
Abstract
Background:
Intimate partner violence during pregnancy is a strong predictor of maternal postpartum depression. In Ethiopia, evidence on the association of intimate partner violence during pregnancy with postpartum depression is very limited. To design appropriate intervention, it is thus important to understand how postpartum depression varies as a function of the type and severity of intimate partner violence victimization during pregnancy. The aim of this study is to explore the association of different types of intimate partner violence during pregnancy and its severity with postpartum depression in Eastern Ethiopia.
Method:
A community-based cross-sectional study was conducted from January to October 2018. The study included a sample of 3015 postpartum women residing in Eastern Ethiopia. The cutoff point for postpartum depression was defined as ⩾13 points according to the Edinburgh Postnatal Depression Scale. The prevalence ratio with 95% confidence intervals was calculated, and the association between the main predictor (i.e. intimate partner violence during pregnancy) and the outcome variable (postpartum depression) was determined using log binomial regression model.
Results:
16.3% (95% confidence interval: 14.9–17.7) of women experienced postpartum depression. After controlling potential confounding factors, the prevalence of postpartum depression among women exposed to severe physical intimate partner violence during pregnancy was 1.98 times higher as compared to those not exposed to physical intimate partner violence during pregnancy (adjusted prevalence ratio = 1.98; 95% confidence interval: 1.53–2.54). Exposure to psychological intimate partner violence during pregnancy was found to increase the prevalence of postpartum depression by 1.79 as compared to non-exposure to psychological intimate partner violence during pregnancy (adjusted prevalence ratio = 1.79; 95% confidence interval: 1.48–2.18).
Conclusion:
The study provides evidence that psychological and severe physical intimate partner violence during pregnancy were significantly associated with maternal postpartum depression. Screening of pregnant women for intimate partner violence and providing them the necessary support can minimize the risk to postpartum depression.
Introduction
Women are more predisposed to mood disorders around time of pregnancy and after childbirth than any time in their lives. Particularly, postpartum period is known to be high time of risk for the development of depression. 1 Postpartum depression (PPD) is a form of mental disorder that is characterized by a range of depressive symptoms including disturbances of sleep, a reduced concentration and appetite loss as well as an overwhelmed feeling of worthlessness and unreasoned sadness. 2 Approximately, 10%–20% of women experience depression either during pregnancy or in the first 12-month postpartum with highest burden of share from developing countries. 3
Available evidences indicate that pregnant women who are victims of intimate partner violence (IPV) suffer higher levels of depression in the pregnancy 4 and/or during the postpartum.5–8 Particularly, women who are exposed to multiple forms of intimate partner violence during pregnancy (IPVP; physical, sexual and/or psychological), 5 and who have been victimized severely and frequently 8 are at a greater risk for PPD.
The quality of life of mothers is immensely affected by the experience of PPD and the impact is more severe for new mothers. 9 PPD has been associated with poor parenting such as child abuse and neglect, 10 poor self-esteem and social interactions, 11 engagement in risky behavior such as smoking, heavy drinking and unsafe sex 12 as well as self-harm, suicidal ideation and attempts. 13 Early-onset postpartum depressive symptoms may also influence infant feeding modes because of difficulty in interpreting hunger and distress cues from the infant.14,15 Conversely, inability to initiate breast feeding has also been associated with early-onset of PPD due to feeling of inadequacy and self-blame. 16
Studies of PPD in Ethiopia are few,17–19 especially in rural settings. Previous studies were also limited by their small sample size and the failure to consider important potential risk factors and/or confounders. While many of these studies have examined the socio-demographic, reproductive and psychosocial aspects of PPD, no study has so far explored association of IPVP with PPD. Therefore, the aim of this study is to examine the association of different forms of IPVP (psychological, physical, sexual violence and controlling behavior during pregnancy) and its severity with maternal PPD in Eastern Ethiopia.
Methods
Study design and setting
The design of the study was cross-sectional. The study was conducted among communities of Eastern Ethiopia living in town of Harar and Kersa district under the Harar and Kersa Health and Demographic Surveillance System (HDSS), respectively. The total inhabitants of the Kersa HDSS have been estimated to be 127,000 living in 24 kebeles (smallest administrative unit in Ethiopia) whereas the Harar HDSS has 12 kebeles with an estimated 56,000 inhabitants. The major sources of living for the study area communities are trading and farming. Khat (Catha edulis), stimulant green leaf, chewing is prevalent in the study area. 20
In the town of Harar, there are 7 hospitals, 4 health centers and 35 clinics. Two hospitals of the town, namely, the Hiwot Fana Specialized University Hospital (HFSUH) and the Jugal General Hospital (JGH), are currently providing mental health care services for its residents and the surrounding, including the nearby Kersa district community. The HFSUH has a psychiatry unit that serves general cases of mental health patients; most treated cases in the unit being psychosis (schizophrenia) and mood disorders including depression and bipolar disorders. These services are currently provided by six psychiatry nurses, three integrated community and clinical mental health specialists and one general psychologist. The JGH provides outpatient department (OPD) services for chronic cases by a psychiatric nurse. In both HFSUH and JGH, the maternal mental health care is not integrated in the antenatal care (ANC) services (personal communication). The study was conducted between January 2018 and October 2018.
Population and sample
New mothers living under the Kersa and Harar HDSS sites were the target population. Married women (formally or informally) age 15–49 years who were living together with the husband/partner at least during the index pregnancy, and who were in the sixth week of giving live birth were eligible for the study. These inclusion criteria were used to determine the women’s experience of IPV during the pregnancy from the father of the index child. Women who were not permanently residing (i.e. lived for less than 6 months) in either Kersa or Harar HDSS study sites were not considered/excluded from the study.
Sample size was determined using the formula for estimation of a single population proportion with the assumptions of 19% PPD prevalence at sixth week of delivery from a previous study in Northern Ethiopia, 21 with 95.0% level of confidence and a 2.5% margin of error. Final sample of 1042 mothers was considered after allowances of 10% for non-response. However, as the study was conducted being part of another large-scale study that examined the association between IPVP and neonatal mortality on same study sample of 3015 mothers, we enrolled all these samples (n = 3015) even though it was more than the size of the sample we calculated for the study. The sample recruitment and procedures have been described in detail previously in Ashenafi et al. 22
Data collection
For the data collection activity, 36 data collectors and three supervisors were involved. All the data collectors and supervisors were recruited from the HDSS sites; they all had secondary and above education and were given training for consecutive 7 days. The survey involved face-to-face interviewing using a well-structured questionnaire that contains socio-demographic, obstetric history, maternal depression and breastfeeding as well as experiences of violence and related questions. The IPV questions were adopted from the World Health Organization (WHO) multi-country study tool on violence against women (VAW) which has been validated and used in previous study in Ethiopia. 23 The questionnaire also contains the Edinburgh Postpartum Depression Scale (EPDS) for the assessment of maternal PPD 24 which has also been validated in Ethiopia previously. 25
Initially, the questionnaire was prepared in English and then translated to the local languages, Afaan Oromo and Amharic, by fluent speakers of the languages and again back translated to English by another person to check its consistency. The instrument was pre-tested in a nearby village on 5% of the sample size and necessary amendments were made based on the pre-test comments. In order to use as quick reference in the fieldwork, the WHO’s fieldwork manual for VAW study was adapted. 26
Ethical approval
The Haramaya University Institutional Research Ethics Review Committee approved the study (approval reference no. IHRERC/153/2017). According to the WHO ethical safety guideline for VAW study, 27 the household of the eligible study participant was first introduced the research as maternal health and general life experience study. However, after the household members’ consent/willingness has been acquired, the specific nature of the study was then personally introduced to the study eligible woman through the participant information sheet. Then, before the actual interview proceeded, a written informed consent was obtained from the participants. For minor participants (age <18 years), the informed consent was obtained from their parents or legal guardians, and an additional assent was acquired from the minors. The participation was with complete voluntary. The interview was conducted in a strict private space with the aim of protecting the safety of participants. Confidentiality was maintained using unique code in the questionnaire and avoiding any personal information identifiers on the questionnaire.
In case when women needed or requested assistance related to their experience of IPV and/or depression, data collectors and supervisors were trained to encourage the women to contact consulting services in a nearby health facility or the local social service institution (particularly, the local Women and Children’s Affairs office). However, no such need of support or taking up of the referral offer was reported from the participants.
Variables and measurement
Outcome variable
PPD was the outcome of the study and it was measured using EPDS that contains 10 items/questions with each question having 0–3 scored response categories. The EPDS total score ranges from 0 to 30 and a higher score reflects the women’s higher depressed mood. 24 Using a cutoff score ⩾13 on EPDS as a standard to define PPD,24,28 the study participant women have been classified as non-depressed (score <13, coded as “0”) and depressed (score ⩾13, coded as “1”).
Exposure to IPVP
The main explanatory variable of interest was the different types of IPV against women (i.e. psychological, physical and sexual violence as well as partner controlling behavior) that happened during pregnancy. For this study, “intimate partner” denotes the biological father of the study participant’s index child who has been partnered with the participant at least during the index pregnancy.
The psychological IPVP was considered to happen when the respondent answers “yes” to at least one of the following four questions: (1) being insulted or made her feel bad about herself; (2) having been humiliated in front of others; (3) being scared/intimidated on purpose; and (4) having been threatened to hurt her or someone close to her. Experience of at least one of the following violent acts constituted the sexual IPVP: (1) physically forced to have sex; (2) having sex out of fear of what the partner might do; and (3) forced to have sex that she considered degrading. Experiencing any of the following six acts defined the physical IPVP: (1) being pushed or object thrown at her; (2) being slapped; (3) being hit with a fist or punched; (4) having been kicked or dragged; (5) being choked or burnt intentionally; and (6) being threatened or attacked with weapon (a knife and gun). Overall, women who responded “yes” to at least one of the above 13 questions were considered as having “experienced overall IPVP,” and women who answered “no” to all of the questions were considered as “no violence experienced.” Based on the WHO violence severity scale, we labeled the violence act as moderate if the husband/partner slapped the woman or pushed her during the pregnancy. In other words, the physical violence was labeled as “moderate” if only one or both of the first two items of the mentioned six physical violence acts happened to the woman. Whereas, experiencing any one of the rest four acts (i.e. items 3–6 of the above-mentioned physical violence) was labeled as “severe” physical violence. 23
Women were also asked about the experience of partner controlling behaviors. The items constituting these behaviors included as follows: (1) whether the partner has attempted to limit the woman’s contact with her family; (2) if he does not permit her from seeing her friends; (3) whether he insists on knowing where she was all the time; (4) if he constantly ignores her or treats her indifferently; (5) if he expects her seeking permission to get health care for herself; (6) if he often accuses her for being unfaithful; and (7) whether he gets angry if she talks to another male. If the woman reported one or more of these acts during the index pregnancy, then she is considered experiencing controlling behavior from her husband/partner. 23
Control variables
The study considered a range of socio-demographic, obstetric and reproductive characteristics theoretically and empirically linked with IPVP and PPD.1,4,29–31 The socio-demographics included place of residence, age, working status, education of women and their partner as well as women’s alcohol drinking habits during pregnancy which was categorized as frequent drinker (i.e. drinking every day or almost every day), occasional drinker (i.e. drinking sometimes or rarely) and not drinking alcohol at all.
Household empowerment of women is a composite measure that was derived from the women’s decision-making autonomy and attitudes they hold on wife beating. 32 The household decision-making was determined as who basically decides on the following issues: (1) spending income; (2) getting of health care for the woman; (3) major household purchases; (4) minor or daily household purchases; and (5) visit to relatives. The response options were as follows: (a) respondent alone, (b) respondent and partner, (c) partner alone, and (d) others/someone else. For each question, a code value of “1” was assigned if (a) or (b) was the response from the alternative options, and a value of “0” when the response was (c) or (d).
The women’s attitude regarding wife beating was determined by asking women whether they justified husbands on beating their wives under the following conditions: (1) if she is unable to carry household activities, (2) if she argues with him, (3) if she asks him whether he has another girl friend or wife, (4) if she is barren, and (5) if she refuses to have sex with him. The response category for each of the questions was “Yes” and “No,” and a code value of “0” was assigned if the woman agreed on or justified the husband’s beating but “1” otherwise.
Social support was measured using the Oslo Social Support Scale (OSSS-3),33,34 which contains three questions that addresses (1) the number of people so close to the women that they count when great personal problems happen to them (the response options were: “none,” “1–2,” “3–5” and 5+); (2) the concern that people around the women show in what they do (the response options were: “none,” “little,” “uncertain,” “some” and “a lot”), and (3) how easy the women get help/assistance from neighbors in time of need (the response options were: “very difficult,” “difficult,” “possible,” “easy” and “very easy”). The total score on OSSS-3 ranges from 3 to 14, and women who scored 3–8 was labeled as receiving “poor social support,” 9–11 as receiving “moderate social support” and those with 12–14 scores was considered as having a “strong social support.” 35 The OSSS-3 has been commonly used in prior studies in Ethiopia17,36,37 and in sub-Saharan Africa (SSA) countries.34,38,39
For the information related to obstetric and reproductive characteristics, women were asked whether they attended/received ANC and postnatal care (PNC) or not; the number of times they have been pregnant (3 or fewer, 4–6 and 7 or more); the number of children under 5 years (2 or fewer and 3 or more); whether they experienced death of index child or not; their parity being classified as primiparous and multiparous; place of birth (home or health facility); and gestational ages at birth categorized as pre-term (<37 weeks), term (37–40 weeks) and post-term (>40 weeks).
The information regarding couple’s intentions to the index pregnancy was evaluated by asking the women, “right before you became pregnant, did you want to become pregnant then, did you want to wait until later, did you not want it at all?” The women were also asked the same question about the pregnancy intentions of their husbands/partners. If there was non-match on both partners’ pregnancy intentions, then the couple’s pregnancy intention was considered as “discordant”; the intention was labeled as “concordant” if there was a match in the pregnancy intention of both partners.
Statistical analysis
The data were double entered and cleaned using EpiData Version 3.1 and analyzed using STATA Version 14. A principal component analysis (PCA) was carried out in order to derive the women’s household empowerment index using each of the variables representing women’s decision-making autonomy and their attitude toward wife beating. The PCA yielded three categories of women’s household empowerment: low, medium and high status.
Log binomial regression model was used to examine the association of different IPVP types (and other relevant control variables) with maternal PPD. We first computed a bivariate analysis and variables with p-value ⩽ 0.25 in this analysis were considered candidate for the further multivariable analysis. However, based on the literature, we managed to keep variables such as education of women and social support for the multivariable analysis even though they did not reach p-value ⩽ 0.25.
To examine the influence of IPVP on PPD, we ran series of adjusted multivariable models controlling for relevant confounders. Model I assessed the separate effect of all forms of IPVP on PPD. Then, variables representing the socio-demographic and reproductive characteristics of women were additionally included in Model II. The last model (Model III) ran all the variables in each of the models (Model I and Model II) and other postnatal factors known to be relevant to PPD (i.e. PNC use, breastfeeding initiation and experiencing death of the index child). Multi-collinearity was assessed using the variance inflation factor (VIF). Adjusted prevalence ratio (APR) along with 95% confidence intervals (CIs) was estimated to examine the associations of the explanatory variables and the outcome (PPD) in each of the multivariable models, and p-value < 0.05 was taken as a cutoff point for statistical significance. For model selection, the log-likelihood ratio test and the Akaike and Bayesian information criterion were used. The Pearson chi-square and Hosmer–Lemeshow goodness-of-fit tests were also used to test for model fitness.
Results
Characteristics of study participants
Of the 3015 women who participated in the study, the majority of them, that is, 88.4% were Muslims, 87.9% were housewives and 64.1% had no formal education. The age range of the respondents was 15–44 years with mean value ± standard deviation (SD) of 26.4 ± 5.8 years. Nearly, equal proportions of the women had empowerment status of low, medium and high levels. Very few proportions of the respondents (0.7%) were frequent alcohol drinkers.
Of the study participating women, 11.9% of them reported physical IPVP, of which 7.9% were moderate level whereas 4% were severe level physical violence. Nearly, a quarter of them (24.4%) stated they experienced psychological IPVP and 11% experienced sexual IPVP. Compared to the women’s experience of each type of the IPVP, the overall IPVP was the highest at 30.5%. About two-third of the study participants (59.5%) experienced husband’s controlling behavior (Table 1). In terms of IPVP joint occurrence, the most frequently overlapping occurrence was physical and psychological IPVP (9.3%), followed by psychological and sexual (7.1%) and physical and sexual IPVP (4.6%). The joint occurrence of all types of IPVP was 4.0%. Physical violence was less likely to occur in isolated form (2.1%) when compared to sexual (3.3%) and psychological violence (12.0%; Figure 1).
Socio-demographic characteristics of participants, Eastern Ethiopia, 2018 (n = 3015).

IPVP: intimate partner violence during pregnancy.
Drinking every day or almost every day.
Drinking sometimes or rarely.
Overall IPVP = physical or sexual or psychological IPVP.

Venn diagram illustrating overlaps between varying types of intimate partner violence during pregnancy in Eastern Ethiopia, 2018.
The majority of the women (87.9%) stated they had concordant/agreed intentions with the partner regarding the index pregnancy. Although few of the women (13.6%) utilized the PNC service, comparably high proportion of them (50.1%) had attended the ANC. Most of the mothers had post-term births (69.2%) and were multiparous (76.8%). Few of them were seven or more times pregnant (14.3%) and had three or more children of under 5 years at home (12.2%; Table 2).
Obstetric and reproductive characteristics of study participants in Eastern Ethiopia, 2018 (n = 3015).

ANC: antenatal care; PNC: postnatal care.
The prevalence of PPD was 16.3% (95% CI: 14.9–17.7). The EPDS scores ranged from 0 to 28; 887 (29.4%) of the respondents scored the minimum point of 0 (zero) while only one (0.03%) scored the maximum point of 28. The mean EPDS score for women with PPD was 15.6 (95% CI: 15.4–16.0).
As shown in Figure 2, there is linear relationship between the mean EPDS scores and the overall IPVP score points (which ranges from 0 to 13) fitted for a regression line. The mean EPDS scores among mothers with PPD were the highest for those exposed to physical IPVP (16.7 score points), followed by sexual (16.5 score points), psychological (16.2 score points) and partner’s controlling behavior (15.8 score points). Moreover, the mean EPDS scores among the depressed mothers were higher for those exposed to each type of violence than the non-exposed (Figure 3).

Association between mean EPDS scores and total IPVP scores in Eastern Ethiopia, 2018.

Mean Edinburgh Postnatal Depression Scale (EPDS) scores among depressed mothers according to their exposure to varying forms of intimate partner violence during pregnancy (IPVP) in Eastern Ethiopia, 2018.
In the multivariable analysis, results of model I (i.e. model with only the IPVP variables included) showed PPD was significantly associated with exposure to psychological IPVP (APR = 1.92; 95% CI: 1.58–2.33) and severe physical IPVP (APR = 1.93; 95% CI: 1.52–2.45). However, after adjusting for socio-demographic and other obstetric factors (model II), PPD was significantly reduced for exposure to psychological IPVP (APR = 1.79; 95% CI: 1.48–2.18) and it significantly increased for exposure to the severe physical IPVP (APR = 2.00; 95% CI: 1.56–2.56). In model III (the final joint model), the prevalence of PPD among women who were exposed to psychological IPVP was 1.79 times higher compared to those not exposed to it (APR = 1.79; 95% CI: 1.48–2.18). Similarly, in the final adjusted model, the prevalence of PPD among women who were exposed to severe physical IPVP was 1.98 times higher compared to those not exposed to physical violence (APR = 1.98; 95% CI:1.53–2.54). There was no association between sexual IPVP, moderate physical IPVP and husband’s controlling behaviors with PPD in all the multivariable models (Table 3).
Factors associated with postpartum depression among participants living in Eastern Ethiopia, 2018 (n = 3015).
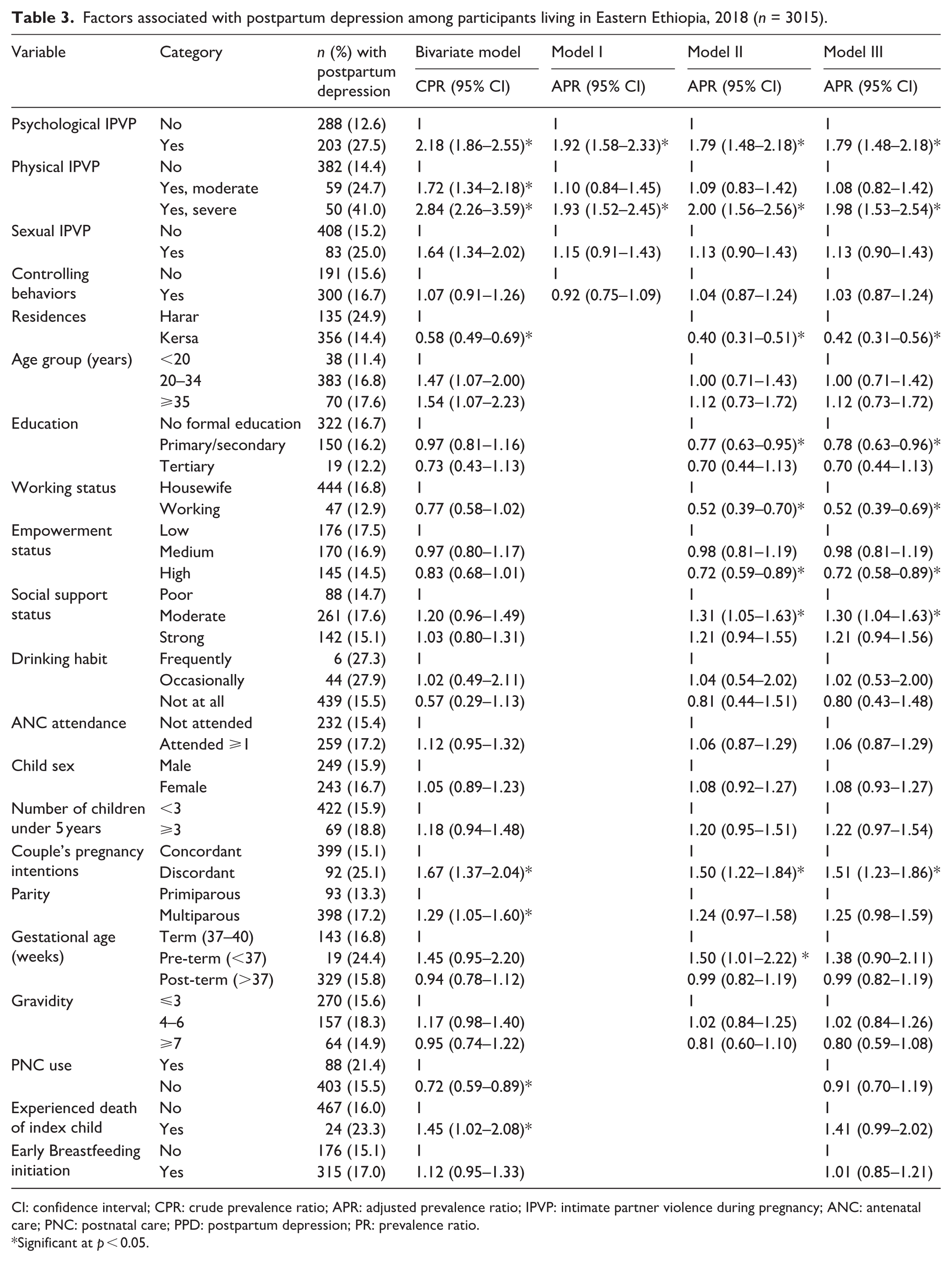
CI: confidence interval; CPR: crude prevalence ratio; APR: adjusted prevalence ratio; IPVP: intimate partner violence during pregnancy; ANC: antenatal care; PNC: postnatal care; PPD: postpartum depression; PR: prevalence ratio.
Significant at p < 0.05.
From the rest of the control variables modeled together, living in Kersa (APR = 0.42; 95% CI: 0.31–0.56), having primary or secondary level education (APR = 0.78; 95% CI: 0.63–0.96), working for cash earnings (APR = 0.52; 95% CI: 0.39–0.69) and having high empowerment status (APR = 0.72; 95% CI: 0.58–0.89) were significantly associated with lower prevalence of PPD. Furthermore, factors significantly associated with higher PPD include receiving moderate social support (APR = 1.30; 95% CI: 1.04–1.63) as opposed to poor support received, and the couple’s discordant pregnancy intentions (APR = 1.51; 95% CI: 1.23–1.86; Table 3).
Discussion
The study showed strong association between psychological and severe physical violence during pregnancy and maternal PPD, after controlling for relevant potential confounders. There was no association between physical IPV which was moderate, the sexual IPV and husband’s controlling behavior during pregnancy with maternal PPD.
Although considerable variations were observed in the studies due to sample size and EPDS cutoff scores differences, the 16.3% PPD prevalence reported in this study was consistent with the most study results in low- and middle-income countries (LMICs)17,40–42 as well as with the rates reported in a recent systematic review in Africa (weighted mean prevalence of 17.8%). 43 In SSA, the prevalence of PPD ranged from 3.8% to 33.5%.18,19,44–46 Higher level of PPD at 34.6% and 50.3% in this region (SSA) was also reported in recent studies in rural communities of Nigeria 47 and South Africa, 48 respectively. In Ethiopia, the social norm which attaches stigma with depression might discourage women to disclose postpartum depressive symptoms they experienced, 18 and this could make PPD less detected or under-reported in the country.
Our finding showing strong association of emotional IPV during pregnancy with maternal PPD is consistent with other studies elsewhere.7,8,41,49–51 The period of pregnancy is a time women often need more emotional support from their husband than ever, 52 and experience of emotional violence from husband against such expectation might lead to feeling of frustration and stress, 53 and to the eventual development of PPD. Women experiencing emotional violence during pregnancy also suffer from low self-esteem and motivational impairment that could contribute to depressive symptoms during the postpartum period. 7
Nearly, twofold increase of PPD associated with severe physical IPVP in our analysis is in agreement with study findings from South Africa, 30 Brazil 7 and Zimbabwe. 8 The reasonable explanation for this association is that women experiencing severe physical aggressions during pregnancy might suffer with intense psychological trauma and physical injuries in the pregnancy and postnatally. 54 Moreover, the physical aggressions usually happen in front of others including family members, close friends or neighbors, resulting a feeling of shame, self-blame and eroded self-belief, 23 making the victim women more viable to PPD symptoms. Abusive husband’s intimidation and physical aggression against female partner in front of relatives, neighbors and friends is a common practice in Ethiopia.55,56
The severe physical abuse during pregnancy strongly associated with PPD in this study is an important finding as literatures largely lack consideration of the severity level of abuse and its association with poor maternal mental health outcome. 4 Few emerging evidences from low-income settings have also confirmed this relationship that violence severity increases the risk of PPD severity.8,30,57
The study did not find association between husband’s controlling behavior and PPD. The plausible explanation might be that regardless of pregnancy status, women in most rural and in some urban Ethiopian community consider husband’s controlling behavior as normal act and sign of affection,56,58 and thus view themselves as not being abused even if in controlled marital relationship. No significant association between sexual violence and PPD in this study could be explained by the contextual meaning of sexual violence, where in traditional community like Ethiopia that condones culturally imposed marital sexual relationship, the sexual violence by intimate partner may not be viewed as abusive act and is considered as a private matter, 59 and not issue of worry. However, the sexual violence might also be under-reported as a result of shame attached to cultural taboos and disfavor related to disclosing sexual issues. 23 The moderate physical violence showing no association with PPD might indicate the abused women’s tolerance of such level of violence to the point it would not affect their mental wellness.
Although our primary interest is exploring association of IPVP with PPD, this study also found some factors that significantly influenced PPD. Our study indicated couple’s discordant intensions in pregnancy contributed for increased PPD, which might suggest the presence of compromised sexual autonomy and/or marital coerced intercourse that might place the victim women for prolonged emotional distress. Moreover, women with unintended pregnancy are psychologically less prepared for parenting and more likely develop PPD. 60
In this study, women’s education, working for cash earning and higher decision autonomy significantly associated with lower prevalence of PPD. It is evident that when mothers are empowered with education and are able to generate their own income, they will have better coping skills with life difficulties including depression, and seek heath care in such difficult situations. 61 Moderate social support being risk factor for PPD in this study, however, need to be taken cautiously as it might also be true that the prior exposure to depression in pregnancy might lead to social isolation and receiving of poor or moderate level social support.
One strength of this study is its being a community-based study conducted in a well-established health and demographic surveillance site. This made identification and follow-up of pregnancy possible in a rural setting of low-income country. Study subjects identified from a community using a well-defined pregnancy identification procedure is believed to minimize possible selection bias, which is more common in studies of facility-based settings. Moreover, the study included large samples of postpartum mothers (n = 3015) in the study area yielding a reasonable estimate of the magnitude of IPVP that can be generalized to similar settings in Ethiopia. We assessed IPVP and other pregnancy-related characteristics from new mothers whose pregnancies had ended very recently, and this is believed to reduce recall bias.
The use of internationally accepted instrument for measuring violence, the WHO VAW tool, is considered as strength of the study. The WHO violence questionnaire is a culturally sensitive instrument validated in Ethiopia and many other countries. 23 The study also used a standard measuring instrument of PPD (i.e. the EPDS tool) 24 which has been previously validated in Ethiopia. 25
The consideration of all types of violence gives the study wider scope to observe which type of violence strongly influenced the outcome of the study (PPD). The severity level of violence considered in this study also shades highlight on the strength of association between IPVP and PPD.
This study used log binomial regression model in estimating the prevalence ratios (PRs) which could help reduce inflation of the observed association that result from use of odds ratio commonly applied in cross-sectional studies. Moreover, the study’s large sample size is believed to yield reasonably precise estimates of the PR with narrow CIs.
The self-report of women on their alcohol drinking habits and experience of sexual IPV during pregnancy might incorporate social desirability bias on their responses due to social disfavor or disapproval of these conditions, and this might lead to underestimating of the observed association. This could be considered as limitation of the study. Nevertheless, the study tried to reduce such bias by employing different measures such as using of only female field staff (i.e. data collectors and supervisors) and securing of information confidentiality.
Although difficult to establish temporal relationship between IPVP and PPD, our findings give an indication of the extent and strength of this association. Nonetheless, we established PPD based on interview response using EPDS tool, not based on clinical diagnosis. Thus, it could be possible that mild cases of PPD could be undetected and under-reported, although the EPDS tool we used has a fairly good sensitivity of 78.9% and specificity of 75.3%. 25
Conclusion
The study provides evidence that emotional/psychological violence and severe physical violence during pregnancy significantly associated with maternal PPD. The strong association between IPV during pregnancy and mothers exhibiting depressive symptoms after birth in the study reinforces the need to screen IPV routinely during pregnancy in an ANC setting or home visits. We recommend future longitudinal research that would warrant inference in the casual link between exposure to varying forms of IPVP and the development of PPD.
Supplemental Material
sj-pdf-1-smo-10.1177_2050312121989493 – Supplemental material for The role of intimate partner violence victimization during pregnancy on maternal postpartum depression in Eastern Ethiopia
Supplemental material, sj-pdf-1-smo-10.1177_2050312121989493 for The role of intimate partner violence victimization during pregnancy on maternal postpartum depression in Eastern Ethiopia by Wondimye Ashenafi, Bezatu Mengistie, Gudina Egata and Yemane Berhane in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the study participants, data collectors and staff of the school of Public Health, College of Health and Medical Sciences for their kind cooperation.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Haramaya University Institutional Research Ethics Review Committee approved the study (approval reference no. IHRERC/153/2017).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Haramaya University. This study also received additional funding and technical support from the African Population and Health Research Center (APHRC) through the African Doctoral Dissertation Research Fellowship (ADDRF) program.
Informed consent
Written informed consent was obtained before administering the survey to the study participants. For minor participants (age <18 years), the informed consent was obtained from their parents or legal guardians, and an additional assent was acquired from the minors.
Data availability
All data analyzed for this article are available with the corresponding author and can be obtained on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.