
Abstract
Background:
In Jordan, many studies reported various rates of vitamin D deficiency and insufficiency among different groups. This study aimed to determine the prevalence of low vitamin D level among Jordanian adults and determine its association with selected variables.
Methods:
The vitamin D level was assessed in a national representative sample of 4056 subjects aged >17 years. The study involved face-to-face interviews with the subjects and measurement of serum 25(OH)D. Low vitamin D level was defined as 25(OH)D < 30 ng/mL. Deficiency was defined as 25(OH)D < 20 ng/mL, and insufficiency was defined as 25(OH)D level of 20–30 ng/mL.
Results:
The overall prevalence of low vitamin D status (25(OH)D < 30 ng/mL) was 89.7%, with higher prevalence in males (92.4%) than in females (88.6%). Vitamin D was sufficient in 7.6% of males, insufficient in 38.4% of males, and deficient in 54% of males. Among females, vitamin D was insufficient in 10.1% and deficient in 78.5%. The prevalence of vitamin D deficiency was much higher in females than in males (p = 0.001). The only variables that were significantly associated with low level of vitamin D were gender, age, obesity, and employment.
Conclusion:
The prevalence of low vitamin D level is extremely high in Jordan. Age, gender, obesity, and unemployment were associated with low levels of vitamin D. Health authorities in Jordan need to increase the level of awareness about vitamin D deficiency and its prevention, particularly among women.
Introduction
Vitamin D deficiency is currently recognized as a common public health problem. 1 The role of vitamin D in calcium and phosphate homeostasis and skeletal and non-skeletal health is well established. Vitamin D deficiency plays an important role among other factors in metabolic bone disorders leading to osteomalacia in adults and rickets in children. 2 Vitamin D deficiency is associated with many chronic diseases including cardiovascular diseases, hypertension, diabetes, metabolic syndrome, depression, autoimmune diseases, cancer, neurocognitive function, and increased occurrence of infection.3–7
Almost 90% of the human endogenous vitamin D is synthesized primarily in the skin by activation of 7-dehydrocholesterol triggered by the exposure to ultraviolet (UVB) sunlight, so limited exposure to the sunlight might lead to vitamin D deficiency. The remaining 10% is acquired from nutritional sources such as codfish, mushrooms, milk, eggs, and fortified food. Although vitamin D synthesis depends on UVB sunlight exposure, many other factors such as age, obesity, skin color, dress style, and sunscreen-use might affect vitamin D level. 8
In Arab countries, with sunlight throughout the year, vitamin D serum levels are expected to be adequate, yet studies from different Arab countries showed high prevalence of vitamin D deficiency and insufficiency.9–14 Globally, the prevalence of vitamin D deficiency is very high and varies from 70% to 90% in different populations.15,16
In Jordan, studies reported various rates of vitamin D deficiency and insufficiency among different groups. A 2009 national study showed that 37% of women were vitamin D deficient. 17 Another study reported a much higher prevalence rate of vitamin D deficiency (62.3%) among women. 18 This study aimed to determine the prevalence of low vitamin D level among Jordanian adults and determine its association with selected variables.
Methods
Sampling and data collection
This national cross-sectional study was conducted among Jordanian adults over a period of 4 months between May and August 2017. A population-based household sample was selected from 12 governorates covering the three regions of the country; the north, middle, and south. A multistage sampling technique was used to select the participants. A systematic sample of households from the catchment areas of 17 selected health centers was selected. A team of two members (a male and a female) visited the selected households and invited household members ⩾18 years of age to participate in the study and to report next morning to the health center after an overnight fast.
Data collection and laboratory analysis
Trained persons interviewed the participants using a structured questionnaire. The questionnaire was developed by the research scholars to study various risk factors of cardiovascular diseases and nutritional status in Jordan including vitamin D deficiency. The same questionnaire was used in previous national surveys in 1994, 2004, and 2009. The questionnaire included sociodemographic variables and information on diabetes and other cardiovascular disease risk factors, morbidity, quality of life, and health services. Height, weight, waist and hip circumferences, and blood pressure were carried out in a standard way by trained research scholars. Three blood samples were drawn from a cannula inserted into the antecubital vein and used for different laboratory measurements. Samples were centrifuged within 1 h at the survey site, and transferred by separate labeled tubes in ice boxes to the central laboratory of the National Center of Diabetes, Endocrinology, and Genetics in Amman, Jordan. All biochemical measurements were carried out by the same team of laboratory technicians using the same method throughout the study period. 25-Hydroxyvitamin D (25(OH)D) was measured using the ARCHITECT 25-OH Vitamin D assay (Abbott Laboratories, Abbott Park, IL, USA). The assay is a delayed, one-step immunoassay with 6-point calibration. The method is used for the quantitative measurement of 25(OH)D in human serum and plasma samples. Low vitamin D level was defined as 25(OH)D < 30 ng/mL. Deficiency was defined as 25(OH)D < 20 ng/mL and insufficiency was defined as 25(OH)D level of 20–30 ng/mL. 19 Body mass index (BMI) was calculated by dividing the weight (kg) by the height (m2). Participants with BMI of 30 kg/m2 or more were considered obese.
The study was approved by the Ethical Committee at the National Center for Diabetes, Endocrinology, and Genetics, Amman, Jordan. Written informed consent was obtained from each participant. All participants were informed that their information will be kept confidential.
Statistical analysis
Data were described using mean values and percentages. Differences between proportions were tested using Chi-square test. Multivariable logistic regression analysis was performed to identify factors associated with low levels of vitamin D. For this purpose, vitamin D level was dichotomized, using 30 ng/mL as cutoff point, and entered into the model as a dependent variable. All other relevant variables were treated as independent variables. Variables showing no relationship to vitamin D status were excluded from the model, and the process was repeated until the best model was obtained. A p-value of less than 0.05 was considered statistically significant.
Results
Participant characteristics
This study included a total of 4056 subjects (1193 males and 2863 females), aged between 18 and 90 years. Table 1 shows the sociodemographic and relevant characteristics of the study participants. The mean age was 43.8 (SD = 14.3) years. The prevailing skin color of participants was wheatish (about 54.3%); 15.9% had dark skin, and the rest were whites or blondes.
Distribution of the study population by sociodemographic characteristics.

SD: standard deviation; BMI: body mass index.
Prevalence of low vitamin D
Table 2 shows the mean values of serum 25(OH)D according to gender and age. The mean values were significantly higher in males than in females across all age groups. The overall crude prevalence of low vitamin D status (25(OH)D < 30 ng/mL) was 89.7%, with higher prevalence in males (92.4%) than in females (88.6%). Vitamin D was sufficient in 7.6% of males, insufficient in 38.4% of males, and deficient in 54% of males. Among females, vitamin D was insufficient in 10.1% and deficient in 78.5%. The prevalence of vitamin D deficiency was much higher in females than in males (p = 0.001). The prevalence rates of low vitamin D level differed significantly according to age, years of education, marital status, and occupation among females only. (Table 3).
Vitamin D status by age and gender (Jordan, 2016).

SD: standard deviation.
Prevalence of low vitamin D (25(OH)D < 30 ng/mL) in the study population among males and females according to selected variables.

Multivariate analysis of factors associated with low vitamin D
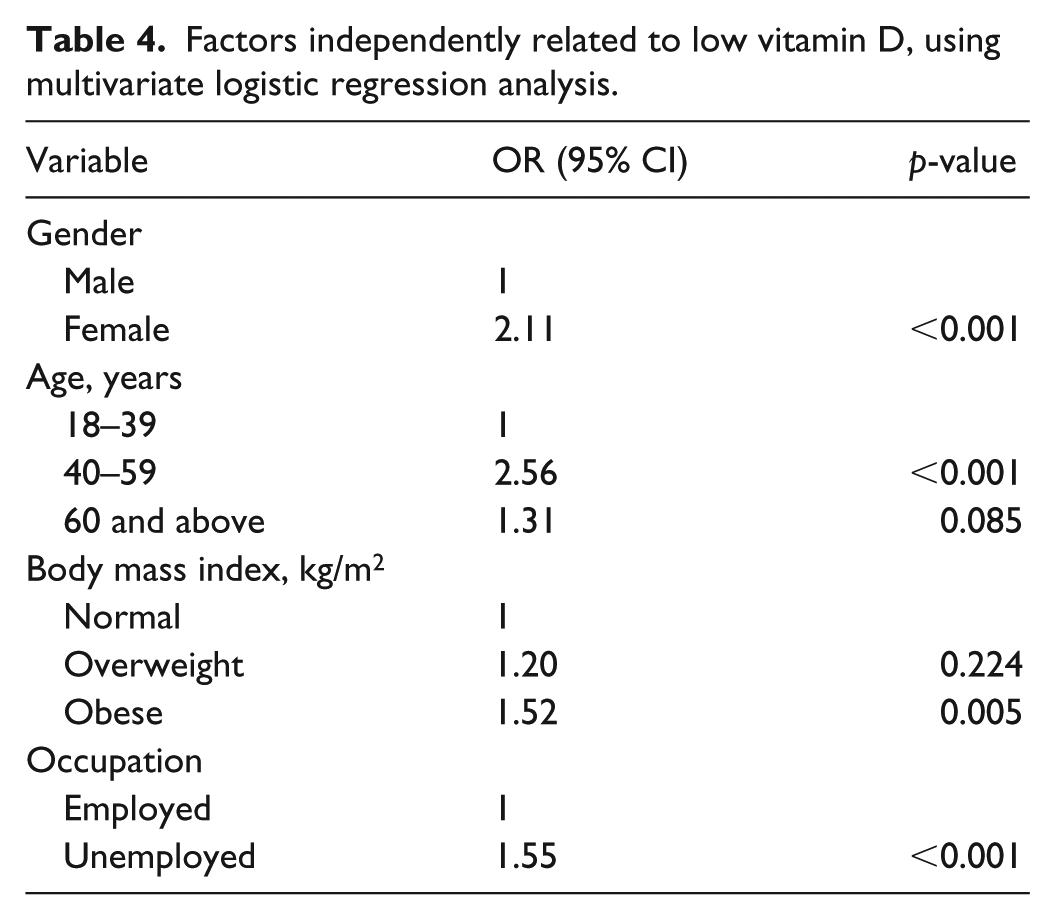
The multivariate analysis of factors associated with low level of vitamin D is shown in Table 4. The only variables that were significantly associated with low level of vitamin D were gender, age, obesity, and employment. The odds of low vitamin D level among women was almost twice that odds for men (odds ratio (OR) = 2.11). People aged 40–59 years had higher odds of low vitamin D level (OR = 2.56) compared to those who were younger than 40 years. Obesity was associated with increased odds of low vitamin D level (OR = 1.52). Unemployed people had higher odds of low vitamin D level (OR = 1.55) compared to employed people.
Factors independently related to low vitamin D, using multivariate logistic regression analysis.
Discussion
The prevalence of vitamin D deficiency is alarming high globally. 20 Previous studies in Jordan revealed various rates of vitamin D deficiency.17,18,21 In this study, 89.7% of Jordanian adults had low vitamin D level (25(OH)D < 30 ng/mL). Nichols et al. 21 reported that 60.3% of non-pregnant women of childbearing age were vitamin D deficient. This estimate was much higher than what had been reported by Batieha et al. 17 in a previous national study who reported a prevalence of 37.3% in females and 5.1% in males.
It is well-known that many methods have been developed by several companies to measure 25(OH)D levels in serum or plasma. Numerous publications have shown the limitations of these methods, with notable variations in vitamin D determination by using these different assays.22,23 The differences in the measurements of 25(OH)D levels because of using different assays might explain the variations in the prevalence rates. To investigate the differences in the findings of this study and the findings of a previous national study by Batieha et al., 17 we re-measured the level of vitamin D in 1000 stored samples from Batieha et al. 17 study using Abbott reagents (Abbott Laboratories) instead of the previously used radioimmunoassay (RIA). We found that 91% of the study group had low vitamin D level.
Moreover, high prevalence rates of low vitamin D were reported in other countries of the region including Lebanon, 44%; 8 Syria, 90.1%; 9 Saudi Arabia, 83.6%; 10 Qatar, 90.4%; 11 Morocco, 91%; 12 Tunisia, 47.6%; 13 and Egypt, 60%. 14
The main factors that were significantly associated with low level of vitamin D in the multivariate analysis in our study were gender, age, obesity, and employment. Vitamin D deficiency and insufficiency affected all age groups in this study. Females were twice more likely than men to have low level of vitamin D. Although Jordan is a sunny country almost all of the year, the high rate among females might be explained by that they are not receiving enough exposure to sun because of their dressing style. In this study, 95% of women were either veiled, wearing the niqab (which covers the whole body including the face and hands), or wearing the hijab (which covers the whole body but spares the face and hands). The finding of a higher prevalence of low vitamin D status in women wearing the niqab or hijab compared to women wearing Western dress styles is consistent with previous studies.17,18 The prevalence of hypovitaminosis reported by Mishal 18 study was 31% in Western-dressed women, 55% in women wearing the hijab, and 83% in women wearing the niqab.
The findings of our study supported the association between obesity and low vitamin D levels. Previous studies showed that obesity was associated with lower serum 25(OH)D concentrations.24,25 However, the mechanism explaining this association is not fully described. One possible explanation is that people with obesity are less likely to participate in outdoor activities and more likely to cover-up and wear more clothing than leaner individuals, thus decreasing sun exposure and limiting endogenous production of cholecalciferol in the skin.
The link between vitamin D levels and occupation has previously been explored. Low levels of vitamin D have been reported in occupational groups with low exposure to sunlight 26 and high levels were reported among outdoor workers. 27 In our study, unemployment was significantly associated with low vitamin D level. Unemployed people in Jordan, especially women, spend less time outdoors and therefore they are less likely to be exposed to the sun.
The main limitation of this study is inherited in its cross-sectional design. Temporal association and causality cannot be established in cross-sectional studies. Measurement errors in dealing with anthropometric measurements and vitamin D level might affect the study findings. A prospective study is strongly recommended to determine the true risk factor of low vitamin D level.
In conclusion, the prevalence of low vitamin D level is extremely high in Jordan. Age, gender, obesity, and unemployment were associated with low levels of vitamin D. Health authorities in Jordan need to increase the level of awareness about vitamin D deficiency and its prevention, particularly among women.
Footnotes
Author contributions
M.E.-K. wrote the manuscript and contributed to the conception and design of the study. Y.K. contributed to the conception and design of the study and performed the statistical analysis and reviewed the manuscript. A.B. contributed to the conception and design of the study and approved the protocol from the statistical point of view, analyzed the data, and approved the results. H.J. contributed to the conception and design of the study and assisted in analyzing the data. D.H. assisted in collecting data and helped in developing the idea and setting the protocol. N.K. contributed to the conception and design of the study. M.A. contributed to the conception and design of the study, the acquisition of data, and the analysis and interpretation of data. K.A. was the originator of the manuscript subject and supervised the research and writing of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this study that involved human participants were in accordance with the National Center for Diabetes, Endocrinology, and Genetics (NCDEG) Ethics Committee, which is accredited by the National Ethics Committee (ID: 12/2017).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Scientific Research Support Fund, The Ministry of Higher Education.
Informed consent
Written informed consent was obtained from all subjects before the study.