
Abstract
Introduction:
Postpartum depression is a prevalent consequence of childbirth experienced by many women. There has been evidence linking dairy intake during pregnancy with a reduction in postpartum depression symptoms. However, there is still a lack of understanding regarding the effects of postpartum dairy consumption on postpartum depression.
Objectives:
To examine whether dairy products intake and calcium in dairy is associated with postpartum depression.
Methods:
A pilot study was conducted (n = 49 postpartum women). A food frequency questionnaire was used to evaluate the participants’ consumption of calcium and dairy products during pregnancy, and the Edinburgh Postnatal Depression Scale was used to screen for postpartum depression symptoms.
Results:
Of 49 participants, 26 (53%) were at risk for postpartum depression (Edinburgh Postnatal Depression Scale ⩾ 12). Consuming >1 serving of Laban per day is significantly associated with reduced risk of postpartum depression (odds ratio = 0.01, 95% confidence interval [0, 0.3]). Total dairy intake >1 serving per day is significantly associated with reduced risk of postpartum depression (odds ratio = 0.17, 95% confidence interval [0.03, 0.83]). No significant association was found between the postpartum intake of milk, cheese, yogurt, or calcium and postpartum depression.
Conclusion:
Our findings indicate that higher total dairy intake was associated with a lower likelihood of postpartum depression. Further assessment with a larger sample size of participants could provide additional insight into the potential of dietary dairy to mitigate postpartum depression.
Introduction
Highlights
Postpartum depression (PPD) is a prevalent consequence of childbirth experienced by many women. Recent studies in Saudi Arabia have placed the rates of PPD between 25% and 40%.
Several studies have shown that dairy consumption during pregnancy is associated with reduced PPD symptoms. However, dairy intake in the postpartum period has not been studied.
The study evaluated postpartum dietary dairy intake and investigated the associations between several related variables. Our study sheds new light on dietary considerations in postpartum women and their associations with PPD.
Our findings indicate that higher total dairy intake was associated with a lower likelihood of PPD. Further assessment with a larger sample size of participants could provide additional insight into the potential of dietary dairy to mitigate PPD.
Background
PPD is one of the most common conditions seen within the first year after childbirth. 1 Mothers with PPD suffer general depressive disorder symptoms, including low mood, insomnia, loss of appetite, anxiety, crying spells, fatigue, and poor concentration. 2
The prevalence of PPD ranges between 5% and 60% globally.3,4 In Saudi Arabia, the prevalence rate is over 50%. The prevalence rate may be higher than detected in the studies reviewed, as many women may face mental health issues alone and may not report mental issues due to the social expectations surrounding motherhood. 5 If untreated, the consequences of PPD are far-reaching and pose a significant public health concern.
Nutritional factors play an important role in maternal health and mental health. Research reveals the importance of a healthy diet during pregnancy and after birth.6,7 Healthy diet patterns have been associated with a reduction in depression risk during pregnancy. 8 Evidence suggests that the development of PPD might be associated with a deficiency of specific vitamins, such as vitamin D and folate, as well as some minerals, including zinc, iron, and calcium.9,10 However, limited information is available regarding the postpartum intake of a specific food group or nutrients in relation to PPD.
Dairy products are the most effective food group to provide sufficient energy and nutrients to meet mothers’ and fetuses’ high demands during pregnancy and lactation. Dairy products have a high density of nutrients, including protein, vitamin B2, vitamin B12, magnesium, phosphorus, potassium, zinc, and calcium. 11 Calcium deficiency plays a critical role in nervous system disorders, such as depression. 12
Recent research suggests that calcium intake may reduce the risk of noncommunicable diseases such as obesity and metabolic syndrome. This is because calcium intake can lower inflammation by decreasing the levels of certain hormones like parathyroid hormone in the bloodstream. In addition, it regulates the production of inflammatory cytokines. 13
Furthermore, a review mentioned that there is a two-way relationship between bone mineral density and depressive symptoms. Based on this finding, calcium intake may have a beneficial effect on reducing depression as it is a bone health-related factor that helps to maintain bone density. 14
Thus, calcium and calcium-rich dairy products are also gaining attention for their role in depressive symptoms. Some evidence found that perinatal dairy intake of milk, yogurt, and cheese has been associated with PPD symptoms. For example, the risk of PPD symptoms was reported to be higher in the lowest quartile of dairy product intake compared to the group with the highest intake. 15 Another epidemiological study showed a lowered score for depression in the group with a high calcium intake and was independently related to a lower prevalence of depressive symptoms during pregnancy. 16 Nevertheless, the literature is still insufficient regarding the association between postpartum dairy intake and PPD symptoms. Also, postpartum women require an increased amount of nutrients, especially for healing, recovery, and breastfeeding support. Therefore, the aim of this study was to evaluate the postpartum intake of dairy products and calcium in relation to the risks of PPD.
Methods
Study design
A pilot study included participants from all five main regions in Saudi Arabia. The Central Region, Eastern Region Western Region, Southern Region, and Northern Region. The study conducted between December 2020 and April 2021. Ethical approval was obtained from the Unit of Biomedical Research Ethical Committee at King Abdulaziz University (Jeddah, Saudi Arabia) (reference no 84-21). A written informed consent was obtained from all subjects before the study.
Study participants and recruitment
The participants were females aged ⩾18 years, and within the first year after childbirth. The minimum postpartum time of this sample was 3 weeks and the maximum was 1 year. Participants who residing outside of Saudi Arabia and/or with a history of mental illness were excluded from this study.
Study instrument and data collection
A survey platform (SurveyMonkey) was used to create an online questionnaire. The survey link was distributed via email and through various social media platforms (WhatsApp, Twitter). Participants could answer the questionnaire only once. All participants completed the self-administered questionnaire. This survey incorporated questions on demographics, employment, family, pregnancy, health, psychological well-being, and health-related factors; and the food frequency questionnaire (FFQ) and the Edinburgh Postnatal Depression Scale (EPDS) screening tool for identifying depression.
Food Frequency Questionnaire
The FFQ measured the frequency and quantity of intake of dairy products and other food groups and nutrients. An Arabic FFQ adapted from the Saudi Food and Drug Administration was used. 17 This questionnaire has been confirmed for high reliability and validity and can be used in nutritional epidemiological research in Saudi Arabia. There were 133 food items covered in this FFQ using a closed-ended approach. There are nine answer options provided for each closed-ended question, with consumption frequency choices presented as follows: neither ever nor less than once a month, every 1–3 months, once weekly, two to four times weekly, five to six times weekly, once a day, two to three times per day, four to five times a day, or more than six times a day. Also, an open-ended question at the end of the FFQ collects specific information about other food items not listed. The FFQ also includes questions regarding nutritional supplements and probiotic consumption. Nutritional values for the items were derived from the Saudi Food Composition Tables of 1996 and McCance and Widdowson’s Composition of Foods Integrated Dataset for 2015.17,18 Microsoft Excel was used to analyze all intake-related data.
The validity and reliability of the FFQ should be ensured before administering it to the main study population. The FFQ was tested in this pilot study on 49 participants, which represents about 12.5% of the total population. Internal consistency was used to assess the reliability of the scale, and Cronbach’s α coefficient = 0.8.
Edinburgh Postnatal Depression Scale
The EPDS questionnaire was used to screen the participants’ depression levels. 19 In addition to the English version, an Arabic version of the EPDS has been translated and validated. 17 The questionnaire consisted of a 10-item self-report scale assessing the common symptoms of depression. The items were scored on a scale of 0–3; total scores ranged from 0 to 30. 20
A cutoff value of ⩾12 has been found to indicate good sensitivity and specificity in the Arabic language. 21 The researchers therefore considered PPD as an EPDS score of 12 or higher.
Statistical analysis
The statistical analysis was done using IBM SPSS (version 27.0.1.0, New York, NY, USA) statistical software. Categorical variables were expressed as numbers and percentages. Continuous variables were expressed as mean and standard deviation. Chi-square testing was used to test the differences between categorical variables. The association between the variables was assessed by univariate analysis. A p value of <0.05 was considered statistically significant. To examine the association between the intake of milk, cheese, yogurt, Laban, and total dairy products (serving/day), logistic regression analyses were conducted with PPD. Internal consistency was used to assess the reliability of the scale.
Results
Table 1 shows that among the 49 women, 26 (53%) were at risk of PPD. The mean age of the participants was 29.42 ± 5.207 years. The majority were non-smokers (n = 39, 69.6%), with a bachelor’s degree (n = 32, 65.3%) and had one to three children (n = 42, 85.7%). Almost half of the participants had a natural birth (n = 26, 53.1%), were not physically active (n = 25, 51%), breastfed their babies (n = 25, 51%), and were employed (n = 24, 49%); 42% (n = 21) and 34% (n = 17) of participants were normal weight and overweight, respectively. The subjects in this study were all married (n = 49, 100%).
Participant’s characteristics and demographics.

Data are expressed as n (%).
BMI: body mass index; PPD: postpartum depression.
Missing value.
In Table 2, participants with a higher body mass index (BMI) were at an increased risk of PPD (p = 0.031). No significant correlations were noted for other variables, including age, education level, number of children, employment, smoking, physical activity, mode of delivery, and breastfeeding.
The relationship between participants’ variables and PPD.
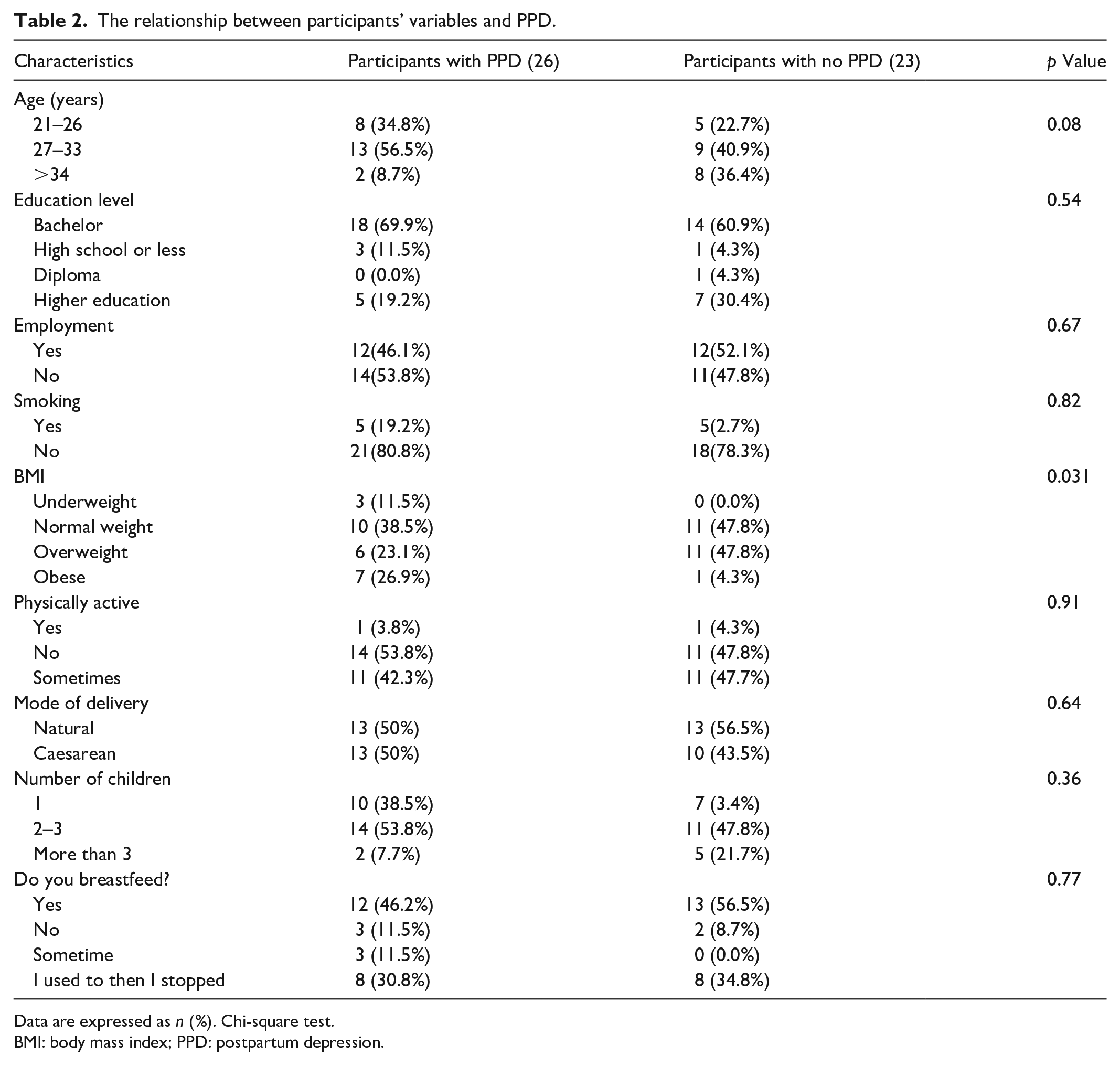
Data are expressed as n (%). Chi-square test.
BMI: body mass index; PPD: postpartum depression.
The associations between dairy intake (servings/day), Ca intake, and PPD were tested in logistic regression models (Table 3). The overall p value of the first model (non-adjusted) is 0.034, while the overall p value of the second model (adjusted) is 0.117. Milk intake >1 serving of milk per day is not significantly associated with PPD (odds ratio (OR) = 2.11, 95% confidence interval (CI) [2.09, 37.3]). Cheese intake >1 serving is not significantly associated with PPD (OR = 2.54, 95% CI [0.39, 16.72]). Consuming >1 serving of yogurt is not significantly associated with PPD (OR = 11.28, 95% CI [0.76, 166.69]). Consuming >1 serving of Laban per day is significantly associated with lower chance of having PPD (OR = 0.01, 95% CI [0, 0.3]). Total dairy intake >1 serving of dairy per day is significantly associated with lower chance of having PPD (OR = 0.17, 95% CI [0.03, 0.83]). Ca daily intake is not significantly associated with PPD (OR = 1, 95% CI [1, 1]).
Logistic regression analysis of diary intake on PPD.
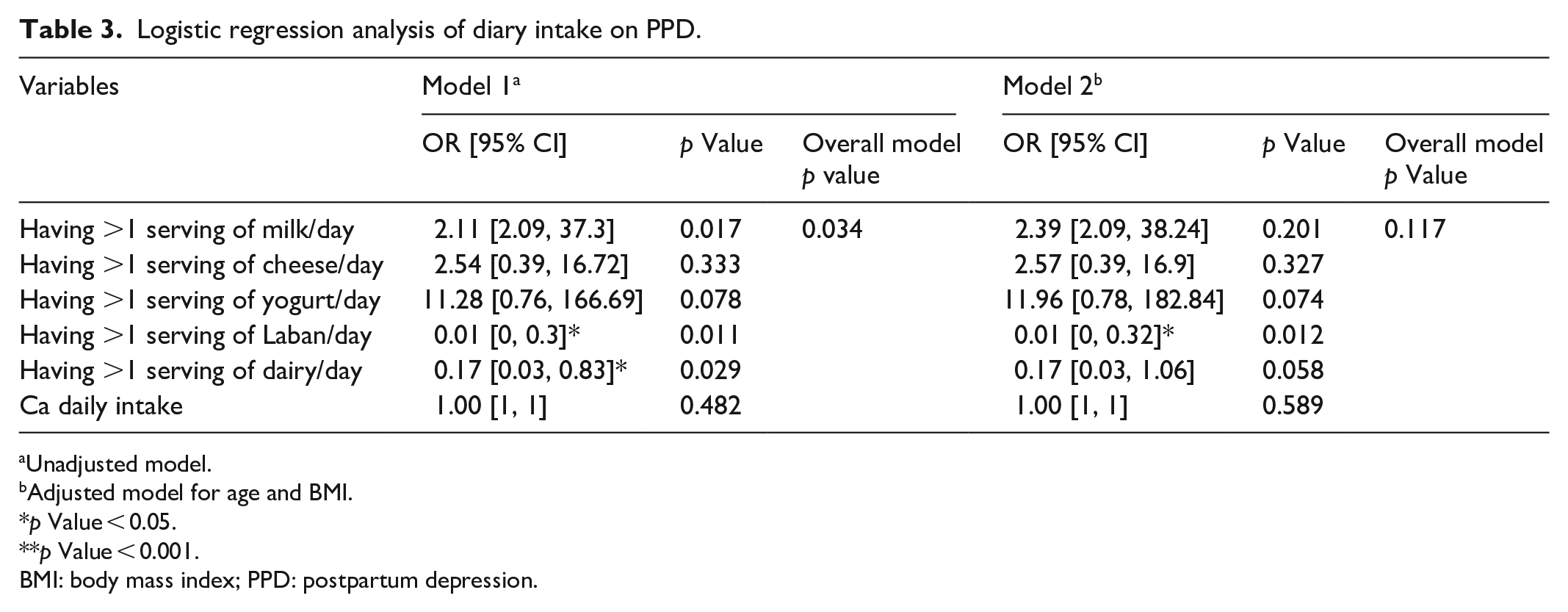
Unadjusted model.
Adjusted model for age and BMI.
p Value < 0.05.
p Value < 0.001.
BMI: body mass index; PPD: postpartum depression.
Discussion
This study evaluated the postpartum consumption of dairy products and calcium and their potential relationship to the risk of PPD. The study also examined the relationship between other variables and PPD, such as age, education level, number of children, employment, smoking, physical activity, mode of delivery, and breastfeeding. In our sample, 53% of the women exhibited symptoms of PPD. A large systematic review estimated that the global prevalence of PPD is greater than previously reported and varies by country. 22 In Saudi Arabia, a prevalence rate of up to 50% has been reported. 5 However, this rate may be an underestimation, as many women may not reveal their struggles to healthcare professionals due to the stigma associated with mental health disorders.
Our findings showed a significant association between total dairy intake of >1 serving per day and a reduced risk of PPD. Furthermore, consuming >1 serving of Laban per day was also associated with lower likelihood of PPD. However, no significant association was found between the postpartum intake of milk, cheese, yogurt, or calcium and PPD. These findings agree with a previous study that suggested that the prepartum intake of a high amount of dairy intake resulted in lowering the risk of PPD. 15 Yet, another study found no effect of prepartum total dairy product intake on the risk of PPD. 23 This inconsistency in results may be due to the different periods of dairy product intake, prepartum versus postpartum, in this study.
This study also found no association between calcium intake and PPD. Similarly, a previous study showed no association between calcium intake levels and depressive symptoms in a large population of 4734 participants. 24 However, one study concluded that a higher intake of micronutrients, such as calcium, magnesium, zinc, and iron, had a positive result in reducing depression symptoms in Japanese mothers. 25 Another study found that dietary calcium intake was higher in a low-risk group than in a high-risk group. 26 Yet, another showed that the prepartum high intake of yogurt and calcium was associated with lowering the prevalence of depressive symptoms over that period, 16 which was not the case in this study.
Although no significant correlations were reported between PPD and other variables, such as age, education level, number of children, employment, smoking, physical activity, mode of delivery, and breastfeeding, we found that PPD was prevalent in mothers with a higher BMI. This could be attributable to psychological (depression) and physiological (weight gain) changes during pregnancy or to the high intake of unhealthy foods. Previously reported, a high level of depression led to the consumption of more unhealthy food and a higher BMI. 27 Furthermore, one study showed that individuals with obesity demonstrated higher levels of depression and anxiety compared to those with a low BMI. 28
The limitations of the study are mainly related to the small sample size. However, we acknowledge that a clear rationale for our chosen sample size was not included in our manuscript. We based our decision on a commonly accepted range for pilot studies of between 12 and 35 participants which is suitable for piloting and would support us testing out the survey tool for use in further research projects.29,30 This study design was also cross-sectional, which may have impacted our ability to draw conclusions regarding causal links. The scoring of the PPD risks was established by a self-administered rating scale (EPDS) and is merely an indication rather than an actual diagnosis determined by a clinician-administered structured diagnostic interview. However, to the best of our knowledge, this is the first study to examine the association between the postpartum dietary intake of dairy products and calcium with PPD.
The results of this study have practical implications. First, early PPD screening for women is important for diagnosing the problem at earlier stages. The importance of providing training in using PPD screening tools, improving healthcare professionals’ understanding of PPD, providing options for referrals, and therapy and treatment, in addition to usual pharmacological treatments. Collaboration with other specialties, such as nutrition specialists, health coaching, and lactation counseling, may also be beneficial.
To confirm the relationship between the dietary intake of dairy products and the risk of PPD, larger-scale studies are required. In addition, extending the current findings by examining the association between PPD and socioeconomic factors would be useful for future research.
Conclusion
Our findings indicate that higher total dairy intake was associated with a lower likelihood of PPD. This study showed that the risks of PPD were higher in women with a higher BMI. Further studies with a larger sample size are required to further explore the relationship between dietary dairy and calcium intake and PPD. Further research on the association between diet and PPD is necessary to support healthcare professionals in their provision of care for women postpartum and to reduce the risks of PPD.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231187756 – Supplemental material for Dairy products intake and the risk of postpartum depression among mothers: A pilot study
Supplemental material, sj-docx-1-smo-10.1177_20503121231187756 for Dairy products intake and the risk of postpartum depression among mothers: A pilot study by Arwa S Almasaudi, Shoug Alashmali, Baian A Baattaiah, Haya S Zedan, Majid Alkhalaf, Salma Omran, Aseel Alghamdi and Aseel Khodary in SAGE Open Medicine
Footnotes
Author contributions
All authors contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent statements
Written informed consent was obtained from all participants before starting the survey. Ethical approval was obtained from the Unit of Biomedical Research Ethical Committee at King Abdulaziz University (Jeddah, Saudi Arabia) (reference no 84-21).
Informed consent
A written informed consent was obtained from all subjects before the study. The informed consent was approved by the Unit of Biomedical Research Ethical Committee at King Abdulaziz University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.