
Abstract
Objective:
Postpartum depression is a common mental illness that affects lactating women. This not only makes daily activities difficult for them, but it also affects child’s future lives. There is little evidence of about postpartum depression and its factors in East African countries, which piqued the authors’ interest in conducting a study on this matter for future decision- and policy-making.
Methods:
The protocol for Preferred Reporting Items for Systematic Reviews and Meta-Analyses was followed. To identify published articles, all major databases such as PubMed/MEDLINE, WHOLIS, Cochrane Library, Embase, PsycINFO, ScienceDirect, Web of Science, and reference lists were used. In addition, shelves, author contact, Google and Google Scholar were also used to identify unpublished studies. Joanna Briggs Institute—Meta-Analysis of Statistical Assessment and Review Instrument was used for critical appraisal of studies. STATA software version 14 was used for the analysis. The random-effect model was used to estimate postpartum depression with 95% confidence interval, while subgroup analysis and meta-regression were used to identify potential sources of heterogeneity and associated factors, respectively. Furthermore, Egger’s test and trim-and-fill analysis were used to check for publication bias.
Results:
Postpartum depression was found in 24% of lactating women in East African countries (95% confidence interval: 17.79–30.20). Postpartum depression was associated with being married (odds ratio = 2; 95% confidence interval: 1.05–3.81), domestic violence (odds ratio = 6.34; 95% confidence interval: 4:11–9.78), a lack of support (odds ratio = 6.59; 95% confidence interval: 1.98–21.89), and a lack of empowerment (odds ratio = 2.79; 95% confidence interval: 1.12–6.92).
Conclusion:
In East Africa, the prevalence of postpartum depression among lactating women is high and rising, as per global postpartum depression estimates. Therefore, the primary focus should be on women’s domestic violence prevention mechanisms. Existing national policies and development agendas must prioritize strategies for women’s support and empowerment. Future research into the relationship between marriage and postpartum depression is required.
Introduction
Postpartum depression (PPD) is an illness that lasts at least 2 weeks and is characterized by persistent sadness and a loss of interest in activities that one normally enjoys, as well as an inability to carry out daily activities. 1 PPD causes extreme sadness, anxiety, and exhaustion in women, making it difficult for them to complete daily care activities for themselves or others. 2
Globally, approximately 13% of women who have recently given birth suffer from a mental disorder, primarily depression. PPD affected 19.8% of women in developing countries. In extreme cases, women’s suffering may even lead to suicide. 1
PPD is a common and serious mental health issue that causes enormous maternal suffering, disability, and devastating effects on a woman’s child, family, and friends. According to studies, the first 6 months after delivery may be a high-risk period for depression. 3
Maternal mental health problems are a major public health challenge worldwide, and they can occur up to 1 year after having a baby, but they most commonly begin about 1–3 weeks after childbirth. 4 It is also a significant issue because it occurs at a time when both the mother and her rapidly developing infant are vulnerable to environmental hazards. 5
Evidence suggests that treating PPD improves newborn growth and development and reduces the likelihood of diarrhea and malnutrition in their children. 1 PPD can also be prevented and treated, but in East African countries, mental disorders are frequently misdiagnosed and undertreated. As a result, the goal of this review was to generate concrete scientific evidence about the prevalence of PPD and its associated factors in East African countries using cross-sectional study design, which will be critical for conducting early measurements.
Methods
Search strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) guideline was followed for our searches. 6 To avoid duplications, databases were searched to see if the same work or ongoing projects were associated with this systematic review and meta-analysis (searched May 2018). However, no review or meta-analysis was conducted on this topic.
All major databases, including PubMed/MEDLINE, WHOLIS, Cochrane Library, Embase, PsycINFO, ScienceDirect, and Web of Science, were used. In addition, reference lists from relevant studies were identified, and full-text articles were reviewed for inclusion.7,8 The key terms used in developing the search strategy were prevalence, magnitude, incidence, PPD, associated factors, related factors, predictors, Ethiopia, Zimbabwe, Uganda, Sudan, Malawi, Kenya, and Eriteria. To search the electronic databases, the key terms were combined with Boolean operators. Furthermore, we used all fields and mesh terms while employing the advanced PubMed searching strategy.
Eligibility criteria
Inclusion criteria
This systematic review and meta-analysis included all studies that determined the prevalence or incidence of PPD and identified its risk factors. East African countries participated in both cross-sectional and cohort studies. This meta-analysis and systematic review were not limited by publication conditions, publication time, or study designs.
Exclusion criteria
We read their titles and abstracts based on the eligibility criteria. We read the full texts of studies that were relevant to our review. Those papers that were not fully accessed at the time of our search were excluded after at least two attempts to contact the principal investigator via email. We excluded these articles because we were unable to assess the quality of each one in the absence of their full texts. Furthermore, after reviewing their full texts, studies that did not report the outcome of interest were excluded. In this systematic review and meta-analysis, studies with low quality after critical appraisal were also excluded.
Data extraction
Data were extracted by eight authors using a standardized data extraction spread sheet. The data extraction spreadsheet was tested on eight randomly selected papers and then modified accordingly. (1) Authors’ name, year, country, study year, and publication year; (2) study design, study setting, study population, sample size, and sampling technique; (3) incidence or prevalence of PPD; (3) data extracted on sex, support (psychological, economic, or spiritual support at the time or after pregnancy), presence or absence of fear, and violence (history of violence against study participants).
Quality assessment
Joanna Briggs Institute 9 —Meta-Analysis of Statistics Assessment and Review Instrument (JBI-MAStARI) was used, which was adapted for both cross-sectional and cohort study designs. Each paper was critically evaluated by four independent reviewers. Disagreements among those reviewers were settled through discussion. If not, two reviewers were involved to resolve inconsistencies between them.
Outcome measurement
The primary finding of this study was PPD. The prevalence of PPD in women in East African countries was calculated by dividing the number of women who experienced PPD by the total number of women who were at risk of developing PPD and multiplying by 100%.
Statistical analysis
The extracted data were entered into the computer using excel sheet and imported to STATA 14 for analysis. The presence of publication bias and heterogeneity was investigated. Begg and Mazumdar’s 10 test with a p value less than 0.05 was used to determine the presence of publication bias. Heterogeneity across studies was assessed using the Cochran Q statistic, with I2 values ranging from 30% to 60%, 50% to 90%, and 75% to 100% indicating moderate, substantial, and significant heterogeneity across individual studies, respectively. 11 A forest plot was also employed to demonstrate the presence of heterogeneity. To declare the presence of heterogeneity across studies, a p value less than 0.05 was also used. Subgroup analysis and meta-regression were used to investigate potential differences between the studies. To estimate the summative effect of PPD and its associated variables, the findings were presented using a forest plot with respective odds ratios (ORs) and 95% confidence intervals (CIs) from a random effects meta-analysis model. The I2 statistics (TAU) were used to quantify the impact of heterogeneity across studies on the meta-analysis, and a cut-off point of 50% was used to declare significant heterogeneity. The odds ratio was used to express the effect size of categorical data.
Measures of effect and reporting
The study selection process was summarized using a PRISMA flow diagram. During the analysis, a random-effect model was used, and odds ratios with 95% confidence intervals were used to present the pooled effect size.
Results
Selection of studies
A total of 251 articles were found using the electronic (246) and supplementary (5) searches, with 36 duplicated articles being excluded. After reviewing the titles and abstracts of the remaining 215 articles, 191 were eliminated. Finally, 24 full-text articles were accessed and evaluated for eligibility criteria. Only 17 articles were included in the final analysis based on the pre-defined criteria and after critical appraisal (Figure 1).

PRISMA flow diagram of included studies to estimate the pooled prevalence of postpartum depression in East African countries from 1998 up to 2018.
Characteristics of included studies
A total of 17 articles were included, with a sample size of 5214 women from East African countries. Between 1998 and 2018, both cross-sectional and cohort studies were included (Table 1). After a thorough search across all East African countries, five articles from Zimbabwe,12–16 four articles from Kenya,17–20 three articles from Uganda,21–23 three articles from Ethiopia,24–26 and the remaining two articles from Sudan27,28 were included.
Characteristics of included studies to estimate the pooled prevalence of postpartum depression and associated factors in East African countries from 1998–2018.

Prevalence of PPD in East African countries
The pooled prevalence of PPD in women in East African countries was 24% (95% CI: 17.79–30.20), as shown in the forest plot below (Figure 2). There was a significant level of statistically significant heterogeneity detected (I2 = 97.2%; p < 0.001), indicating that the use of the random effects model in estimating the pooled estimates is appropriate. The significant magnitude of heterogeneity also suggests the need for subgroup analysis, which necessitates identifying the sources of heterogeneity (Figure 2).
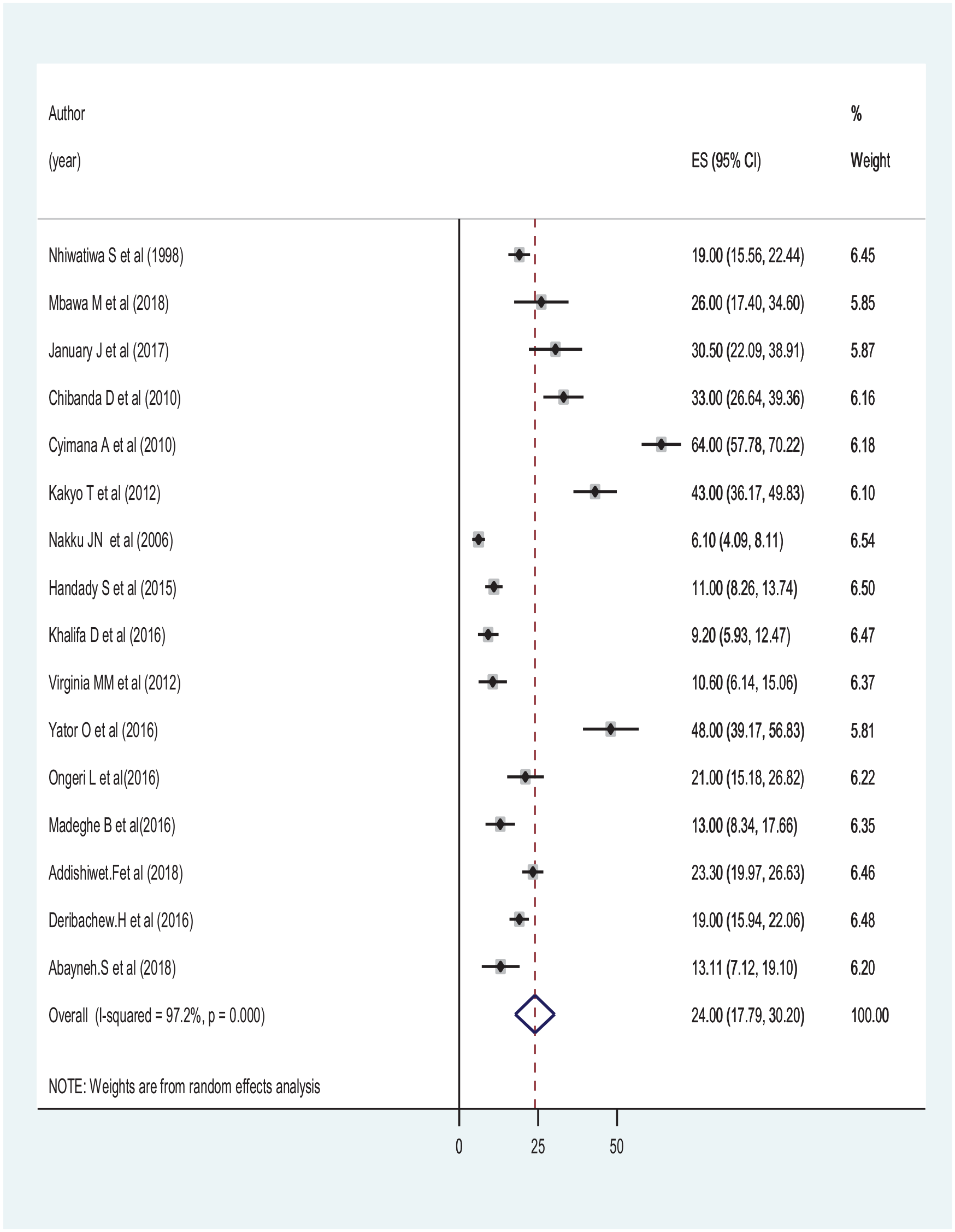
Forest plot showing the pooled prevalence of postpartum depression in East African countries’ women from 1998 up to 2018.
Sensitivity analysis
Prior to performing the subgroup analysis, we conducted sensitivity analysis to identify outlier studies, and any influential studies that had an effect on the overall pooled estimate of this systematic review, and meta-analysis were excluded.
Subgroup analysis
Subgroup analysis based on country was considered as a possible source of heterogeneity across studies (Figure 3). The subgroup analysis, on the contrary, was insignificant. Despite the fact that subgroup analysis could not reduce the level of heterogeneity, significant variation in PPD was observed among women in East African countries (Figure 3). Zimbabwe and Sudan were the most- and least-affected East African countries, accounting for 34.5% and 10.26% of the total, respectively. Furthermore, using Begg and Mazumdar’s 10 and Egger et al.’s 29 tests, publication bias was identified as a source of heterogeneity, and the value was found to be significant at p values of 0.008 and 0.002, respectively.

Forest plot showing subgroup analysis to determine the pooled prevalence of postpartum depression in East African countries’ women from 1998 up to 2018.
To account for the publication bias, a trim and fill meta-analysis was performed. 30 According to this analysis, the prevalence of PPD among women in East African countries was 24 % (95% CI: 17.79–30.20), with no significant difference when compared to the main meta-analysis.
Meta-regression
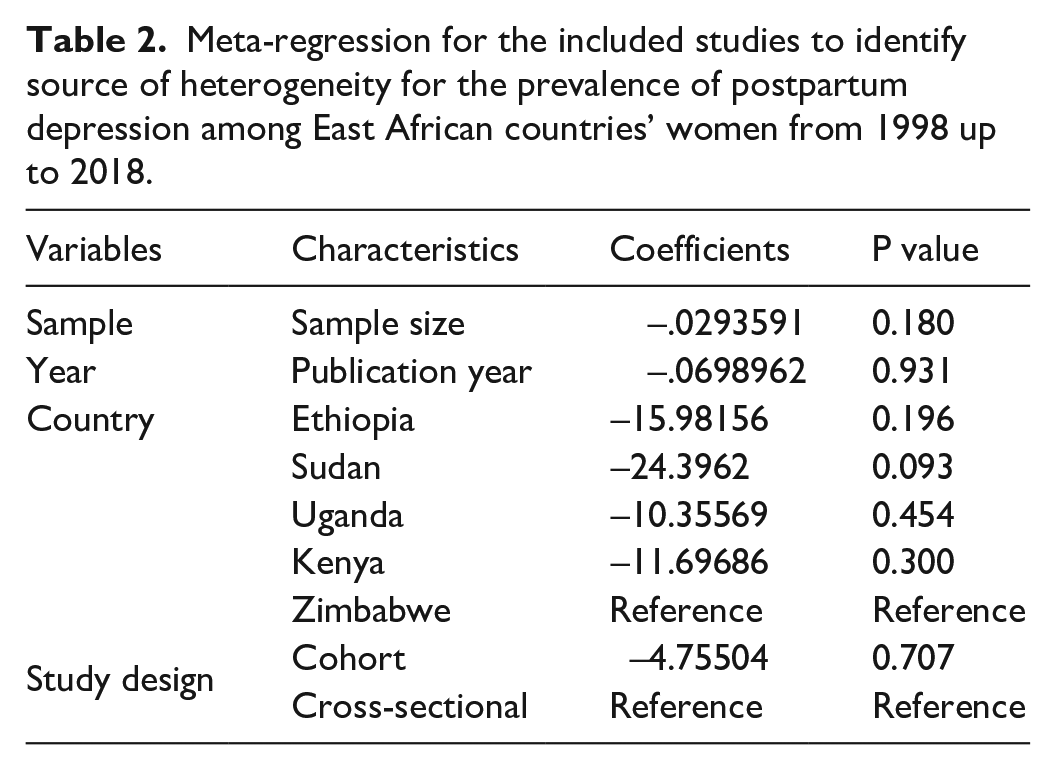
Meta-regression was also used to identify factors associated with the pooled prevalence of PPD across East African countries, using both continuous and categorical data. The meta-regression took into account country, sample size, publication year, and study design for each individual study. However, meta-analysis revealed that the pooled prevalence of PPD across East African countries was unrelated to country, sample size, publication year, or study design (Table 2).
Meta-regression for the included studies to identify source of heterogeneity for the prevalence of postpartum depression among East African countries’ women from 1998 up to 2018.
The associated factors of PPD
Women who gave birth without marriage were twice as likely as those who gave birth with marriage to develop PPD (OR = 2; 95% CI: 1.05–3.81). Women who had experienced violence were six times more likely to develop PPD than women who had not (OR = 6.34; 95% CI: 4.11–9.78). Women who received no social support were six times more likely to develop PPD (OR = 6.59; 95% CI: 1.98–21.89). Women who did not receive empowerment were three times more likely to experience PPD than women who did (OR = 2.79; 95% CI: 1.12–6.92; Figure 4(a)–(d)).

Figure 4(a)–(d): Forest plot which describes associated factors of postpartum depression in East African countries’ women from 1998 up to 2018: (a) marital status and postpartum depression, (b) violence and postpartum depression, (c) support and postpartum depression, and (d) empowerment and postpartum depression.
Discussion
As previously stated, we conducted a systematic review and meta-analysis to obtain the most accurate estimate of the prevalence of PPD among East African women. The overall pooled estimate of PPD was 24%, ranging from 10.26% to 34.5% depending on geographic location. In other developing countries, the prevalence of PPD ranges from 5.2% to 74.0%, according to a similar review. 31 According to this study, Zimbabwe has the highest prevalence of PPD (34.5%). The current systematic review and meta-pooled analysis’s estimate of PPD was lower than a systematic review and meta-analysis focused on depression among outpatient individuals worldwide (27%). 32 This can be explained by the fact that the illness, poor patient-health-care provider relationships, and less-satisfactory medical care may all contribute to a higher prevalence of depression in the outpatient department than this study.33,34 Aside from that both individual characteristics and regional disparities in depression prevalence may have a significant impact. This study focuses on PPD in East African women, whereas the later one looks at the prevalence of depression among outpatients worldwide. The same systematic review and meta-analysis conducted in Iranian women’s (25.3%) revealed a similar result. 35
According to this systematic review and meta-analysis, East African women who did not receive support (any psychological, professional, social, economic, or spiritual support during or after pregnancy), were violated (history of violence during or after pregnancy), were not empowered, and gave birth without marriage were more likely to experience PPD. According to a Chilean study, women who had experienced violence had higher levels of PPD symptoms such as anxiety/insecurity, emotional liability, anger, and mental confusion than women who had not experienced violence.36,37 Another study on Canadian women found a significant link between PPD and intimate partner violence. 38 A similar meta-analysis published in 2012 found violence to be a risk factor for PPD in mothers. 39 A nationwide clinical-based cross-sectional study in Malaysia found a consistent finding between intimate partner violence and PPD. 40 In a study similar to this one, a lack of social support and professional assistance was found to be a risk factor for the occurrence of PPD in mothers living in the Midwestern United States 41 and a recent study reported from Italian women. 42 This review also investigated the fact that women who gave birth without marriage had a higher risk of developing PPD than married women in East African countries, and that this relationship had been established since 2003. 43 Vietnam also reported more consistent findings. 44 This could be attributed to premarital childbirth’s marginalization and social stigma.45,46 However, a surprising finding from the South East Sweden Birth Cohort study (SESBiC) revealed that single mothers did not experience more PPD symptoms than married women. 47 The Swedish government’s increased support for sexual and reproductive health and rights 48 and the presence of continuous support through doulas 46 may both render the relationship between marital status and PPD insignificant.
According to this systematic review and meta-analysis, a lack of any kind of support increases the risk of developing PPD, which is also supported by a British Columbia, 49 Midwestern United States, 41 Taiwan, 50 Turkey, 51 and from China. 52 This finding is not surprising, given that social support from a partner, friend, or other family members may assist mothers in maintaining their quality of life. Women’s empowerment, once again, reduces their chances of developing PPD. A study that investigated the relationship between women’s employment as a means of empowerment and PPD also supported this review. 53 Women’s employment is one method of reducing cultural and social barriers to women’s participation in all aspects of social welfare. Previous research has established a link between cultural restrictions and PPD. 54
Our study has both strengths and limitations. For the quality assessment of individual studies, this systematic review and meta-analysis used internationally accepted tools for critical appraisal. Because no original studies were reported from some East African regional states, the representativeness of this systematic review and meta-analysis may be compromised. Time differences between individual studies, differences in measurement tools, sample size, nature of data collected, and geographic location may all have an impact on the outcome. However, an appropriate statistical model (random effect model) was considered, as well as best statistical estimation approaches such as subgroup analysis and meta-regression, to narrow this limitation.
Conclusion
In East Africa, the prevalence of PPD among lactating women is high and rising, as per global PPD estimates. As a result, the primary focus should be on women’s domestic violence prevention mechanisms. Existing national policies and development agendas must prioritize strategies for women’s support and empowerment. Future research into the relationship between marriage and PPD is required.
Footnotes
Acknowledgements
The authors thank all authors of studies included in this systematic review and meta-analysis.
Author contributions
Y.H., H.T., A.N., T.G., and A.B. developed the protocol and involved in the design, selection of study, data extraction, statistical analysis and developing the initial drafts of the manuscript. Y.H., A.N., and H.T. involved in quality assessment. Y.H., A.N., and A.B. prepared and revising subsequent drafts. Y.H., A.N., T.G., H.T. and A.B. prepared the subsequent and final draft of the manuscript. All authors read and approved the final draft of the manuscript.
Availability of data and material
The data sets analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.