
Abstract
Objectives:
Cardiovascular disease is a major cause of morbidity and mortality worldwide. Cardiovascular disease was responsible for over 17.9 million deaths in 2016, accounting for 31% of deaths globally and 37% of deaths in Saudi Arabia. With a lifetime risk exceeding 60% for the general population, healthcare professionals are continuously monitoring the health of others but often do not find time to care for themselves. This study aimed to assess the prevalence of cardiovascular risk factors; medical conditions, such as, hypertension and diabetes mellitus; stress; and attitudes and barriers against healthy lifestyle choices among healthcare professionals at King Abdulaziz University Hospital.
Methods:
A cross-sectional study based on a self-administered questionnaire was conducted among the staff at King Abdulaziz University Hospital over a period of 12 weeks. A validated questionnaire was adopted from a study that had previously been conducted in the United Kingdom.
Results:
The study included 400 healthcare workers, of whom, 78% were clinical staff and 22% were non-clinical staff. Approximately, two-thirds of the clinical staff were aged ⩽25 years, whereas 43.2% of the non-clinical staff were aged 26–35 years. Most of the clinical staff (70.5%) were female, compared to 56.8% of the non-clinical staff. Significantly higher rates of hypertension and smoking were observed among the non-clinical staff than among the clinical staff. However, no other significant differences were observed in the prevalence of diseases between the groups. Overall, poor lifestyle, in terms of low compliance with the recommended dietary and physical activity guidelines, was observed in both groups.
Conclusion:
The prevalence of cardiovascular risk factors among the clinical staff at King Abdulaziz University Hospital was not markedly different from that among the non-clinical staff, except the prevalence of hypertension and smoking, which was significantly higher among the non-clinical staff. Further studies that include staff from other institutions are recommended.
Introduction
Cardiovascular diseases (CVDs) are a major cause of morbidity and mortality worldwide. According to the World Health Organization, CVDs were responsible for more than 17.9 million deaths in 2016, representing 31% of all deaths globally and 37% of deaths in Saudi Arabia. 1 Many cases of CVD can be prevented by reducing known risk factors, such as smoking, unhealthy diet, obesity, and physical inactivity. Although the lifetime risk exceeds 60%, 2 healthcare professionals, including both clinical and non-clinical staff, are continually on the lookout for other people’s health, but rarely look after themselves. 3 The awareness and knowledge of risky health behaviors among this group of professionals does not necessarily reflect their health status, yet stress-related disorders are highly prevalent in this group. 4 Thus, the assessment of the prevalence of cardiovascular risk factors, medical conditions and stress, and attitudes and barriers against healthy lifestyle among healthcare professionals at the King Abdulaziz University Hospital (KAUH) is needed.
Saudi Arabia has witnessed a significant economic growth and undergone an epidemiological transition in recent decades. Consequently, a major lifestyle transformation, in terms of poor dietary habits and predominantly sedentary lifestyle, has led to a marked increase in the prevalence of obesity and non-communicable diseases, particularly CVDs. 5 Many studies have documented behavioral risk factors and their association with CVDs among the general population. However, little research has been conducted on the risk among healthcare professionals, particularly in Saudi Arabia.
A study was conducted in the United Kingdom to evaluate the health status and behavioral lifestyle of hospital staff as risk factors for CVD. That study revealed that although many staff members were overweight or obese and did not follow physical activity guidelines, they had a lower prevalence of cardiovascular risk factors than the general population, with no difference between clinical and non-clinical staff. 4 Therefore, this study was conducted to assess the status of cardiovascular risk factors among healthcare professionals in Jeddah in terms of behavior and pre-existing medical conditions and to identify the various factors that contribute to the cardiovascular risk among the clinical and non-clinical staff. Given their increased knowledge of CVD and their role in increasing awareness, early detection, and treatment of disease, the risk of CVD due to behavioral and lifestyle habits among health care professionals is expected to be significantly lower.
Methods
A web-based, cross-sectional study was conducted, based on a self-administered questionnaire, among the staff of KAUH. Both the clinical and non-clinical hospital staff were included in the study.
The sample size obtained for this study was 400 healthcare staff. We determined the minimum sample size using the Roasoft online sample size calculator, taking into account KAUH total staff statistics providing a confidence level of 95% and a margin of error of 5%. All work was conducted with the formal approval of the Institutional Review Board of KAUH, and written informed consent was obtained from all participants prior to their inclusion in the study.
The questionnaire was developed on a web-based platform (www.google.com/forms) to improve ease of completion and collection of data. Ten data collectors circulated the questionnaire on electronic tablets in the hospital on several occasions over a period of 12 weeks from September to November 2018. All staff members were invited to participate in the study, and all eligible staff members (those who consented) were encouraged to respond voluntarily, and those who have not consented were excluded from the study. At the end of this period, the online responses were extracted for analysis.
Survey questionnaire design
A reliable, validated questionnaire was adopted from a study that was previously conducted in the United Kingdom. 4 Permission was officially obtained from the authors to use the questionnaire. The questionanaire used is provided in the supplemental meterial.
The questionnaire was developed to include anonymized data and demographics; no identifiable personal information was collected from the respondents. The survey was sorted into five sections, with each having multiple-choice questions. Section A included respondent demographics: age, gender, job role, and body mass index (BMI). All staff, including doctors, nurses, and medical students, were included in the clinical category; whereas job roles, such as administrator, clerk, housekeepers, and others, were classified as non-clinical. A BMI ⩾ 25 kg/m2 was classified as overweight, whereas BMI ⩾ 30 kg/m2 was classified as obese. In section B, participants were asked about certain risk factors and medical conditions (health checkup, smoking, and any chronic conditions, such as diabetes, hypertension, and high cholesterol). Section C focused on the participants’ dietary habits, whereas section D focused on participants’ leisure and work-related physical activities. The calculated Cronbach’s alpha value was 85%.
Statistical analysis
The collected data were managed and encrypted using Microsoft Excel. Data analysis was then performed using SPSS version 24 (IBM Corp., Armonk, NY, USA). Continuous data were described as means and standard deviations, whereas categorical data were described as percentages and proportions. In the statistical inference, a chi-square test and an independent t-test were used to compare the outcomes of clinical and non-clinical groups. Regarding the perception of work and barriers to a healthy lifestyle, a Likert-type scale was used to assess responses in a ranked fashion.
Results
The study included 400 healthcare workers, 78% and 22% of whom were clinical and non-clinical staff members, respectively.
Demographic characteristics
Approximately, two-thirds of the clinical staff (61.2%) were aged ⩽25 years, whereas 43.2% of the non-clinical staff were aged 26–35 years (Table 1). Most of the clinical staff (70.5%) were female, compared to 56.8% of the non-clinical staff. The majority of participants in both groups were ethnic Saudis (90.7% of the clinical staff and 72.7% of the non-clinical staff). Concerning the job role of the clinical staff, 55.8% were junior physicians and 16.7% were nurses; among the non-clinical staff, 33% were administrative workers/clerks and 26.1% were managers. Most of the participants (70.8% of the clinical staff and 75% of the non-clinical staff) worked in hospitals.
Demographic data of the study participants.

Risk of CVDs
Table 2 summarizes the differences between the clinical and non-clinical staff with regard to the prevalence of diseases that increase the risk of CVDs, the results included are only for those who have these risks confirmed, those who do not know or are uncertain are not included in the following results: The clinical staff tended to be more obese than the non-clinical staff (13.5% vs 5.68%). However, the difference was not statistically significant. The rate of hypertension was significantly higher among the non-clinical staff than among the clinical staff (20.5% vs 9.3%, p = 0.015). The rate of diabetes was higher among the non-clinical staff than among the clinical staff (11.4% vs 6.7%). However, the difference was not statistically significant. The rate of hypercholesterolemia was higher among the non-clinical staff than among the clinical staff (11.4% vs 9%). However, the difference was not statistically significant. The rate of smoking was significantly higher among the non-clinical staff than among the clinical staff (26.1% vs 12.5%, p < 0.001). No statistically significant differences were observed in the rates of other diseases (angina/coronary artery disease, heart attacks, peripheral vascular diseases, stroke, cancer, and musculoskeletal injury) between the clinical and non-clinical staff. The rate of anxiety/depression was higher among the clinical staff than among the non-clinical staff (15.7% vs 9.1%). However, this difference was not statistically significant. A higher proportion of the non-clinical staff desired the facility for cardiovascular health-check at their hospitals compared to that of the clinical staff (71.6% vs 59%, p = 0.022).
Prevalence of cardiovascular risk factors, medical conditions, and stress among the clinical and non-clinical staff.
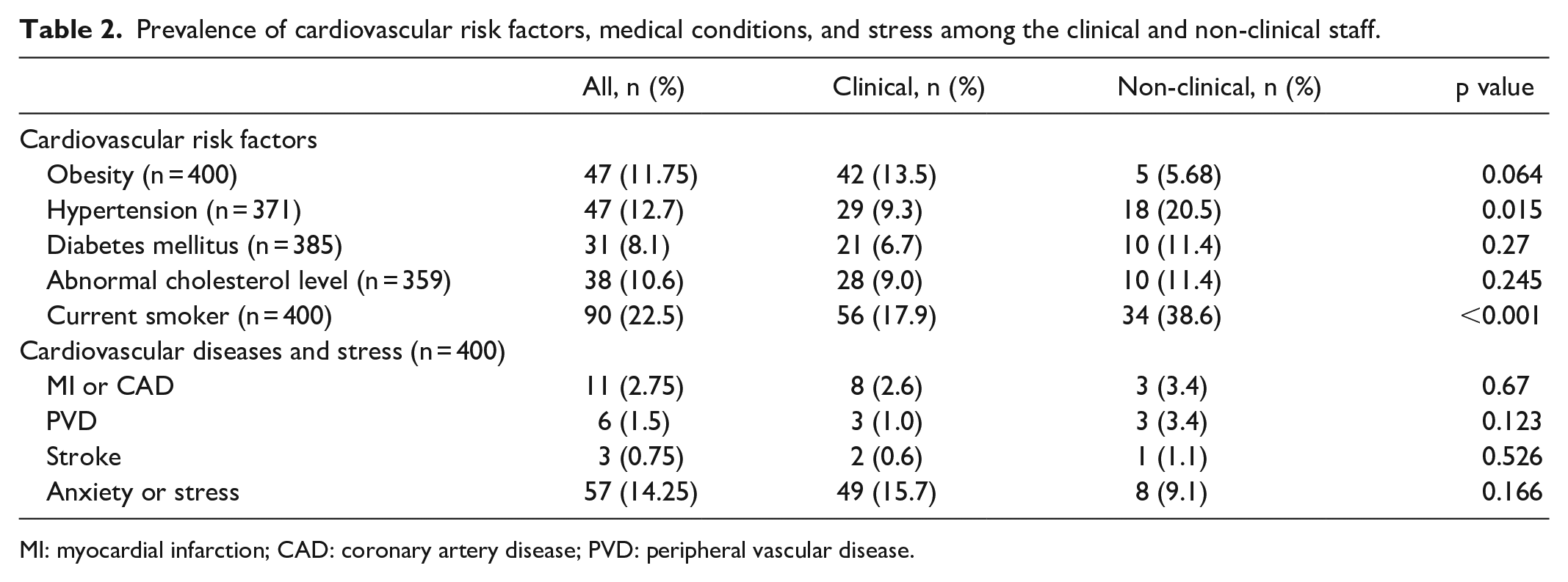
MI: myocardial infarction; CAD: coronary artery disease; PVD: peripheral vascular disease.
Dietary behaviors
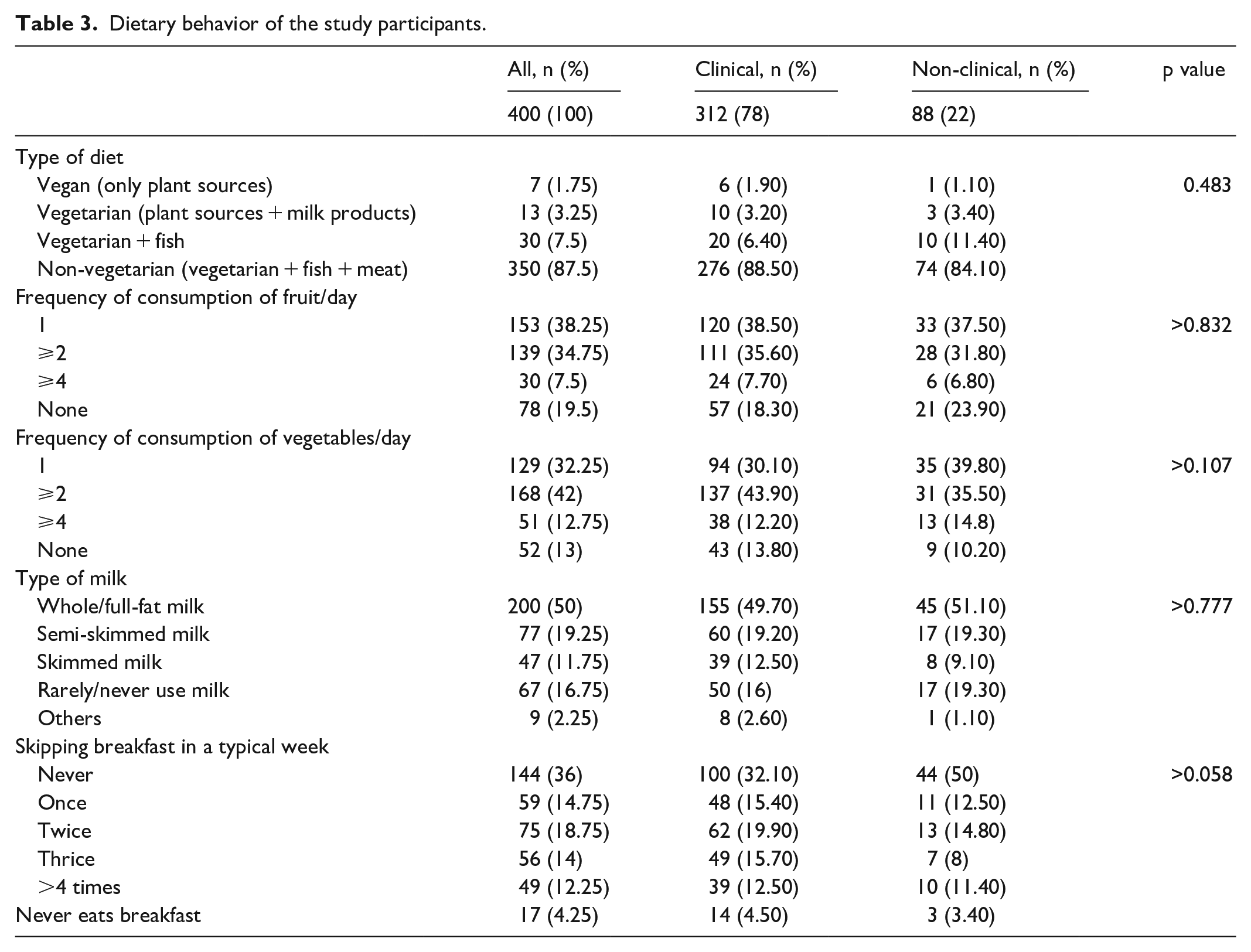
According to Table 3, a majority of the participants in both groups reported eating non-vegetarian diets (88.5% and 84.1% of the clinical and non-clinical staff, respectively), with no significant difference. More than one-third (38.5%) of the clinical staff ate, on an average, one portion of fruit per day, whereas 18.3% never ate fruit, compared to 37.5% and 23.9% among the non-clinical staff, respectively. These differences were not statistically significant. Less than one-third (30.1%) of the clinical staff ate, on an average, one portion of vegetables per day, whereas 13.8% never ate vegetables, compared to 39.9% and 10.2% among the non-clinical staff, respectively. These differences were not statistically significant. Almost half the participants in both groups (49.7% of the clinical staff and 51.1% of the non-clinical staff) drank full-fat milk, whereas 12.5% of the clinical staff and 9.1% of the non-clinical staff drank skimmed milk and 16% of the clinical staff compared to 19.3% of the non-clinical staff rarely or never drank milk. The difference between the two groups in this regard was not significant. Almost one-third of the clinical staff (32.1%), compared to exactly half of the non-clinical staff, never skipped breakfast. This difference was borderline non-significant with a p value of 0.058.
Dietary behavior of the study participants.
Physical activity
As shown in Table 4, 17% of the clinical staff compared to 38.6% of the non-clinical staff described their work as mostly involving sitting at the desk (p < 0.001). History of long-standing illness that limits physical activity was reported more frequently among the non-clinical staff than among the clinical staff (30.7% versus 13.5%, p < 0.001). A total of 138 participants in the clinical staff group (44.2%) compared to 39 (44.3%) in the non-clinical staff group reported engaging in physical exercise beyond that demanded by work, with no significant difference between the groups. A majority of the participants in both groups (93.9% in the clinical staff group and 88.6% in the non-clinical staff group) reached their place of work by car, with no significant difference between the groups. More than half of the clinical staff (51.6%) compared to 62.5% of non-clinical staff were willing to undertake physical activity if facilities were provided at their place of work (p > 0.05). More than half of the clinical staff (51.3%) compared to 58% of the non-clinical staff had not engaged in vigorous physical activity during the preceding 7 days. In addition, 56.4% of the clinical staff (compared to 64.8% of the non-clinical staff) had not engaged in moderate physical activity during the preceding 7 days (p > 0.05). Approximately 40.7% of the clinical staff compared to 55.7% of the non-clinical staff walked for at least 10 minutes at a stretch for >5 days during the preceding 7 days. The difference was borderline significant (p = 0.054). During the preceding week, 6.7% of the clinical staff compared to 17% of the non-clinical staff reported sitting for more than 10 hours/day (p = 0.013). Most of the participants in both groups (74% of the clinical staff and 71.4% of the non-clinical staff) reported being able to perform any exercise to improve muscle strength at least 2 days a week (p > 0.05).
Distribution of the level of physical activity among the study participants.

The reasons given for not engaging in extra physical activities are summarized in Figure 1. The most common reason given by participants in both groups was inadequate time.

Reasons given by participants for not engaging in physical exercise.
Attitude toward health and cardiovascular risk factors
As shown in Table 5, 66.7% of the clinical staff compared to 79.5% of the non-clinical staff either agreed or strongly agreed that they adopted a responsible attitude toward their health and tried to follow general lifestyle advice. More than half of the clinical staff (53.2%) compared to 46.6% of the non-clinical staff either agreed or strongly agreed that their working hours prevented them from staying as fit as they would like to be. Approximately one-third (36.5%) of the clinical staff compared to 40.9% of the non-clinical staff either agreed or strongly agreed that it was not possible to hold down a full-time job and stay fit. In addition, 35.3% of the clinical staff compared to 44.3% of the non-clinical staff either agreed or strongly agreed that they were able to find healthy food options in the hospital cafeteria. Only 16.4% of the clinical staff compared to 36.4% of the non-clinical staff either agreed or strongly agreed that the hospital had sufficient facilities to help them keep fit. Only 22.4% of the clinical staff compared to 39.8% of the non-clinical staff either agreed or strongly agreed that they received support from their manager regarding health and well-being. Less than half of the clinical staff (40.4%) and non-clinical staff (40.9%) either agreed or strongly agreed that they were managers and were aware and understood the health and well-being policy. Overall, no statistically significant difference was observed between the groups regarding the attitudes toward health and cardiovascular risk.
Distribution of attitudes and barriers to health among the study participants.

Discussion
Healthcare providers advise the general public regarding healthy lifestyles as an essential part of their job, in addition to providing treatment. 4 However, the prevalence of lifestyle and cardiovascular risk factors among them is not well known; therefore, this study was conducted to explore the status of cardiovascular risk factors (behavioral and lifestyle-related) among healthcare professionals (clinical and non-clinical staff) in Jeddah, Kingdom of Saudi Arabia.
In this study, 31% of the participants were either overweight or obese. Clinical staff tended to be more obese than non-clinical staff (13.5% versus 5.68%), with no significant difference in this regard between the groups. In a similar study conducted in the United Kingdom, 4 half of the healthcare providers were overweight or obese. In Bahrain, the prevalence of overweight or obesity was 72% among healthcare staff. 6
Concerning compliance with recommended dietary guidelines, a majority of the participants from both clinical and non-clinical groups reported eating non-vegetarian diets. Almost half of them drank full-fat milk and reported a low consumption rate of vegetables and fruit. In addition, almost two-thirds of clinical staff and half of non-clinical staff reported skipping breakfast at various rates. Low compliance with recommended dietary guidelines was also observed among health care workers in the United Kingdom. 4 The poor compliance observed in this study among healthcare workers could reflect that in the general population. In a recent study conducted in Saudi Arabia, only a small percentage of healthcare providers met the dietary recommendations. 7 The poor compliance with dietary recommendations observed in this study could be attributed to personal dietary habits, long working hours, and non-availability of suitable dietary elements at the workplace.
Regarding physical activity in this study, non-clinical staff described their work as mostly involving sitting at the desk at a significantly higher rate than clinical staff. A majority of the participants from both groups used cars to reach their places of work. A considerable proportion of participants in both groups never engaged in vigorous or moderate physical activity; however, they walked for at least 10 min at a time. Low compliance with recommended physical activity guidelines was also reported among healthcare workers in the United Kingdom. 4 However, in a study conducted in Aljouf (Saudi Arabia), almost two-thirds of the primary healthcare physicians engaged in moderate to vigorous physical activity, and only 34.8% were inactive. 8 It is difficult to compare the results of this study to those obtained in the study conducted in Aljouf due to differences in the demographics of the participants in the two studies. Not having enough time was the main reason for not engaging in extra physical activities among members of both groups in this survey. In a similar study conducted in the United Kingdom, the main barriers to physical activity were lack of fitness facilities, not enough time, and lack of support from managers. 4 Lack of time as a barrier to engaging in physical activity was also reported in other studies carried out locally 8 and internationally. 9
It has been documented that poor lifestyle choices, including dietary behavior and physical inactivity, may result in stress among healthcare workers. Conversely, improved lifestyle choices could lead to lowered stress, increased productivity, and better cardiovascular health outcomes, which all result in better quality of care provided to patients.10,11
In this study, the prevalence rates of hypertension and smoking were significantly higher among the non-clinical staff than among the clinical staff. However, no significant differences were observed in the prevalence of other diseases between the groups; similar findings were reported in the United Kingdom. 4 The lower prevalence of smoking among the clinical staff than among the non-clinical staff could be attributed to the implementation of a no-smoking policy in Saudi hospitals in general, as well as the increased perception of the harmful effects of smoking. 12 In this study, the rate of smoking was 12.5% among the clinical staff. This figure is higher than that reported among cardiologists in the United States (1.3%) 13 and clinical staff in the United Kingdom (7.6%). 4 However, it is lower than that reported among cardiologists in Spain (19.5%). 14 On the other hand, the rate of smoking in this study was 26.1% among non-clinical staff, which is higher than that reported among the general population in Saudi Arabia (12.2%) 15 and in the general population of the United Kingdom (20.5%). 16 This figure is alarming and requires further investigation with gender-adjusted models, considering that most of the participants in this study were female.
In this study, the prevalence of diabetes mellitus was 6.7% among the clinical staff and 11.4% among the non-clinical staff, with no significant difference. However, among the general adult population in Saudi Arabia, the rate was 23.9%. 17 In Bahrain, the prevalence of diabetes among physicians was 11%. 6 Other studies reported similar or slightly better patterns of lifestyle and risk factors among healthcare workers than among the general population.13,14,18–20
The prevalence of anxiety/depression/stress in this study was higher among the clinical staff than among the non-clinical staff, but not significantly. This finding is consistent with that of other studies.9,21
This study has three important limitations that must be mentioned. The cross-sectional design used in this study did not allow us to confirm the temporal association between dependent and independent variables. The self-reported nature of the data collected is subject to bias of under- or over-estimation of exposure. Finally, the study was conducted at a single institution, which could affect the generalizability of the results obtained. Despite these limitations, this study is of great public health importance regarding this essential issue.
Conclusion
The prevalence of cardiovascular risk factors among the clinical staff in KAUH, Jeddah, Saudi Arabia, is not markedly different from that found among the non-clinical staff, except for the prevalence of hypertension and smoking. Their attitudes toward good health are acceptable. Further studies that include staff from other institutions are recommended to ensure a comprehensive understanding of the situation.
In this survey, the prevalence of cardiovascular risk factors among the clinical staff at KAUH, Jeddah, Saudi Arabia, was not much different from that found in non-clinical staff, except for those of hypertension and smoking, which were higher among the latter group. Their attitudes toward good health are acceptable. Compliance with dietary and physical activity recommendations was low among both groups, which they attributed to non-availability of suitable dietary elements at the workplace and a lack of time to engage in extra physical activities. A majority of the staff demonstrated responsible attitudes toward their health and tried to follow general lifestyle advice, but they identified lack of time and facilities as the main barriers to maintaining good health.
Supplemental Material
sj-pdf-1-smo-10.1177_2050312120973493 – Supplemental material for Cardiovascular health and lifestyle habits of hospital staff in Jeddah: A cross-sectional survey
Supplemental material, sj-pdf-1-smo-10.1177_2050312120973493 for Cardiovascular health and lifestyle habits of hospital staff in Jeddah: A cross-sectional survey by Ranya Alawy Ghamri, Noor Jamal Baamir and Basma Salah Bamakhrama in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank the staff of KAUH for participating in this survey. They specially thank Tarun Mittal for sharing the survey used in this research and the data collectors, Afnan Alsaif, Ghaida Eissa, Danah Bawazeer, Rafef Derar, Jehan Alsubhi, Ahad Banjar, Remaz Aynousah, Nasrin Shikdar, Raghad Aljondi, and Albatol Alamoodi. They would like to thank Ediatge (![]() ) for English language editing.
) for English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Institutional Review Board of King Abdulaziz University. (Reference No 290-18)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all participants prior to their inclusion in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.