as the study was a single-centered study, which limits the study to be conducted in mass sample size. The use of convenience sampling may limit the generalizability of the findings to a broader population and lack of control over the sample composition. More importantly, the research conducted in low resource country restrains us from conducting molecular assays to evaluate the genes responsible for evolving uropathogens into MDR and XDR bacteria. Despite limitations, our study possesses some strength as these findings are important for reviewing empirical therapy as the study has a prime focus on MDR/XDR strains of uropathogens. Apart from that, documentation of predisposing factors and statistical analysis determines the leading risk factor responsible for the potent carrier and rise in drug-resistant pathogens among admitted patients in a healthcare facility. Therefore, our study recommends the utilization of recent surveillance data and guidelines to optimize treatment outcomes and minimize antimicrobial resistance in healthcare settings.
Conclusion
E. coli and K. pneumoniae were the most common uropathogens in admitted patients. Colistin had greater susceptibility toward the multiple drug-resistant and extensively drug-resistant gram-negative uropathogens. The high prevalence of MDR and XDR among gram-negative uropathogens determines the vital concern to practice infection control policy in healthcare settings to prevent the transfer of drug-resistant pathogens. Diabetic patients were more prone to get infected by MDR bacteria that impose significant risk. The current study alarms the use of antibiotics only whenever necessary to prevent the colonization and development of superbugs.
Footnotes
Acknowledgements
The authors would like to acknowledge all the staffs and clinicians of Koshi hospital for cooperating, assisting for taking history and providing clinical reports and information.
Author contribution
The authors confirm their contribution to the paper as follows: study conception and design: BS, PD, SKM; Data collection: BS, CS, UM; analysis and interpretation of results: PD; Literature review and initial draft: BS, PD, SKM. Critical revision of the manuscript for intellectual content: PD, CS, DPA. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Institutional Review Committee (IRC) of Purbanchal University College of Medical and Allied Science (PUCMAS-IRC) (APPROVAL REF NO: IRC/014/2020).
Informed consent
Verbal informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.