
Abstract
Polypharmacy and prescribing of potentially inappropriate medications (PIMs) are the key elements of inappropriate medication use (IMU) in older multimorbid people. IMU is associated with a range of negative healthcare consequences including adverse drug events and unplanned hospitalizations. Furthermore, prescribing guidelines are commonly derived from randomized controlled clinical trials which have specifically excluded older adults with multimorbidity. Consequently, indiscriminate application of single disease pharmacotherapy guidelines to older multimorbid patients can lead to increased risk of drug–drug interactions, drug–disease interactions and poor drug adherence. Both polypharmacy and PIMs are highly prevalent in older people and strategies to improve the quality and safety of prescribing, largely through avoidance of IMU, are needed. In the last 30 years, numerous explicit PIM criteria-based tools have been developed to assist physicians with medication management in clinically complex multimorbid older people. Very few of these PIM criteria sets have been tested as an intervention compared with standard pharmaceutical care in well-designed clinical trials. In this review, we describe the most widely used sets of explicit PIM criteria to address inappropriate polypharmacy with particular focus on STOPP/START criteria and FORTA criteria which have been associated with positive patient-related outcomes when used as interventions in recent randomized controlled trials.
Keywords
Introduction
The management of multimorbidity in older people is challenging. Treatment guidelines are generally derived from single disease trials which often exclude older participants, and their application to patients with multimorbidity may result in lengthy, problematic prescriptions.1–4 While the individual recommendations from a guideline may be rational, the sum of all recommendations for the individual multimorbid patient is often inappropriate. In the United States, 39% of adults aged over 65 years take five or more daily medications. 5 In Europe, almost 25% of nursing home residents take 10 or more daily medications. 6 Polypharmacy, defined here as the concurrent use of five or more daily medications, may of course be appropriate and justified when treating multimorbid patients. However, polypharmacy, when it is inappropriate, is associated with a range of adverse consequences including falls, hip fractures, cognitive decline and avoidable hospitalizations.7–9 Older people are particularly vulnerable to the harmful effects of polypharmacy due to age-related changes in pharmacokinetics and pharmacodynamics.10,11 Therefore, the challenge for the prescriber when treating older multimorbid patients is to strike a balance between optimizing chronic disease control and minimizing the risks of polypharmacy.
Inappropriate polypharmacy which engenders potentially inappropriate medications (PIMs) can be addressed by examining the process of prescribing. 12 This involves screening for inappropriate medication use (IMU). IMU refers to (1) drug overuse, the use of drugs without a valid indication and (2) drug misuse, the incorrect choice of drug (potential harm outweighs the benefit, risk of drug–drug interactions or drug–disease interactions), incorrect dose or incorrect duration.12–14 The aim is to match the medication regimen to the patient’s overall condition and goals of care. 15 Prescribers also have the opportunity to address inappropriate polypharmacy when they encounter the adverse outcomes of prescribing. Adverse drug events (ADEs) cause or contribute significantly to 6–17% of all hospital admissions in older adults.16,17 However, ADEs are under-recognized in this population because they commonly manifest as nonspecific symptoms such as fatigue, dizziness, falls, constipation and confusion.11,18 It has been suggested that any new symptom in an older patient should be considered a drug side effect until proven otherwise. 18
Despite the importance of choosing the correct drugs, screening for IMU and recognizing ADEs, it is a fact that the great majority of older people with multimorbidity are managed by physicians who do not have expertise in geriatric medicine or pharmaco-therapeutics. 19 Valid and effective methods are needed to assist these physicians with the management of patients with multimorbidity and polypharmacy.
In the last 30 years, multiple criteria-based strategies to address inappropriate polypharmacy have been published. Implicit PIM criteria are judgement-based quality indicators that focus primarily on the patient rather than drugs or diseases. Although patient-centered and often sensitive for detection of IMU, this approach is time-consuming and very much depends on the knowledge and experience of the prescriber. 12 For this reason, implicit criteria have limited applicability outside of the research setting. In contrast, explicit criteria are clearly defined statements which highlight PIMs in particular clinical circumstances. For the most part, explicit PIM criteria are based on trial evidence, expert opinion and consensus techniques. 12 The intention is not to replace clinical judgement but rather to alert the prescriber to potential instances of IMU. There are currently 26 published explicit criteria-based tools to address inappropriate polypharmacy which have been described in recent reviews.20,21 The present review will focus primarily on the most widely used explicit, criteria-based PIM tools (Table 1) and, in particular, those that have been used as interventions to address IMU in well-designed trials.
Most commonly used explicit criteria-based tools.
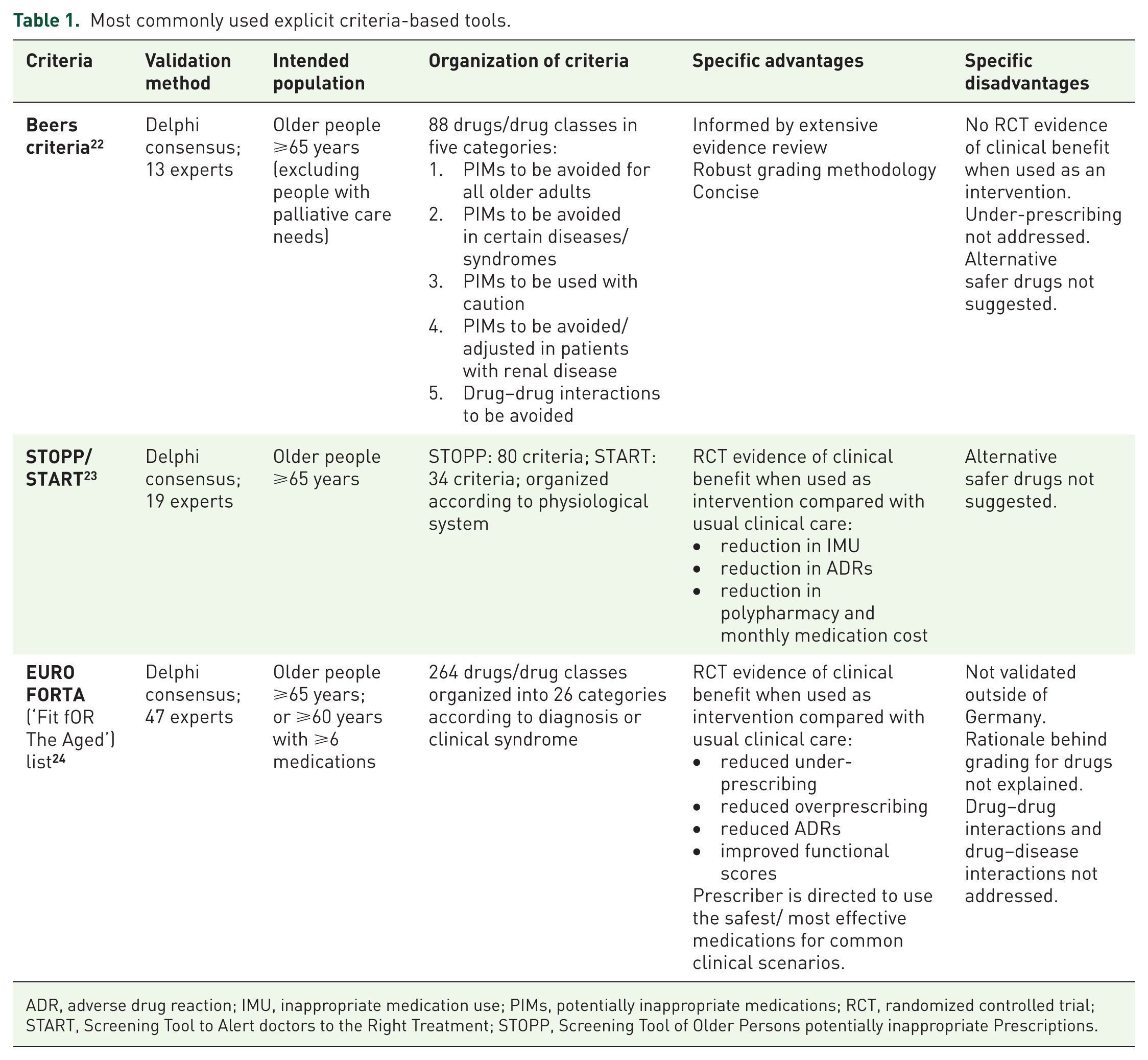
ADR, adverse drug reaction; IMU, inappropriate medication use; PIMs, potentially inappropriate medications; RCT, randomized controlled trial; START, Screening Tool to Alert doctors to the Right Treatment; STOPP, Screening Tool of Older Persons potentially inappropriate Prescriptions.
Beers criteria
Beers criteria are the most widely used criteria to evaluate potentially inappropriate prescribing in people over the age of 65 years. First published in 1991, the criteria have been updated four times, the most recent iteration being published in 2015. Since 2011, the American Geriatrics Society (AGS) have taken responsibility to update and maintain the Beers criteria. The intention of the Beers criteria is to improve care of older adults by reducing IMU, reducing ADEs, educating physicians and patients about appropriate pharmacotherapy, and by serving as a tool for evaluating quality of care, medication cost and patterns of drug use. 22 The criteria are not designed to be used in a hospice or palliative care setting.
The 2015 AGS Beers criteria were developed following a systematic literature review and consensus evaluation of evidence by a 13-member expert panel using a modified Delphi methodology. 22 The panel represented expertise in geriatric medicine, nursing, clinical pharmacy, research and quality measures. For each criterion, a quality of evidence and strength of recommendation rating was assigned. In addition, the rationale behind each recommendation was explained. The final criteria included 88 medications or medication classes, which are divided into five categories:
(i). drugs and drug classes to avoid in older adults independent of diagnosis or condition
(ii). drugs and drug classes to avoid in older adults with certain diseases or syndromes
(iii). drugs and drug classes that should be used with caution in older adults
(iv). non-anti-infective drugs that should be avoided or adjusted in older adults with renal disease
(v). non-anti-infective drug–drug interactions that should be avoided in older adults.
The use of Beers criteria drugs in older people has been shown to be associated with an elevated risk of unplanned hospitalization in the United States, Australia and Taiwan.9,25–27 However, these findings were not replicated in a European study and this may be explained by the fact that several drugs included in the Beers criteria are seldom prescribed or do not appear at all in drug formularies in Europe.28,29 As a result, several country-specific and region-specific derivations of Beers have recently been developed such as PRISCUS, 30 NORGEP 31 and the EU(7)-PIM criteria. 32 To date, there are no randomized controlled trials (RCTs) showing that application of the Beers criteria (or its derivatives) to older people’s prescriptions improves clinical outcomes.
STOPP/START criteria
The Screening Tool of Older Persons potentially inappropriate Prescriptions (STOPP) and the Screening Tool to Alert doctors to the Right Treatment (START) were developed in tandem in Ireland and published initially in 2008; the second iteration appeared in 2014.23,33 The 2014 version was developed following an extensive literature review and two rounds of Delphi consensus validation with 19 panellists across 13 European countries, each with recognized expertise in geriatric pharmacotherapy. STOPP version 2 consists of 80 IMU criteria outlining clinical circumstances where specific, commonly encountered medications or medication classes are considered potentially inappropriate in older people. Examples of these circumstances include:
(i). Drugs prescribed without an evidence-based indication for example, ‘levodopa or dopamine agonists for benign essential tremor.’
(ii). Drugs prescribed beyond their recommended duration for example, ‘proton pump inhibitors at full therapeutic dose to treat uncomplicated peptic ulcer disease beyond 8 weeks.’
(iii). Drug–drug interactions for example, ‘beta-blocker in combination with verapamil or diltiazem (risk of heart block).’
(iv). Drug–disease interactions for example, ‘prochlorperazine or metoclopramide with Parkinsonism (risk of exacerbating Parkinsonian symptoms).’
(v). Incorrect dosages for example, ‘long-term aspirin at doses greater than 160 mg per day (increased risk of bleeding, no evidence for increased efficacy).’
The criteria are organized according to physiological system and, in addition, there are sections relating to analgesic use, anticholinergic burden, and drugs that increase the risk of falls. START, comprised of 34 criteria, is designed to screen for potentially inappropriate under-prescribing and is intended to be used concomitantly with STOPP.
The use of STOPP/START to screen and address IMU in Europe, Asia, North America, South America, Africa and Australia suggests that the criteria have global relevance.34–41 In comparison with Beers criteria, patients with STOPP-defined IMU are more likely to have an ADE, present to the emergency department and be admitted to hospital. 39
To date, STOPP/START criteria have been tested as an intervention in four RCTs. These trials are summarized in Table 2. Gallagher and colleagues showed that, in older hospitalized patients, STOPP/START recommendations communicated to attending physicians at the time of hospital admission significantly improved medication appropriateness compared with usual pharmaceutical care. 42 In this RCT, medication appropriateness was measured using the medication appropriateness index (MAI) and the Assessment Of Underutilization (AOU), validated implicit IMU assessment tools.43,44 Using a similar design, O’Connor and colleagues showed that this intervention significantly reduced nontrivial adverse drug reactions (ADRs) compared with usual pharmaceutical care (absolute risk reduction of 11.4%; number of patients needed to screen to prevent one ADR = 9). 45 In Israel, Frankenthal and colleagues showed that application of STOPP/START recommendations significantly reduced polypharmacy (Table 3), IMU, incident falls and the average monthly cost of medications in frail elderly nursing home residents. 46 Finally, in Belgium, Dalleur and colleagues applied STOPP criteria to the prescriptions of hospitalized older patients in addition to a comprehensive geriatric assessment (CGA). 47 They showed that from this intervention, the reduction in PIMs for the intervention group was double that for the control group at hospital discharge (39.7 and 19.3%, respectively; p = 0.013).However, there was no statistically significant difference between the intervention and control groups in the proportion of patients prescribed ⩾1 potentially inappropriate medication at the time of discharge from hospital (16.1% versus 23.1%). The more modest results in this trial may be explained by the fact that just 39.7% of STOPP/START recommendations were implemented. This is in contrast to the aforementioned trials where uptake of recommendations ranged between 82% and 91%. This is important because the success of STOPP/START criteria, or indeed any other explicit tool, as an intervention will depend on its integration and implementation in normal clinical workflow.
Randomized controlled trials of STOPP/START as an intervention tool.

ADR, adverse drug reaction; AOU, assessment of under-utilization; CGA, comprehensive geriatric assessment; IMU, inappropriate medication use; LOS, length of stay in hospital; MAI, medication appropriateness index; PIMs, potentially inappropriate medications; QoL, quality of life; START, Screening Tool to Alert doctors to the Right Treatment; STOPP, Screening Tool of Older Persons potentially inappropriate Prescriptions.
Impact of STOPP/START on inappropriate medication use and polypharmacy.

PIMs, potentially inappropriate medications; START, Screening Tool to Alert doctors to the Right Treatment; STOPP, Screening Tool of Older Persons potentially inappropriate Prescriptions.
Two multicenter European trials are currently underway which are designed to examine the clinical impact of pharmacotherapy optimization software interventions based on STOPP/START version 2 criteria. SENATOR (‘Software Engine for the Assessment & Optimization of drug and nondrug Therapy in Older peRsons’) primarily examines the impact of the software intervention on ADR incidence in older people hospitalized with acute illness. A similar RCT called OPERAM (‘OPtimising thERapy to prevent Avoidable hospital admissions in the Multimorbid elderly’) is focused on the effect of a different software system on drug-related hospital admissions. The results of these trials are expected to be published in 2019 and 2020, respectively.
FORTA (‘Fit fOR The Aged’) list
FORTA was initially proposed in 2008 by the German clinical pharmacologist, Professor Martin Wehling, and was validated for use in Germany and Austria through a two-round Delphi procedure involving 20 experts in 2012.48,49 FORTA was updated in 2015 and, in subsequent years, six region-specific European FORTA lists were developed, validated and collated into the EURO FORTA list. 24 The EURO FORTA list consists of 264 medications/medication classes organized into 26 groups according to diagnosis or clinical syndrome. Each medication is graded according to the level of expected clinical benefit to older patients:
A (
B (
C (
D (
Guidance is given on the appropriateness of various drugs used to treat common conditions affecting older people such as hypertension, atrial fibrillation, chronic obstructive pulmonary disease, dementia, diabetes mellitus, idiopathic Parkinson’s disease and epilepsy. In addition, the drugs used to treat complex symptoms such as insomnia, behavioural and psychological symptoms of dementia and chronic pain are graded. The value of this format is that the prescriber is prompted to use the safest, most effective drugs first. Potentially harmful drugs are highlighted and, if required, the prescriber is directed towards more appropriate alternatives. However, important provisos are generally absent in the grading system. For example, opioids are assigned a grade B for the treatment of chronic pain. While undoubtedly effective, opioids are strongly associated with a range of potential adverse effects in older people including constipation and falls, and prescribers should be made aware of these well-known potential side effects. In addition, anticoagulants are assigned as grade A for use in the context of stroke prevention in older people. Routine anticoagulation for stroke is recommended only in certain specific clinical situations such as chronic atrial fibrillation and this grading, without extra qualifying information, has the potential to be misleading. Furthermore, drug–disease and drug–drug interactions are not addressed in FORTA.
The 2012 FORTA list was evaluated in a randomized controlled trial involving 409 hospitalized patients in Germany. 50 Patients were cluster randomized to the intervention or control group depending on which medical ward they were situated. Physicians overseeing the care of intervention ward patients were provided with FORTA-based recommendations for each individual patient. The primary endpoint was the FORTA score, a bespoke quantitative measure of IMU based on the FORTA list, where higher scores indicated greater levels of IMU. Secondary outcomes included incident ADRs and functional status scores, with all outcomes being measured at hospital discharge. In the intervention group, the median number of medications did not change between hospital admission and discharge. In contrast, the median number of daily medications in the control group increased by one. The primary endpoint (i.e. FORTA score) was significantly reduced (i.e. improved) in the intervention group relative to the control group. Intervention patients also had significantly reduced incidence of ADRs with a number needed to screen of only five to prevent one clinically significant ADR. Furthermore, significant improvements in functional scores were noted in the intervention group relative to the control group.
While these results are very encouraging, the trial had some significant limitations. The primary outcome measure was derived from the intervention tool and the use of a separate, validated measure of medication appropriateness would have strengthened the clinical impact of the results. Furthermore, the proportion of patients who had at least one ADR was 52.3%. This ADR incidence is substantially higher than the ADR incidence reported in a number of recent studies which vary from 11.5% to 32.2%.44,51–54 ADRs were ascertained using a trigger list of clinical events possibly representative of ADRs. These events included falls, confusion, nausea, dizziness, dyspnea, decompensated heart failure, acute kidney injury and angina. Dyspnea, not commonly defined as an ADR, accounted for almost 10% of all events. Of note, validated methods for assigning probability of causation to a drug were not used. This is an important limitation because if the recorded events were not corroborated as true ADRs, then the reduced event rate reported in the intervention arm may be related to factors other than implementation of FORTA recommendations (e.g. ward-based falls prevention strategy, greater staff numbers in the intervention ward).
Conclusion
The complexity associated with multimorbidity and polypharmacy mandates a systematic approach to ensure the best possible patient outcomes. While ongoing education and training for prescribers is essential, it is not reasonable to expect all physicians who care for older people to have expertise in geriatric pharmacotherapy. Explicit tools simplify the process of medication optimization by alerting the prescriber to potential IMU in specific circumstances.
Ultimately, the goal of any IMU intervention tool is to improve medication appropriateness and minimize the risk of serious ADRs. The Beers criteria, while groundbreaking in terms of being the first explicit criteria set to screen for IMU in older people, does not currently have a robust evidence base to support its use as an intervention tool. We contend that only explicit tools that have proven tangible clinical benefits merit serious attention. Currently, only STOPP/START criteria and the FORTA list meet this requirement on the basis of highly significant positive patient-related outcomes in recent RCTs.
Recognition and prevention of IMU in the future must be evidence-based. That evidence base in turn depends on PIM detection and minimization strategies that are proven to work from RCT data. Explicit PIM criteria have found their way into routine clinical practice, unlike implicit PIM/IMU criteria which remain in the research domain. Explicit PIM criteria that have an RCT-proven clinical benefit need to be applied in the arena of routine medication review for multimorbid older people, in particular those who are exposed to the highest levels of polypharmacy and its associated ADRs and ADEs. The challenge facing busy prescribers everywhere is finding efficient and practical methods of PIM/IMU explicit criteria deployment in busy, routine clinical practice. Avoidance of unacceptably prolonged patient consultations resulting from medication review and application of explicit PIM/IMU criteria remains a significant practical and research challenge, the solutions to which clearly lie within the information and communications technology software domain.
Technological innovation will undoubtedly advance in the coming decades and widespread deployment of explicit criteria-based tools in daily clinical practice is likely to be realized through sophisticated, reliable software systems integrated into normal clinical workflows. We believe that clinically relevant, explicit recommendations delivered to the prescriber in a timely manner, combined with emerging developments in pharmacogenomics, offers one way to stem the tide of the inappropriate polypharmacy and associated ADRs and ADEs and to ensure optimal management of the rapidly growing global population of multimorbid older patients.
Footnotes
Conflict of interest statement
Prof. O’Mahony and Dr. Gallagher have been involved in the development, refinement and validation of versions 1 and 2 of STOPP/START criteria.
Funding
The authors were supported by the SENATOR project funded by the EC Seventh Framework Programme (FP7), grant number 305930.