
Abstract
Objective:
To examine medical provider (n = 16) perceptions in addressing and managing pediatric obesity with a diverse, low-income patient population.
Methods:
Semi-structured audio-recorded interviews were performed at three pediatric clinics. Transcripts were reviewed using content analysis and consensus was reached among authors for themes. Themes were grouped into categories including: (1) initiation of weight discussions, (2) advice and perceived effectiveness, and (3) barriers.
Results:
Most providers reported being comfortable addressing weight and use a variety of methods to initiate conversations; however, many challenges were reported, which include limited time and parent misperceptions of child’s weight. A broad range of lifestyle advice was utilized, but preference to discuss physical activity over nutrition was reported.
Conclusion:
Results suggest that successful management of children’s weight involves addressing issues at both the parent and the provider levels. Improved nutrition resources or training for providers is suggested; however, time must also be available for individualized counseling. Incorporation of registered dietitians may also reduce the burden.
Introduction
Childhood obesity has tripled over the last 30 years and is associated with an increased risk of type 2 diabetes, hypertension, hyperlipidemia, sleep apnea, asthma, joint stress, as well as social and psychological issues. 1 The World Health Organization’s 2 Commission on Ending Childhood Obesity reports that the number of infants and young children with obesity increased from 32 million in 1990 to 41 million in 2016 and that it is expected to reach 70 million by 2025 without further improvement in management and prevention. Youth with obesity are likely to mature into adults with obesity and face heart disease, type 2 diabetes, stroke, several types of cancer, and osteoarthritis. 1 Caloric imbalance and environmental factors increase the risk of obesity for all individuals; however, the burden of obesity is not equally distributed. Minority and low-income children are far more likely to be overweight and/or obese.3,4
Pediatric care providers are often first to identify children and adolescents with obesity and are responsible for preventive measures and treatment.4–6 Recommended practices for weight counseling have been examined in other studies with inconsistencies observed between medical providers.7–10 Barriers to initiation of counseling include a variety of factors: limited time with patients, lack of reimbursement, and low patient motivation.7–13 Time constraint during annual examinations has been mentioned in several studies as a barrier for providers when treating obesity because it limits the physicians’ ability to properly follow recommended obesity guidelines.14,15 For example, in a study by Yarborough et al., 15 providers interviewed felt that there was an inadequate amount of time in appointments to properly treat obesity. When physicians discuss weight with children, some studies suggest that parents are most interested in receiving guidance from physicians on healthy diet and lifestyle changes that the family can make as a whole. For example, in a study by Lupi et al., 16 parents reported the need for nutrition guidance including how to get their child to eat well through nutrition advice and meal planning and viewed their pediatricians as a source of such information. Although a variety of constraints on weight counseling have been reported, evidence suggests that failure to address weight may be a source of health care disparity observed among minority and low socioeconomic groups.4,17
There are several barriers to discussing lifestyle changes, with time being one of the most common barriers pediatric and primary care providers report. In addition to this barrier, lack of resources, training, and self-efficacy regarding counseling and/or pediatric obesity management has also been reported.14,15,18,19 Primary care providers have also specifically reported low-to-limited self-efficacy with regard to provision of nutrition information to patients.14,20 A potential cause of low self-efficacy could be related to limited nutrition training during medical school.15,18,19,21 Nutrition is a necessary component of expert committee recommendations regarding the prevention, assessment, and treatment of children and adolescents with obesity. 5 The report outlines counseling areas for providers to address with families and pediatric patients including food intake, eating behaviors, the importance of family interactions around food and meals, and physical activity. 5 A diet that is balanced in macronutrients is recommended, fruits and vegetables should be encouraged and sugar sweetened beverages should be limited. 4 Family meals are also encouraged as it is associated with greater intakes of vegetables, fruits, and milk, as well as lower in soft drinks and fried foods. 4 The role of parents includes modeling healthy diets and portion sizes, as well as encouraging physical activity and limiting screen time. 16 Despite these evidence-based guidelines, obesity rates have remained elevated. The prevalence of children and adolescents with obesity aged 2–19 years old in the United States has stayed around 17% since 2011. 1
Little progress has been made in addressing this national health crisis. Moreover, low-income and minority groups are at increased risk for obesity, and few studies have specifically focused on primary care and pediatric providers working with these groups. The objective of this study was to identify weight management practices and perceptions of medical providers who see a large patient base that includes minority and/or low-income patients. This study examined providers’ approaches, specific advice, and barriers to discussing weight with the families of low-income overweight/obese children.
Methods
Study design
Semi-structured interviews were conducted with medical providers at three community pediatric clinics in a county in central North Carolina between February and March 2012. The clinics were managed under one medical facility and provided primary care services. Questions targeted medical providers including physicians and nurse practitioners. The interview guide was developed specifically for this project. The guide was reviewed by a physician and a registered dietitian (RD) from an on-site Obesity Management Team representing the three clinics (Table 1). Feedback from the physician and RD was used, and the wordings of some questions were modified to appropriately target questions. The Obesity Management physician and RD provided a list of medical providers, and recruitment was conducted by a research assistant on site during clinic hours. Interviews were conducted by the first author (L.R.S.) who at the time was a research assistant (Master’s student) to the last author (L.H.) (both female), with L.H. a nutrition faculty member holding a doctorate. The research assistant conducting the interviews was trained by the principal investigator (PI) and had also conducted a prior literature review on qualitative methodology to prepare for the study. Recruitment continued until a majority of eligible personnel had been invited to participate. All medical staff approached for interviews agreed to participate, and recruitment and interviews continued until saturation of themes was identified. Participants were invited via email or phone to participate in the interviews (contact information provided by Obesity Management Team at the clinics). Incentives were not used in this study. The research assistant who conducted the interviews did not have a prior established relationship with the participants. The participants were aware of the study focus to examine weight management practices at the clinic. Although the research assistant who conducted the interviews is currently an RD, this training and credentialing did not occur until after the study concluded (conclusion of data collection and analysis). Data analysis and results were also reviewed by the third author (K.J.G.) who has expertise in pediatric obesity but is not a nutrition faculty or RD. Interviews were audio-recorded and transcribed verbatim, and content analysis was performed to determine themes. The study was approved by the institutional review board at the principal investigator’s university. Informed consent was obtained prior to all interviews.
Medical providers interview guide.

Site description
At the time of the study, the medical facility operated three clinics that provided primary care pediatric services to primarily low-income patients representing a wide range of ethnicities including a large number of Hispanic patients. Approximately, 56,000+ patients were seen annually. The clinics operated with a mixture of part- and full-time medical staff, a medical director with oversight for the three clinics, an Obesity Management Team, and on-site management. Previous research with this facility revealed 43% of school-aged patients (n = 2951) fell within the overweight and/or obese category. 22 Most patients have Carolina Access (state-subsidized insurance, 73.9%) or Medicaid (13.1%). Approximately, 45.5% of the patients are African American, 28.7% Hispanic, 5% Middle Eastern, 9% Southeast Asian (ethnicity and insurance data from a sample set of n = 600 patients). 23 Cost for visiting a medical provider for annual examinations or weight management varies between types of medical insurance. Cost for uninsured patients is adjusted with a sliding scale for fees based on income.
Medical staff interviews
Interviews were conducted in locations in the clinic selected by the participant. Interviews were private with only the participant and interviewer present and ranged from 10 to 45 min depending on the participants depth of interview responses. Interview questions for physicians and nurse practitioners focused on weight discussions including: age of initiation and comfort level in initiating conversation, strategies for approaching weight, specific counseling advice, perceived patient receptivity, perceived influence and reported frequency of patient behavior changes, and barriers to discussing weight.
Data analysis
Content analysis was used to interpret interview transcriptions. Transcriptions were reviewed by the primary author (L.R.S.) who identified codes. An additional research team member (L.H.) reviewed transcriptions and coding to gain theme consensus. Responses to individual questions per group were summarized using an open-coding process, in which categories were created and transcribed during note-taking as described by Elo and Kyngäs. 24 These categories were reviewed and, in some cases, collapsed into more generalized themes. Identified themes closely tracked interview questions, and the following categories were used to organize the themes: (1) initiation of weight discussions, (2) counseling advice and perceptions, and (3) barriers to weight discussions. Initiation included comfort level, age of patient when weight is first addressed, and specific tools to begin weight conversations. Counseling advice and perceptions included: specific advice given to patients, and perceived receptivity to and influence of counseling. Barriers included all perceived obstacles to discussing weight.
Results
Demographics
Participants (n = 18) included medical providers (n = 16 primarily physicians, some NPs and RDs (n = 2)). In total, 69.6% of medical providers participated in the study and 100% of dietitians on staff. Mean time of employment for medical providers was 7.4 ± 7.5 years. Medical providers included (n = 13) female and (n = 3) male participants. RDs included two female participants.
Provider perceptions
Initiating weight discussions
Most providers were comfortable initiating weight discussions and initiated discussion at or prior to age of 2 years (Table 2). Providers reported a variety of tools and techniques, and some initiated conversations with an open-ended question for parents regarding their child’s weight. Some providers reported the use of motivational interviewing (n = 3).
Initiating weight discussions.

MP: Medical Providers; RD: registered dietitian.
MP includes medical doctors/physicians (MDs) and nurse practitioners (NPs).
Counseling advice and perceptions of patient outcomes
Once the weight status of a patient was approached, lifestyle changes were discussed; the most commonly reported advice focused on physical activity versus nutrition (which was reported by some of the interviewees to be a difficult topic) (Table 3). Counseling efforts were rarely perceived to be successful. Providers perceived parents and the home environment to have the greatest influence on changes over patient behavior (with respect to diet and exercise) (Table 2).
Weight counseling advice, observed changes, and influencing patients.
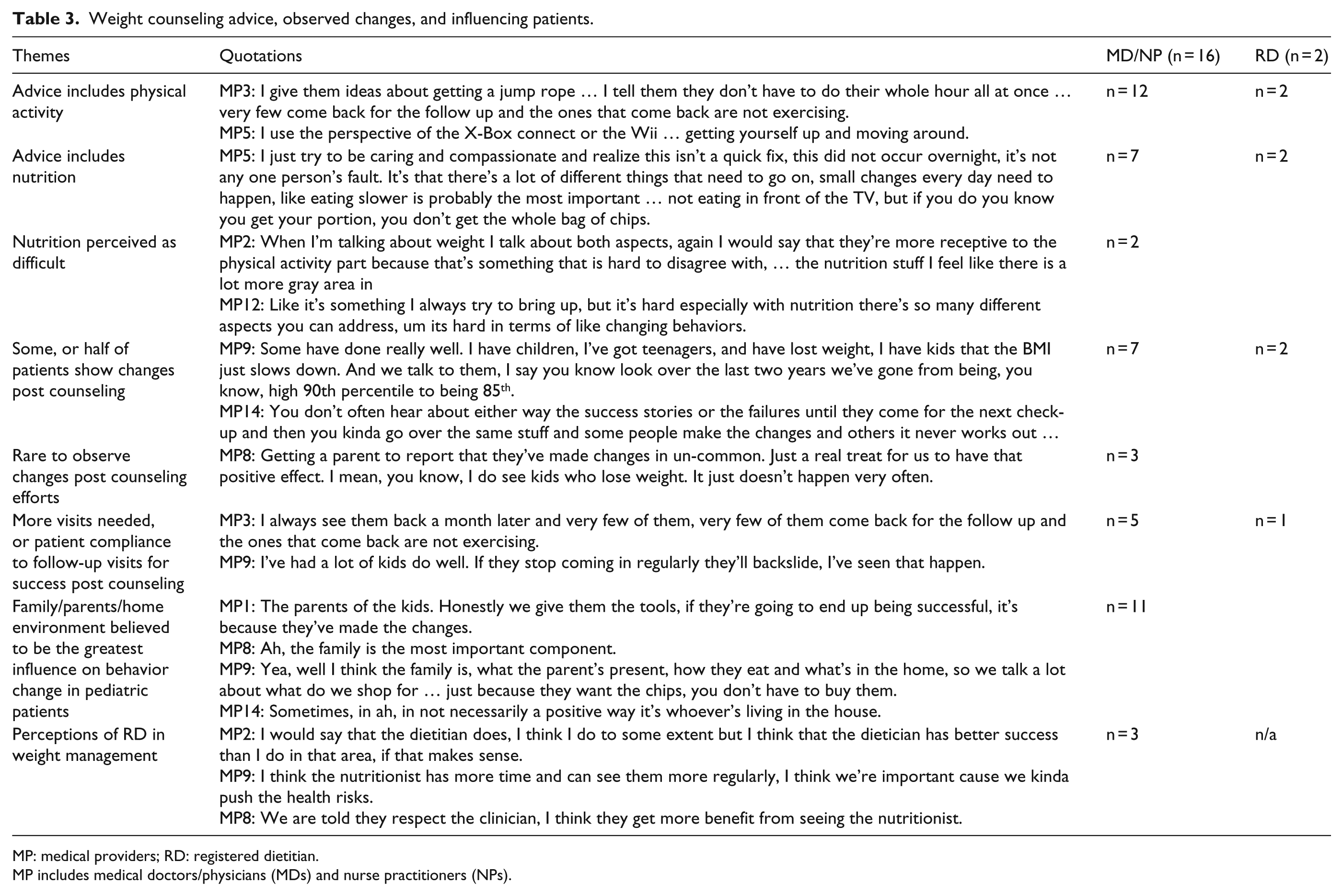
MP: medical providers; RD: registered dietitian.
MP includes medical doctors/physicians (MDs) and nurse practitioners (NPs).
Barriers to discussing weight
A summary of barriers to discussing weight management is reported in Table 4. The most frequently reported barrier affecting weight management discussions involved parental perceptions/support. Lack of time, cultural perceptions of weight, language barriers, and lack of follow-up visits also were noted. Three barriers cited only once (not shown in Table 4) were visit intervals/frequency, insurance status, and lack of patient resources.
Barriers to weight counseling.

MP: medical providers; RD: registered dietitian.
MP includes medical doctors/physicians (MDs) and nurse practitioners (NPs).
Discussion
The lack of progress managing or reducing the pediatric obesity epidemic and the role of primary care providers in prevention and treatment supports the continued need to further investigate weight management practices and perceptions in primary and pediatric care, especially with at-risk (e.g. minority) patient groups. The objective of this study was to examine practices and perceptions of medical providers of addressing and managing obesity with patients and families from diverse, low-income, pediatric clinics.
Providers in this study indicated they begin weight discussions at or prior to age of 2 years following professional guidelines.4,5 Most providers were found to be comfortable discussing weight, which is consistent with findings from Klein et al. (2010); however, some perceived difficulty initiating weight discussions. Weight management discussions were approached with a diverse selection of tools and techniques including body mass index (BMI) charts, open-ended questions regarding parent’s perception of child’s weight, and family risk factors. Once the topic of weight was initiated, counseling typically focused on physical activity, which is consistent with other reported findings.8,13 Nutritional advice, when given, was consistently perceived and reported as a more difficult topic in contrast to physical activity, which was reported as more straightforward and more readily accepted by parents. Several participants reported that this was due to differences in perceptions regarding what is nutritious by patients.
Providers face many barriers to discussing and managing patient’s weight and lifestyle risks, and this study reported rarely observing behavior changes as a result of counseling. Parents are perceived as the primary barrier in weight management discussions. Primary factors affecting this communication include parental weight (overweight), lack of agreement regarding weight and health status, and lack of recognition by parents of what are “healthy” foods and serving sizes. Parental perceptions of their child’s weight status are well-supported in the literature, especially in minority groups represented at this clinic.25–33 Parents in many cultural groups, particularly Hispanic and African American as well as other groups, do not always perceive excess weight as problematic. Some studies have examined parental preferences for weight counseling; however, studies focusing on minority parents are scarce.34,35 The unique perceptions and preferences of diverse cultural groups most at risk (e.g. Hispanics and African Americans) should be further explored to support tailoring/targeting effective counseling approaches and/or nutrition education with these groups by all members of the health care team. Furthermore, cultural context and perceptions with food, weight, and body image supports the need for health care providers to provide culturally relevant information and use culturally sensitive strategies to promote lifestyle changes. Tailored, targeted nutrition education has been found to be the most effective at supporting behavior change, which is necessary to address obesity.36–38
Although parents were identified as a barrier, they were also believed to be the most influential factor in pediatric weight management. Parent-focused interventions have been associated with significant positive behavior changes and/or weight status changes in children, in contrast to child-focused interventions (e.g. a meta-analysis revealed few results and limited longevity of weight/behavior change with child-focused interventions).39–41 The magnitude of the parent’s role in pediatric weight management is also supported by the results of this study.
As previously mentioned, the barriers providers face to effective weight management are high. Consistent with other studies, language, cultural variances in perception of health and weight, and insufficient time were reported as barriers.8,11–13 Time available to cover the necessary components of a medical visit in addition to assessment of nutrition and lifestyle behaviors to provide individualized nutrition education and lifestyle prescriptions is likely to be insufficient. However, to support long-term behavior changes necessary to address weight management (obesity), such individualized or “tailored” approaches that are evidence-based are essential.36–38
From the provider end, additional barriers to effective weight management communication were evident as well. Avoidance of nutrition advice is a clear barrier for successful weight management as both energy intake and energy expenditure are key components to managing weight. Providers in this study reported difficulty with providing nutrition advice, which is concerning because of the hesitancy or avoidance of nutrition education for patients by providers. Yarborough et al. 15 also found that providers reported a lack of confidence regarding nutrition advice. However, in order to meet recommended guidelines for the prevention, management, and treatment of pediatric obesity nutrition must be included in weight management counseling. Improved nutrition training for medical providers has been suggested and could possibly improve prevention, management, and treatment of pediatric obesity.36–38,42 Moreover, improvement of self-efficacy and delivery of nutrition education may meet parental needs and foster a positive patient–provider relationship. For example, there is evidence of parental preferences for individualized nutrition information. In a study by Lupi et al., 16 parents reported interest in receiving weekly meal and nutritional plans from their providers.
RDs are uniquely qualified to help patients with obesity because of their extensive nutrition training and knowledge. Skills RDs possess that are specific to pediatric obesity include knowledge of weight management strategies, along with knowledge of healthy food preparation, assessment of body size and diet, competency in behavioral-science techniques, and knowledge of parents and child-feeding practices that are intended to promote a healthy weight. 43 Furthermore, RDs have physiologic and metabolic training that allows them to assist the health care team in the case that a child is extremely obese. 43 Studies that have investigated the incorporation and/or outcomes of pediatric weight management with care by dietitian have been overall promising. In a study by Bocca et al., 44 outcomes were improved in an intervention program for 3-year-old and 5-year-old children with excess weight or obesity when an RD was included on the multidisciplinary team. Children had a decreased BMI and waist circumference, and their results lasted longer than those receiving usual care. Furthermore, the specific training of dietitians makes them a strong potential health care team in combating the current pediatric obesity epidemic and they may be able to assist in relieving the high burden of obesity prevention, management, and treatment.
Findings from this study explore the experiences of medical providers in weight counseling and management. Study limitations do exist. Due to the time constraints and potential stress level of interviewing during working hours, some feedback may not have been as detailed, or as extensive as desired, although interviews which were shorter usually included participant responses that were brief. Theme saturation was reached during interviews however, the sample size was small. The interview guide used in this study was developed specifically for this project and was not pilot tested prior to this study. Validation primarily focused on face validation from members of the clinic’s Obesity Management Team (which included a physician and an RD). This study investigated perceptions of providers working with a very specific audience at an urban, diverse, low-income pediatric community clinic, and results may not be applicable to other clinical settings; however, disparities and limited research with these patients support the need to examine practices with these groups. Findings were also self-reported experiences and perceptions which have potential for subjective bias. Despite efforts for quality control in the interpretation and analysis of interview transcriptions, there is potential for un-intended bias.
Conclusion
The results of this study suggest that successful management of children’s weight likely involves addressing the issue at two levels: the parent and the provider. At the parent level, this requires that parents understand the risks that being overweight can have on their children’s health and development and that they have a critical role in helping their children manage their weight and general health. At the provider level, the challenge is more complex because it requires health professionals to discuss with parents their child’s nutrition, physical activity levels, sleep patterns, and existing medical conditions and to formulate an individualized or tailored plan for the parent and the child. To achieve success at both levels, open efforts to understand and work together for the common benefit of the child are essential. The results from this study suggest better resources (or training) for primary care providers are needed to support provision of sound and effective nutrition advice. The consistent reporting of time as a major barrier in combination with the above challenges suggests the potential benefit of incorporating dietitians into primary care to assist primary care providers (e.g. physicians and pediatricians) and may be a viable complementary practice in preventing, managing, and treating pediatric obesity. The relatively poor progress made toward preventing, managing, and treating pediatric obesity in our society clearly indicates that new approaches and/or utilization of new resources or collaborations are needed. A good first step would be to enhance pediatric practitioner’s ability to address children with excess weight and/or obesity and to teach parents the importance of good nutrition, physical activity, adequate sleep, and staying informed and engaged with their children’s health and development.
Supplemental Material
COREQ_checklist – Supplemental material for A qualitative study examining medical provider advice, barriers, and perceived effectiveness in addressing childhood obesity to patients and families from a low-income community health clinic
Supplemental material, COREQ_checklist for A qualitative study examining medical provider advice, barriers, and perceived effectiveness in addressing childhood obesity to patients and families from a low-income community health clinic by Lauren R Sastre, Stephanie Matson, Kenneth J Gruber and Lauren Haldeman in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the medical providers at the clinics for their time in participating in the study interviews. The authors also thank the Obesity Management Team for their oversight for this study as well as assistance with participant recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from The University of North Carolina at Greensboro Institutional Review Board (12-0094).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Community-Based Research Grant Program sponsored by the Office for Leadership and Service Learning at The University of North Carolina at Greensboro.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.