
Abstract
Objective:
Identify the incidence and risk factors of vitamin D deficiency/vitamin D insufficiency in children aged 1–5 years.
Methods:
A cross-sectional survey was conducted among children between the ages of 1 and 5 in the Bope-Poddala and Galle municipality areas. The sample was obtained by cluster sampling method. Data on socio-demography, pregnancy, sun exposure, and diet were obtained. Serum 25(OH)D concentrations were measured and the cutoff value was determined as per the global consensus in 2016.
Results:
Among 100 children, the mean serum 25(OH)D level was 86.4 nmol/L (24.06 ng/mL). The prevalence of vitamin D deficiency and vitamin D insufficiency was 7% and 28%, respectively. Birth weight and sunlight exposure were significantly different among vitamin D deficiency/vitamin D insufficiency and sufficient groups. Both were found to be risk factors for vitamin D deficiency/vitamin D insufficiency in logistic regression.
Conclusion:
Vitamin D deficiency/vitamin D insufficiency is significant among children aged 1–5 years and decreased sun exposure and low birth weight are the main risk factors.
VDD/VDI was not a significant health problem among Sri Lankan children over the last few decades.
Rickets, the disease entity with severe VDD, was rarely seen over the last few decades.
The recent incidence of VDD is increasing among Sri Lankan children.
This article confirms that VDD/VDI will be a threat among children in Southern Sri Lanka.
Introduction
In the past few years, it has been witnessed that vitamin D deficiency (VDD) has become a global health problem in children. 1 Although several measurements were made to fix this problem, its prevalence is still increasing yearly. Low vitamin D is reported in Asian nations, but the problem is not limited to a single country or continent and has been reported globally. 2 Its role in skeletal health has been recognized for several years. 3 Earlier, Holvik et al. 4 conducted a vitamin D prevalence study and reported low vitamin D in Sri Lankan immigrants. 4 While existing literature also supports low percentages of 25 hydroxyvitamins in children aged 1–5 years. 5
Female gender, pre-term babies, preschool children, overweight, inadequate exposure to sunlight, high skin melanin content (dark skin), ethnicity (African and Asian), winter season, and low socioeconomic status are some of the well-recognized risk factors for VDD. 6 However, a number of good methodological studies were considered debatable due to their limited emphasis on school children, which showed an association between dietary factors and VDD. 7 Several researchers have also conducted studies on sleep duration and vitamin D. Although, in recent years, studies have found a relationship between physical activity and 25(OH)D status. 8 Furthermore, an inverse relationship between serum 25(OH)D and parathyroid hormone (PTH) levels has been extensively explained in the literature. 9 Hence, it is essential to maintain sufficient vitamin D levels, as elevated PTH levels are associated with bone resorption.
Vitamin D levels are related to various calcemic and non-calcemic health outcomes, namely rickets, asthma, dermatitis, diabetes, osteoporosis, lipid alterations, etc. 10 In India, a recent case–control study showed no significant difference in the serum 25(OH)D levels between the cases (the group with rickets) and controls. At the same time, much lower levels of calcium and higher intake of food with dietary phytate were observed in the group with rickets. 11 Maternal VDD is strongly associated with VDD in newborns and children aged 1–5 years. 12 The mothers of Vitamin D-deficient children with rickets were observed to have 25(OH)D levels ⩽25 nmol/L, as per a retrospective audit from Melbourne. 13
Nutritional rickets remained a most important health issue among the growing Sri Lankan children till the 1960s and 1970s due to the poor socioeconomic status and the decreased access to vitamin D-enriched diet. 14 Despite enhancement in the degree of services, availability, and access to vitamin D-enriched diet, there has been an upsurge in the number of children with nutritional rickets at Sri Lankan clinics. 15
It is necessary to introduce policies to improve vitamin D and categorize children with greater risk. Moreover, it is essential to identify factors that enhance VDD/vitamin D insufficiency (VDI) such as lifestyle, dietary levels, feeding patterns and physical activity, sun exposure, etc. This study aimed to assess the vitamin D status and the associated risk factors among children of 1–5 years of age in the Galle municipality and Bope-Poddala areas.
Methodology
A descriptive cross-sectional study was conducted in the Galle district of Sri Lanka. The cluster sampling method and the probability proportionate to the population size method were utilized in this study, and the calculated sample size was 108. Cluster sizes were determined by the number of resident children of 1–5 years of age registered in the public health midwives’ (PHM) areas of Bope-Poddala and Galle municipalities. Considering the population ratio (1–5 years) of 4476 (Galle municipality) and 5402 (Bope-Poddala), the ratio taken was 4:5.
Children of 1–5 years old from Galle municipality and Bope-Poddala areas were included in the study. Children without their parent’s consent, those who had vitamin or mineral supplements during the last 6 months, those who had chronic renal failure, chronic liver disease, cerebral palsy, preexisting disease of parathyroid, thyroid or calcium metabolism, or children who are on medications that interfere with calcium metabolism were excluded from the study.
Ethical approval was obtained from the Ethics review committee, Faculty of Medicine, University of Ruhuna (Ref # 2021.P.019; Dated February 17, 2021), and the research was conducted in conformity with the principles outlined in the Helsinki Declaration. The senior public health midwife and the primary healthcare provider (PHM) supported the selection of the study population. After obtaining informed consent from parents, only selected children were requested to participate in the study.
The study was carried out from May to August 2021. The structured predesigned questionnaire was used to collect data related to the socio-demographic characteristics, pregnancy details, breastfeeding, complementary feeding, dietary habits, lifestyle-associated factors, hours of exposure to sunlight, preexisting comorbidities, dentition, and gross motor developmental milestones. The current hours of exposure was considered as the “exposure to sunlight.” The weight and height were measured at the time of enrolment in the study. A local anesthetic agent was applied 30 min prior to phlebotomy. Blood samples of 2 mL were collected to assess serum vitamin 25(OH)D level and bone profile which measured serum calcium, serum phosphate, and alkaline phosphatase. These testings were carried out at the Chemical Pathology Department, Teaching Hospital Karapitiya.
The cutoff value for serum 25(OH)D was determined as per the global consensus in 2016. It classified VDI as serum 25(OH)D 20–30 ng/mL (50–75 nmol/L), VDD as serum 25(OH)D 20 ng/mL (50 nmol/L), and vitamin D sufficiency as serum 25(OH)D >30 ng/mL (75 nmol/L).
Statistical analysis
Using SPSS version 20.0, the gathered data were analyzed. Measures of central tendency and dispersion were used in the presentation of descriptive data. In addition, relationships between epidemiological parameters and evaluation components were analyzed. A probability value less than 0.05 was considered statistically significant.
Results
Out of 100 children, 52 were boys and 48 were girls. Weight (SD), height (SD), and body mass index (SD) at the time of data collection were 15.1 (2.6) kg, 1.01 (0.15) m, and 14.2 (1.5) kg/m2, respectively.
Based on the mean serum levels of 25(OH)D, there were 07 (7%) VDD, 28 (28%) VDI, and 65 (65%) vitamin D-sufficient children. Among 100 children, the mean serum vitamin D level was 86.4 nmol/L. The average serum vitamin D level in the 35 deficient/insufficient patients was 48.91 ± 10.99 nmol/L.
During the analysis, we have combined insufficient and deficient groups together which is denoted by VDD/VDI (Table 1).
Demographic characteristics between VDD/VDI and vitamin D-sufficient groups.

VDD, vitamin D deficiency; VDI, vitamin D insufficiency.
Values are presented as numbers (%).
Chi-square test/Fisher’s exact test; p-value <0.05 is considered significant.
Most of the vitamin D-deficient children were males (54.3%), with a monthly income between Rs. 41,000 and 100,000 (48.6%). The majority were females (55.4%) in the vitamin D-sufficient group.
The comparison of pregnancy-related complications, intake of vitamin and mineral supplements, and the diet during pregnancy between the VDD/VDI and sufficient groups is shown in Supplemental Table 1.
There were no statistically significant differences between the two groups related to pregnancy-related complications, intake of vitamin and mineral supplements, and diet during pregnancy.
The comparison of birth details, breastfeeding, complementary feeding, and sun exposure between VDD/VDI and sufficient groups is shown in Supplemental Table 2.
There were no statistically significant differences between the two groups related to the mode of delivery, period of exclusive breastfeeding, and age that introduced fish, meat, cheese, fresh milk, or formula milk. But birth weight, the age that introduced yogurt, and the duration of sun exposure showed a statistically significant difference between the VDD/VDI and the sufficient groups.
There were no statistically significant differences in the mean serum levels of phosphorus, calcium, and alkaline phosphatase between the two groups concerned and are shown in Supplemental Table 3.
Table 2 demonstrates the correlation between various factors and vitamin D levels. The duration of sunlight exposure (r = 0.533; p = 0.000) and birth weight (r = −0.228; p = 0.023) significantly correlated with vitamin D levels.
Correlation between vitamin D levels with anthropometric measures and sunlight exposure.

Correlation is significant at the *0.05 level and **0.01 level.
Odds ratio in Table 3 highlights the risk factors for VDD. Duration of sunlight exposure and birth weight showed a significant association.
Risk factors of VDD.
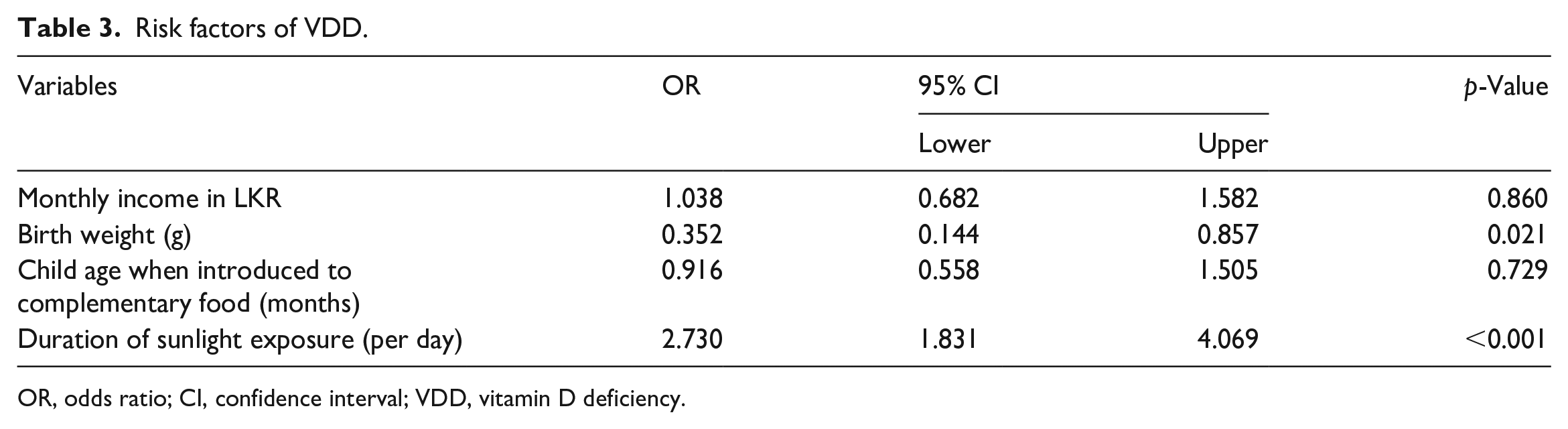
OR, odds ratio; CI, confidence interval; VDD, vitamin D deficiency.
Logistic regression was performed to investigate the risk factors related to VDD; only the duration of sunlight exposure (OR: 2.730; 95% CI: 1.831–4.069) and birth weight (OR: 0.35; 95% CI: 0.144–0.857) were found to affect VDD significantly.
Discussion
In this study, VDD was found to be common among children aged 1–5 years. The average serum vitamin D level in the 35 deficient patients was 48.91 ± 10.99 nmol/L. In a prior investigation of the vitamin D status of Korean children, Lee et al. 16 found that the mean serum vitamin D level in 2880 children was 17.42 ng/mL (43.50 nmol/L), which is comparable with our findings. In a different study including 1212 children between the ages of 4 and 15, the prevalence of VDD was 58.6%. 17 According to an Indian study, VDD was present in 93% of children who lived in high-altitude regions. Although there was plenty of sunlight in the district, subjects were at risk of vitamin deficiency due to their lack of outdoor activities which, in turn, caused decreased exposure to sunlight. An earlier study of adults aged 18–40 living in the high-altitude region of Kashmir Valley discovered that 83% had VDD. 18
There is no consensus or agreement concerning the definition of vitamin D status in children and teenagers.19,20 The lowest cutoff for vitamin D status is generally recognized as a serum 25(OH)D level of less than 10 ng/mL (25 nmol/L). 20 Serum 25(OH)D concentrations of<10 ng/mL (25 nmol/L) can cause rickets in babies and young children. 21 A serum 25(OH)D level of >20 ng/mL (50 nmol/L) is sufficient for bone health, according to the International Organization for Migration in the United States. 19 The global consensus in 2016, classified VDI as serum 25(OH)D 20–30 ng/mL (50–75 nmol/L), VDD as serum 25(OH)D 20 ng/mL (50 nmol/L), and vitamin D sufficiency as serum 25(OH)D >30 ng/mL (75 nmol/L). 22 This was due to mounting evidence that the optimal 25(OH)D level in adults may be higher than 30 ng/mL. 23
Modern society’s changing lifestyle has increased indoor activity, resulting in less sunlight exposure among children and adolescents. Lee et al. discovered that 100 Korean children aged 5–13 spent only 2.6 h/week in daylight during the winter and 3.9 h/week during the summer. They also discovered that vitamin D-deficient children spent less time outside during the day than non-deficient children. 24 Ultraviolet sun rays penetrate the skin and are required for vitamin D synthesis. The lower solar zenith angle makes it easier to absorb ultraviolet B radiation for vitamin D synthesis. An observational study found that 10–15 min of sunlight twice a week is enough to produce serum vitamin D3 in the body. 25
We found a significant association between the duration of sunlight exposure and the high prevalence of VDD (p < 0.01). In addition, it is known that obese people have lower vitamin D levels than people of normal weight. 26 Key adipose tissue-acting enzymes, including fatty acid synthase and lipoprotein lipase, are hypothesized to be inhibited in VDD, leading to fat deposition. Between the vitamin D sufficiency and deficiency groups, the current research discovered a substantial difference in birth weight, that is, 3.66 ± 0.53 g versus 3.37 ± 0.72 g (p = 0.041). Logistic regression analysis also revealed that low birth weight is a risk factor for VDD. In the past, researchers have found an association between vitamin D insufficiency and reduced calcium and greater phosphate and alkaline phosphatase levels. 27 Between patients with vitamin deficiencies and those who had enough vitamin D, the current study showed no discernible difference. Although there were slightly low serum calcium and phosphate levels while slightly raised alkaline phosphatase levels among the deficient patients.
There are some limitations to the current study. Patients from Bope-Poddala and Galle municipalities were enrolled, so the data do not represent the entire Sri Lankan population. One of the key factors influencing vitamin D status, PTH levels, was not measured. Furthermore, because no seasonal variations were tracked in this study, the effect of lack of or differential availability of daylight, subsequent exposure, and VDD was not taken into account.
Conclusion
Sun exposure duration is the most significant risk factor for VDD, and it is common in children at a young age. To improve vitamin D status, measures must be made. These include increasing outdoor activities during the day to get greater exposure to sunlight and consuming vitamin D supplements. Furthermore, we believe that, given our circumstances, supplementing the vitamin D intake guidelines is necessary.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231195997 – Supplemental material for Vitamin D level and bone profile among 1- to 5-year-old children in Galle municipality and Bope-Poddala areas in Sri Lanka
Supplemental material, sj-docx-1-smo-10.1177_20503121231195997 for Vitamin D level and bone profile among 1- to 5-year-old children in Galle municipality and Bope-Poddala areas in Sri Lanka by Pushpika Jayawardana and Gayani Liyanage in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231195997 – Supplemental material for Vitamin D level and bone profile among 1- to 5-year-old children in Galle municipality and Bope-Poddala areas in Sri Lanka
Supplemental material, sj-docx-2-smo-10.1177_20503121231195997 for Vitamin D level and bone profile among 1- to 5-year-old children in Galle municipality and Bope-Poddala areas in Sri Lanka by Pushpika Jayawardana and Gayani Liyanage in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121231195997 – Supplemental material for Vitamin D level and bone profile among 1- to 5-year-old children in Galle municipality and Bope-Poddala areas in Sri Lanka
Supplemental material, sj-docx-3-smo-10.1177_20503121231195997 for Vitamin D level and bone profile among 1- to 5-year-old children in Galle municipality and Bope-Poddala areas in Sri Lanka by Pushpika Jayawardana and Gayani Liyanage in SAGE Open Medicine
Footnotes
Acknowledgements
We are thankful to all parents who consented to participate with their children in this study. The Medical Officers of Health and public health midwives in Galle municipality and Bope-Poddala areas helped us in the selection of eligible children. The director of Teaching Hospital Karapitiya for authorizing the use of the laboratory facilities and the chemical pathologist for the assistance given in the analysis of serum samples. The authors wish to acknowledge the directors of George Steuart Health for the financial assistance offered to them. Furthermore, the authors would like to acknowledge the Medical Affairs department of Getz Pharma for their technical support and assistance in the publication process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received a research grant from the Faculty of Medicine, University of Ruhuna. The remaining expenditure was supported by George Steuart Health.
Informed consent
Written informed consent was obtained from all parents or the child’s legally authorized representative to publish this research data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.