
Abstract
Multimorbidity and polypharmacy are increasingly prevalent across healthcare systems and settings as global demographic trends shift towards increased proportions of older people in populations. Numerous studies have demonstrated an association between polypharmacy and potentially inappropriate prescribing (PIP), and have reported high prevalence of PIP across settings of care in Europe and North America and, as a consequence, increased risk of adverse drug reactions, healthcare utilization, morbidity and mortality. These studies have not focused specifically on people with dementia, despite the high risk of adverse drug reactions and PIP in this patient cohort. This narrative review considers the evidence currently available in the area, including studies examining prevalence of PIP in older people with dementia, how appropriateness of prescribing is assessed, the medications most commonly implicated, the clinical consequences, and research priorities to optimize prescribing for this vulnerable patient group. Although there has been a considerable research effort to develop criteria to assess medication appropriateness in older people in recent years, the majority of tools do not focus on people with dementia. Of the limited number of tools available, most focus on the advanced stages of dementia in which life expectancy is limited. The development of tools to assess medication appropriateness in people with mild to moderate dementia or across the full spectrum of disease severity represents an important gap in the research literature and is beginning to attract research interest, with recent studies considering the medication regimen as a whole, or misprescribing, overprescribing or underprescribing of certain medications/medication classes, including anticholinergics, psychotropics, antibiotics and analgesics. Further work is required in development and validation of criteria to assess prescribing appropriateness in this vulnerable patient population, to determine prevalence of PIP in large cohorts of people with the full spectrum of dementia variants and severities, and to examine the impact of PIP on health outcomes.
Keywords
Introduction
The world’s population is ageing at an increasingly dramatic rate as fertility rates fall and people in high-, middle- and low-income countries are living longer [World Health Organization, 2015]. Multimorbidity, commonly defined as the presence of two or more chronic medical conditions [World Health Organization, 2015] and, as a consequence, polypharmacy (the prescribing of multiple medications) are increasingly prevalent across healthcare systems and settings in most developed countries [Cadogan et al. 2016] as demographic trends shift towards increased proportions of older people in their populations. Coupled with age-related changes in drug pharmacokinetics and pharmacodynamics, multimorbidity and polypharmacy are widely regarded as key predisposing factors for adverse drug reactions (ADRs) [Mangoni and Jackson, 2004; Viktil et al. 2007; Cherubini et al. 2011; Petrovic et al. 2012; Onder et al. 2013].
It is widely recognized that there is no universally accepted definition of ‘polypharmacy’ [Cadogan et al. 2016]; it has been defined as the prescribing of medications over a threshold number of four or five [Maher et al. 2014; Patterson et al. 2014], or may be considered conceptually to describe the prescribing of ‘many drugs’ or ‘too many’ drugs [Cadogan et al. 2016], introducing a dimension in which the appropriateness of the prescribing is taken into account [Aronson, 2004]. Irrespective of the lack of a universally recognized definition of the term, numerous studies have highlighted the association between polypharmacy and inappropriate medication use in older people [Cadogan et al. 2016; Bradley et al. 2012; Cahir et al. 2010]. Medicines are considered to be prescribed appropriately when they have a clear evidence-based indication, are cost effective and well tolerated [O’Mahony and Gallagher, 2008]. Inappropriate medication use, inappropriate drug use (IDU), inappropriate prescribing (IP) and potentially inappropriate prescribing (PIP) are terms used to refer to suboptimal prescribing practices which include overprescribing, underprescribing and misprescribing of medications [Spinewine et al. 2007; Kaufmann et al. 2014]. The (in)appropriateness of prescribing for older people has received significant research attention in recent years, with numerous studies reporting high prevalence of PIP in acute and long-term care settings and in community-dwelling older people in Europe and North America, and demonstrating its association with increased risk of ADRs, morbidity, mortality and healthcare utilization [Fialova et al. 2005; Fu et al. 2007; Spinewine et al. 2007; Gallagher et al. 2008, 2011; Hamilton et al. 2011; García-Gollarte et al. 2012; Opondo et al. 2012; Hill-Taylor et al. 2013; Blanco-Reina et al. 2014; Galvin et al. 2014; Gosch et al. 2014; Kovačević et al. 2014; Shade et al. 2014; Tommelein et al. 2015]. However, few studies have focused specifically on people with dementia [Montastruc et al. 2013].
Dementia is an irreversible neurodegenerative disorder characterized by a cluster of signs and symptoms, including difficulties in memory, disturbances in language, psychosocial and psychiatric changes, and impairments in activities of daily living [Burns and Iliffe, 2009; Wu et al. 2016]. It is commonly associated with other chronic medical conditions such as diabetes, chronic obstructive pulmonary disease, chronic cardiac failure, musculoskeletal disorders, and vascular disease [Doraiswamy et al. 2002; Schubert et al. 2006; Lee et al. 2009; Onder et al. 2012; Bell et al. 2015], and as a consequence, polypharmacy [Onder et al. 2013]. It has been reported that people with dementia take an average of 5–10 medications, of which 1–2 are prescribed for dementia and the remainder are indicated for the treatment of other comorbid medical conditions [Elmståhl et al. 1998; Lau et al. 2010]. The use of multiple medications in this population raises a number of issues; memory loss, decline in intellectual function, and impaired judgement and language may cause difficulties in communicating symptoms or problems related to adverse effects of drugs [Ganjavi et al. 2007; Onder et al. 2011]. Furthermore, older people, and those with dementia in particular, are often excluded from clinical trials and guidelines, so the evidence base to guide prescribing for these patients is limited [Brauner et al. 2000; Marengoni and Onder, 2015]. Finally, people with dementia have a reduced life expectancy, which may impact on the risk–benefit profile of a medication; drugs for primary or secondary prevention may require years of treatment to demonstrate their benefit, and their use may be considered inappropriate if a patient is not expected to survive to realize this benefit [Currow and Abernethy, 2006; Fusco et al. 2009; Holmes, 2009; Onder et al. 2013].
In this narrative review article we discuss the prevalence of PIP in older people with dementia, giving consideration to how appropriateness is assessed, the medications which are most commonly implicated in PIP, the clinical consequences of such prescribing, and research priorities to optimize prescribing for this vulnerable patient group.
Search methodology
A literature search was conducted using MEDLINE (1950–January 2016), EMBASE (1980–January 2016), Web of Science (1981–January 2016), International Pharmaceutical Abstracts (1970–January 2016) and the Cochrane Library of Systematic Reviews (1999–January 2016). The search terms used were ‘inappropriate’, ‘potentially inappropriate’, ‘dementia’, ‘Alzheimer’, ‘drugs’, ‘medicines’, ‘medications’, ‘prescribing’, ‘prescription’, ‘older’, ‘old’, ‘elderly’, ‘aged’ and combinations thereof. Only articles in the English language were selected. No attempt was made to reject papers on the basis of methodology, for example not a randomized controlled trial, as some studies were descriptive in nature or were papers that were classified as commentaries.
Medication appropriateness in people with dementia
There has been considerable effort to develop criteria to classify the appropriateness of medication use in older people in recent years, resulting in the evolution and refinement of a number of tools. These utilize implicit (judgement-based) or explicit (criterion-based) measures of medication appropriateness, or a combination of both approaches [Kaufmann et al. 2014]. A recent systematic review found 46 available tools, each with limitations, strengths and weaknesses [Kaufmann et al. 2014]. These tools varied in their target populations; while most named older people as target patients, just over 20% did not specify an age group. The majority (59%) did not specify healthcare setting, some focused on hospitalized patients, while others considered ambulatory care or long-term care [Kaufman et al. 2014]. The Beers criteria [Beers et al. 1991; Beers, 1997; Fick et al. 2003; Campanelli, 2012; American Geriatrics Society, 2015] and the Screening Tool of Older Person’s Prescriptions (STOPP) and the Screening Tool to Alert doctors to Right Treatment (START) criteria [Gallagher et al. 2008; O’Mahony et al. 2014] are probably the best known and most widely studied of these tools in US and European settings respectively. These tools, and others developed since the publication of the systematic review by Kaufmann and colleagues [Renom-Guiteras et al. 2015], do not specifically consider older people with dementia [Kröger et al. 2015; Montastruc et al. 2013]; there is a paucity of studies relating to the development and application of criteria specifically for assessing appropriateness of medication for this patient population.
PIP in people with dementia has been understudied to date [Montastruc et al. 2013; Johnell 2015; Sköldunger et al. 2015], but is gaining research interest, as indicated by the recent publication of a number of studies focusing on this particularly vulnerable cohort. Much of this work, discussed below, has focused on people with advanced dementia (characterized by profound cognitive deficits, inability to recognize family members, speech limited to fewer than five words, total functional dependence, incontinence, and inability to ambulate [Mitchell et al. 2012]) and limited life expectancy. These studies are summarized in Table 1.
Summary of studies determining medication appropriateness in people with dementia.
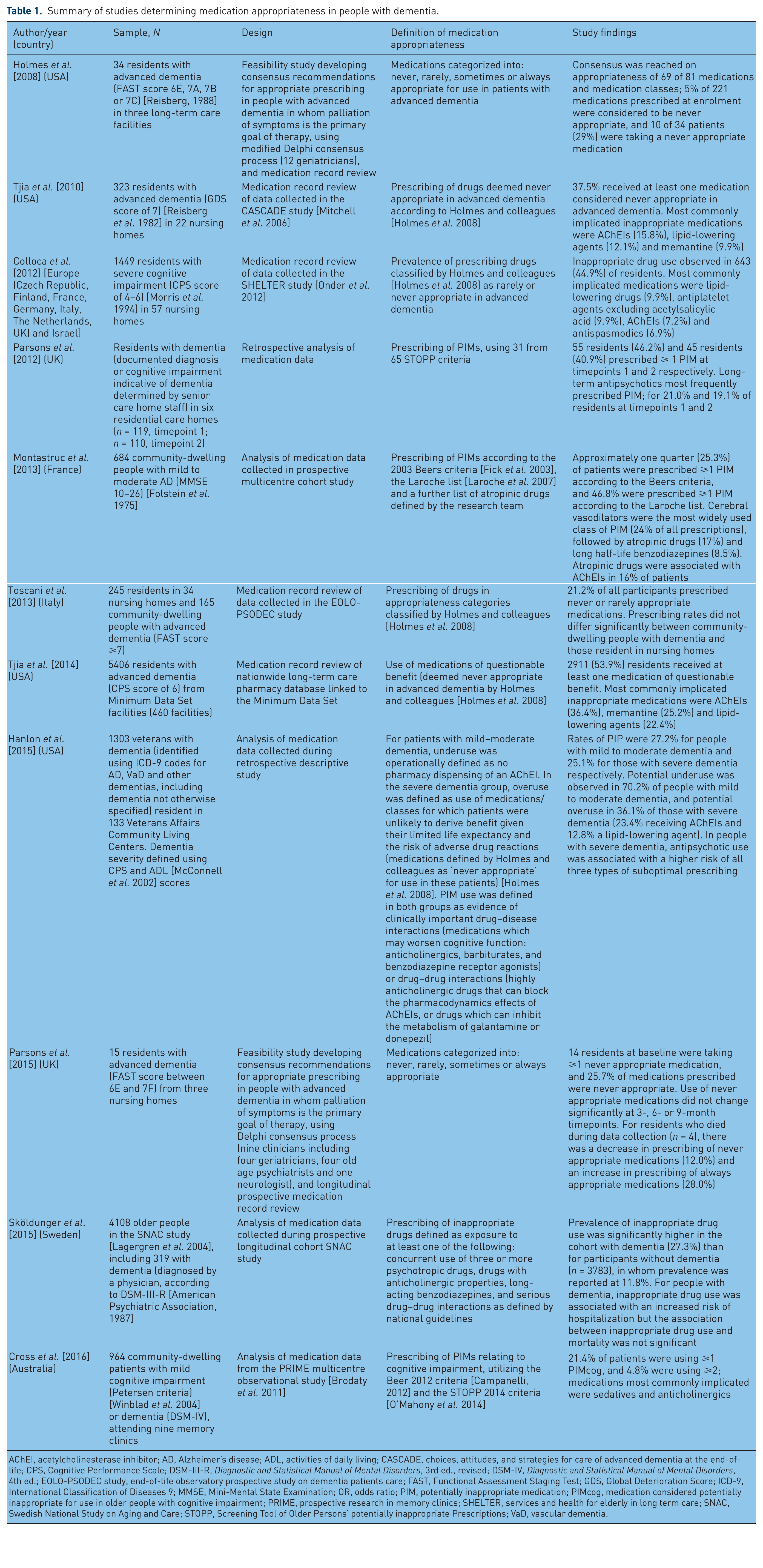
AChEI, acetylcholinesterase inhibitor; AD, Alzheimer’s disease; ADL, activities of daily living; CASCADE, choices, attitudes, and strategies for care of advanced dementia at the end-of-life; CPS, Cognitive Performance Scale; DSM-III-R, Diagnostic and Statistical Manual of Mental Disorders, 3rd ed., revised; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; EOLO-PSODEC study, end-of-life observatory prospective study on dementia patients care; FAST, Functional Assessment Staging Test; GDS, Global Deterioration Score; ICD-9, International Classification of Diseases 9; MMSE, Mini-Mental State Examination; OR, odds ratio; PIM, potentially inappropriate medication; PIMcog, medication considered potentially inappropriate for use in older people with cognitive impairment; PRIME, prospective research in memory clinics; SHELTER, services and health for elderly in long term care; SNAC, Swedish National Study on Aging and Care; STOPP, Screening Tool of Older Persons’ potentially inappropriate Prescriptions; VaD, vascular dementia.
The most significant advance in the literature in this area was the development of consensus criteria for appropriate prescribing by Holmes and colleagues [Holmes et al. 2008]. These criteria have since been applied in a number of other studies in the USA and Europe (Table 1). More recently, Kröger and colleagues undertook a scoping review of criteria on medication appropriateness in severe dementia and characteristics of intervention studies [Kröger et al. 2015]. This revealed that although considerable attention had been devoted to inappropriateness of medication use among older residents of nursing homes, comprehensive specific criteria were limited to the list of Holmes and colleagues. Following the publication of this review, Parsons and colleagues presented medication appropriateness indicators for people with advanced dementia specific to the UK context developed using a similar approach to Holmes and colleagues [Parsons et al. 2015], details of which are outlined in Table 1. To the best of the author’s knowledge, the criteria identified by Holmes and colleagues [Holmes et al. 2008] and Parsons and colleagues [Parsons et al. 2015] represent the only currently available systems for identifying PIP in people with advanced dementia in whom a palliative approach is needed.
Studies including people with mild to moderate dementia or recruiting across the full spectrum of disease severity are now beginning to appear in the research literature. Summarized in Table 1, these studies focus on the medication regimen as a whole, or on several medications or medication classes. They demonstrate the high prevalence of PIP across disease severity and setting and country of care, and the necessity for development and validation of tools to assess appropriateness of prescribing specifically for people with dementia. Expanding the evidence base in this area is of critical importance due to the adverse health, clinical and economic outcomes associated with IDU among older people with dementia [Sköldunger et al. 2015].
In addition to this body of work, some studies have considered misprescribing, overprescribing, or underprescribing of individual medications or medication classes, as outlined below. Considerable scope exists to improve the quality of prescribing for people with dementia in each of these areas.
Appropriateness of prescribing of specific drug classes
Anticholinergic medications
Older people are commonly subjected to a high anticholinergic load or burden due to the widespread use of anticholinergic/antimuscarinic medications and the wide range of medications possessing anticholinergic side effects (such as antihistamines, antidepressants, anti-Parkinson agents, antipsychotics, antispasmodics, and skeletal muscle relaxants) [Mate et al. 2015]. People with dementia are particularly susceptible to adverse effects associated with a high anticholinergic load [Sunderland et al. 1985, 1987; Sura et al. 2013]; they have reduced levels of acetylcholine (a neurotransmitter critical to the neurons involved in cognition), and as a consequence anticholinergic medications may worsen their cognitive function [Feinberg, 1993; Roe et al. 2002; Carnahan et al. 2004; Kemper et al. 2007; Rudolph et al. 2008; Carrière et al. 2009; Modi et al. 2009; Fox et al. 2011].
Studies have demonstrated a high anticholinergic load among people with dementia; work conducted in the US, Australia and the UK have reported that between 40% and 60% of patients with dementia use at least one anticholinergic medication [Chan et al. 2006; Bhattacharya et al. 2011; Sura et al. 2013; Mate et al. 2015; Cross et al. 2016], with 10–25% using higher potency anticholinergic drugs or medications with clinically significant anticholinergic activities [Bhattacharya et al. 2011; Sura et al. 2013; Mate et al. 2015; Palmer et al. 2015; Cross et al. 2016]. Due to the association of anticholinergic burden with falls, worsening cognition and worsening function [Moore and O’Keefe, 1999; Tune, 2001; Cao et al. 2008; Lowry et al. 2011; Uusvaara et al. 2011], clinicians should consider the anticholinergic properties of medications when adding to or changing patients’ drug regimens, with a view to minimizing the anticholinergic effects [Palmer et al. 2015].
Psychotropics
Psychotropic drugs, including antipsychotics, anxiolytics, hypnotics, antidepressants, anticonvulsants and antidementia drugs, are widely prescribed for behavioural and psychological symptoms of dementia (BPSD) [Thompson Coon et al. 2014; van der Spek et al. 2015], which include behaviours such as aggression, screaming, restlessness, anxiety, hallucinations and depressive mood [Cerejeira et al. 2012]. These neuropsychiatric symptoms are highly prevalent in people with dementia; up to 90% of people with Alzheimer’s disease experience at least one symptom during the course of the disease [Liperoti et al. 2008].
Treatment guidelines for BPSD recommend that antipsychotics should not be used as first-line management; detailed assessment to rule out other treatable causes of symptoms and alternative nonpharmacological interventions should be tried first [Food and Drug Administration, 2005, 2008; National Institute for Health and Care Excellence, 2006; European Medicines Agency, 2010; Chiu et al. 2015; Foebel et al. 2016]. Antipsychotics are unlicensed for treatment of these symptoms [Muench and Hamer, 2010], with the exception of risperidone, which has approval for this indication in some countries [Langballe et al. 2014]. Furthermore, they have demonstrated limited efficacy and have been associated with serious side effects, increased morbidity, exacerbation of functional and cognitive decline, and mortality [Schneider et al. 2005; Kales et al. 2007; Liperoti et al. 2009; Trifirò et al. 2009; Ballard et al. 2011; Musicco et al. 2011; Huybrechts et al. 2012; Langballe et al. 2014; Bonner et al. 2015; Foebel et al. 2016]. Despite this, they continue to be prescribed frequently, often on an unlicensed, long-term basis. As a result, the appropriateness of antipsychotic use in this population is often questioned [Chiu et al. 2015; Foebel et al. 2016], and it has been estimated that two-thirds of prescriptions are unnecessary [Ballard et al. 2014]. Although rates of antipsychotic prescribing in older people with dementia are declining in response to warnings from agencies such as the US Food and Drug Administration [Food and Drug Administration, 2005, 2008], the European Medicines Agency [European Medicines Agency, 2010] and the UK Department of Health [Banerjee, 2009], antipsychotic use remains widespread, particularly in long-term care settings. Recent rates of antipsychotic prescribing have been reported to range from 7.4% in primary care and 16.6% in acute care in the UK [Martinez et al. 2013; Stephens et al. 2014], to 25% across care settings in Germany [Schulze et al. 2013], 31% in institutional care settings in The Netherlands [Kleijer et al. 2014], and 40% in geriatric care settings in Sweden [Lövheim et al. 2006]. In the US, the 2004 National Nursing Home survey reported that approximately one third (32.9%) of nursing home residents with dementia received at least one antipsychotic medication [Kamble et al. 2009]. More recent figures suggest that patterns of prescribing in the US have not changed considerably; 23.9% of all long-stay nursing home residents received at least one antipsychotic medication [Centres for Medicare and Medicaid Services, 2011]. Future research should aim to continue to gather and apply research evidence to improve the safety and quality of antipsychotic prescribing, and to address a number of key unanswered questions regarding the mortality risk of drugs at the individual drug level, the relationship between dose and mortality, and the individual patient factors which may predispose or mitigate risk [Ballard et al. 2014].
Antibiotics
People with dementia are susceptible to infections, including respiratory tract infections, urinary tract infections (UTIs), and skin and soft tissue infections [Mitchell et al. 2009; Vandervoort et al. 2013]. Treatment decisions, particularly in the more advanced stages of dementia and at the end of life, are complex [van der Maaden et al. 2015] and require a balance of the potential burden caused by treatment, the best interests of the patient, and family and patient preferences [van der Steen et al. 2001; Hurley and Volicer, 2002]. This complexity is due in part to the inability of patients to communicate their symptoms, and because typical symptoms of infections are often absent [Scherder et al. 2009; D’Agata et al. 2013].
Much work has been undertaken to examine potentially inappropriate antimicrobial use in older people residing in long-term care settings [Zimmer et al. 1986; Warren et al. 1991; Pickering et al. 1994; Montgomery et al. 1995; Loeb et al. 2001; Lim et al. 2012; Phillips et al. 2012; Stuart et al. 2012; Peron et al. 2013; Sloane et al. 2014; van Buul et al. 2015], reporting asymptomatic bacteriuria as the most common reason for potentially inappropriate antibiotic use [Pickering et al. 1994; Loeb et al. 2001; Nicolle, 2002; Black et al. 2006; Phillips et al. 2012; D’Agata et al. 2013; van Buul et al. 2015]. However, there has been limited work undertaken to date to examine the appropriateness of antibiotic prescribing specifically in people with dementia [Mitchell et al. 2014]. One study of US nursing home residents with advanced dementia reported that 44% of treated episodes of suspected infection met minimum clinical criteria [Loeb et al. 2001] for initiation of antimicrobial treatment, suggesting that much of the extensive prescription of antimicrobials in advanced dementia may be unwarranted [Mitchell et al. 2014]. The authors reported that antibiotics were most likely to be initiated in the absence of minimum treatment criteria for UTIs which rely on subjective signs and symptoms undetectable to the observer in the absence of patient self-report. They highlighted the difficulty in interpreting what is ‘symptomatic’ in people with advanced dementia and in applying minimum criteria for treatment. The development of consensus criteria to measure appropriateness of prescribing, specific to people with dementia and comprising indicators of appropriate prescribing of antimicrobials, would facilitate a more judicious approach to infection management in this vulnerable patient population, avoiding unnecessary treatment burden and mitigating the threat of multidrug-resistant organisms [Mitchell et al. 2014].
Analgesics
It has been widely reported that approximately 50% of older people with dementia experience pain [Leong and Nuo, 2007; Zwakhelen et al. 2009; Barry et al. 2016], which is often chronic in nature and caused by musculoskeletal conditions, previous fractures or neuropathies [Hadjistavropoulus et al. 2007; Scherder and Plooij, 2012]. Despite this, there is evidence that pain in dementia often remains undetected and undertreated [Hoffmann et al. 2014; Tan et al. 2015]. A number of possible reasons for this have been suggested; people with dementia have difficulty in expressing and communicating their pain [Marzinksi, 1991; Ferrell et al. 1995; Cook et al. 1999; Husebo et al. 2008; Reynolds et al. 2008], it can be difficult for observers to identify pain which can manifest in a range of behaviours and symptoms also indicative of other forms of distress including depression, boredom or anxiety [Breland et al. 2015], and physicians may be reluctant to prescribe medications, particularly opioids, for these patients due to higher rates of treatment complications [Closs et al. 2004; Pickering et al. 2006; Corbett et al. 2012; Monroe et al. 2014; Breland et al. 2015; Li et al. 2015]. Furthermore, a lack of pharmacological studies examining the pharmacodynamic properties of analgesics in this vulnerable patient population [McLachlan et al. 2011] may result in treatment decisions made in the absence of a clear knowledge of the impact of comorbidities on the efficacy and adverse effect profiles of analgesics [Achterberg et al. 2013].
It has been hypothesized that people with dementia may perceive and express pain differently to cognitively intact individuals; however, to date, many studies examining pain and analgesic use in people with dementia have utilized pain assessment scales or instruments which are not specific to this patient population [Scherder et al. 2003; Corbett et al. 2012; Tan et al. 2015]. Future research is required using dementia-specific pain scales [Achterberg et al. 2013; Tan et al. 2015] and considering the neuropathology, experience, assessment and management of pain in these vulnerable patients [Tan et al. 2015]. The appropriateness of pharmacological treatments for people with dementia, considering the use of different analgesic classes and doses, as part of a standardized approach to pain management, is a research priority [Tan et al. 2015].
Priorities for research
Further studies of PIP in large cohorts of people with dementia and cognitive impairment, which include patients across the spectrum of variants and dementia severities, are required [Johnell, 2015; Sköldunger et al. 2015]. In order to undertake these studies, it is imperative that prescribing appropriateness criteria specific to this patient population are developed and/or utilized, which take into consideration the most commonly implicated medications discussed in this narrative review; namely anticholinergics, psychotropics, antibiotics and analgesics, in addition to drug–drug and drug–disease interactions. Such criteria must consider dementia of all severities and be applicable across settings of care. Future work should also examine the impact of PIP on health outcomes for people with dementia [Hanlon et al. 2015], an area which has received little research attention to date.
Conclusion
Older adults with dementia are at risk of suboptimal prescribing and PIP. Evidence-based guidelines to assist physicians in prescribing for these vulnerable patients, who often have multiple comorbidities and take multiple medications, are lacking. The pharmacotherapeutic management of these patients is an area requiring urgent research attention.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.