
Abstract
The positive benefit–risk ratio of most drugs is decreasing in correlation to very old age, the extent of comorbidity, dementia, frailty and limited life expectancy (VOCODFLEX). First, we review the extent of inappropriate medication use and polypharmacy (IMUP) globally and highlight its negative medical, nursing, social and economic consequences. Second, we expose the main clinical/practical and perceptual obstacles that combine to create the negative vicious circle that eventually makes us feel frustrated and hopeless in treating VOCODFLEX in general, and in our ‘war against IMUP’ in particular. Third, we summarize the main international approaches/methods suggested and tried in different countries in an attempt to improve the ominous clinical and economic outcomes of IMUP; these include a variety of clinical, pharmacological, computer-assisted and educational programs. Lastly, we suggest a new comprehensive perception for providing good medical practice to VOCODFLEX in the 21st century. This includes new principles for research, education and clinical practice guidelines completely different from the ‘single disease model’ research and clinical rules we were raised upon and somehow ‘fanatically’ adopted in the 20th century. This new perception, based on palliative, geriatric and ethical principle, may provide fresh tools for treating VOCODFLEX in general and reducing IMUP in particular.
Keywords
Introduction
In this article, we address the use of the terms polypharmacy and inappropriate medication use (IMU) together. Improved medical technology in the last generations has resulted in a huge increase in lifespan in general, and in patients with age-related chronic, life-shortening diseases in particular. This rapid change in the balance between young-healthy-supportive and old-very sick-debilitated subpopulations is associated with an unprecedented exponential increase in medical, economic and social age-related problems to which one of us (DG) has already referred to as the ‘Geriatric boom catastrophe’ [Garfinkel, 1997] and ‘The tsunami in 21st century health care’ [Garfinkel, 2013]. Nowadays, most adults and older people experience time-related increases in the number of incurable comorbidities, disability and suffering for increasingly prolonged periods before death. This situation makes models of the ‘one disease – one therapy/guideline’ an unrealistic approach to good care. However, older patients and those with comorbidity are usually excluded from randomized controlled trials (RCTs) that are considered essential for establishing evidence-based medicine (EBM) and clinical practice guidelines (CPGs). Combined with other major medical obstacles of our time, overdiagnosis, drug companies’ pressure and fear of lawsuits, most medical doctors are forced into practicing ‘defensive medicine’. Consequently, medical doctors use CPGs based on a single-disease-model EBM studies proven in young/middle-age adults without significant comorbidity who have a life expectancy of several decades. Family physicians and all experts usually extrapolate from these CPGs to include older people in whom research evidence underpinning guidelines does not exist. For most if not all drugs, this approach is inappropriate because old subpopulations are much more vulnerable to drug adverse effects (ADEs). The positive benefit–risk ratio of most drugs seems to be decreasing or becomes negative in correlation with age [Fick et al. 2003]; this reality is mostly pronounced and particularly troublesome in the very old, in correlation to increased extent of comorbidity, dementia, frailty and limited life expectancy for whom the acronym VOCODFLEX has been suggested [Garfinkel, 2013]. Furthermore, the extent and severity of IMU and polypharmacy (IMUP) also increases in correlation with exactly the same parameters, thus creating a vicious circle leading to significant health risks for an increasing number of older people. All specialists recommend adhering to guidelines regarding drug treatment in their field of specialty. Eventually, the higher the number of diseases (and specialists), the higher the complexity of guidelines recommended by health authorities. Boyd and colleagues have warned that ‘adhering to current clinical practice guidelines in elders with several co-morbidities may have undesirable effects … lead to inappropriate judgment of the care provided, create perverse incentives … and diminish the quality of their care’ [Boyd et al. 2005]. Obviously, the negative economic outcomes of IMUP are huge. Unfortunately, despite this ominous trap that places IMUP as a leading 21st century epidemic, a scheduled, formal drug reevaluation may never be performed in older people, either in hospitals or a long-term care (LTC) setting or in the community.
This article is primarily aimed at medical doctors of all expertise (mainly family physicians) but may also be useful to clinical pharmacists, nurses, other health professionals, experts in ethics and policy makers. The extent and quality of EBM declines in association with age is practically absent in VOCODFLEX; therefore, scientific, ‘high-quality’ reviews or meta-analyses in these subpopulations are practically impossible and should not be expected. However, this article has several specific goals. First, we review the extent of IMUP globally and highlight its negative medical, nursing, social and economic consequences. Second, we try to expose the main clinical, practical and perceptual obstacles that combine to create the negative vicious circle that eventually makes us feel unsuccessful, helpless, frustrated and even hopeless in treating VOCODFLEX in general, and in our ‘war against IMUP’ in particular. Third, we summarize a variety of international approaches and the main methods suggested and tried in different countries in an attempt to combat and improve the ominous clinical and economic outcomes of IMUP; these include a variety of clinical, pharmacological, computer-assisted, and educational programs. Lastly, we suggest a new comprehensive perception for providing good medical practice to VOCODFLEX in the 21st century. This includes new principles for research, education and CPGs completely different from the ‘single disease model’ research and clinical rules (or myths?) we were all raised on and somehow ‘fanatically’ adopted in the 20th century. Embracing our new perception, based on palliative, geriatric and ethical principles, enables fresh tools for treating VOCODFLEX in general and reducing IMUP in particular.
Age-related effect on pharmacodynamics, pharmacokinetics and adverse drug effects
Adverse dug effects (ADEs) are found in 35% of ambulatory older people [Hanlon et al. 1997] and in around two thirds of nursing home (NH) residents [Cooper, 1999]. Drug-related hospitalizations accounted for 2.4–6.5% of all medical admissions in the general population; the proportion is much higher for older patients [Lazarou et al. 1998; Onder et al. 2002; Pirmohamed et al. 2004].
Elderly people have a significantly higher risk of developing ADEs [Thomsen et al. 2007]. The reason for this is multifactorial, ranging from physiological changes and loss of reserve related to the aging process itself, age-related increase in frailty, disability and multiple comorbidities, the resulting intervention of multiple care providers and experts prescribing many drugs that eventually all together increase the risk of drug interactions and ADEs. Polypharmacy is associated with a 2.3-fold increase in the risk of ADEs [Ahmed et al. 2014]. In NHs, the risk of ADEs has been shown to double in residents taking nine or more medications compared with those taking fewer drugs [Nguyen et al. 2006]. Salazar and colleagues stress that polypharmacy, along with the numerous physiologic alterations that occur in the geriatric populations, distorts the picture of ‘normal’ drug effects, ‘common’ side effects and ‘known’ drug interactions. They conclude that as care givers we should ‘expect the unexpected, think the unthinkable’ [Salazar et al. 2007].
There is an age-related change in pharmacodynamics resulting from changes in drug-receptor affinity, thus altering the concentrations of drugs that are effective and toxic. Pharmacokinetic parameters including drug absorption and bioavailability, distribution and elimination (metabolism and particularly excretion) are also affected by age. There is an age-related decline in serum albumin concentrations [Turnheim, 2003]. Drugs that are highly bound to serum proteins such as phenytoin, warfarin and digoxin may compete for albumin binding sites, and therefore, their concurrent use even at small doses may be associated with increased risk and toxicity in older people. Drug excretion by the kidneys also declines with age [Turnheim, 2003]. Therefore, drugs that are mainly excreted by the kidney, for example digoxin, penicillin, aminoglycosides and lithium, may accumulate and have significantly prolonged duration of action even at lower doses. Unlike the kidney, there is no comparable, significant age-related decline in liver capacity to detoxify, metabolize and eliminate drugs. Nevertheless, simultaneous consumption of drugs that are highly metabolized by cytochrome P450 or similar liver enzymes may result in competitive inhibition (or enhancement) of each other, resulting in slow clearance, drug accumulation and toxicity.
Other drug, patient and environmental issues that may affect ADEs and IMUP
Drug–drug interactions
Medications interact with each other at a variety of sites along the way, from drug entry through distribution, metabolism and excretion (pharmacokinetics) to drug effect at the target organ’s receptor level (pharmacodynamics). Drug–drug interactions (DDIs) occur as a result of different mechanisms, including competitive inhibition due to chemical similarities of the compounds, leading to either decreased or increased concentrations at the target site; the clinical results are reduced efficacy and therapeutic effects or overdose and toxicity, respectively.
Competitive inhibition is only one well known mechanism explaining the negative impact of multiple medication interactions; many other as yet invisible and unknown molecular and biological mechanisms probably exist, contributing to the negative clinical impact of drug interactions. Probably only a few of these DDIs have been completely exposed and understood. For example, concomitant use of medications having anticholinergic properties with acetylcholinesterase inhibitors negatively affect cognitive and physical functioning in patients with Alzheimer’s disease [Bottiggi et al. 2007]. Iron supplements are associated with decreased absorption and lower efficacy of bisphosphonate, levothyroxine, methyldopa and quinolone antibiotics (Ferrous sulfate: Drug information, http://www.uptodate.com/contents/ferrous-sulfate-drug-information?source=see_link).
DDIs are a frequent cause of preventable ADEs and medication-related hospitalizations [Gurwitz et al. 2003]. A case control study from Canada evaluated hospitalizations resulting from drug-related toxicity in a population of older patients who had received one of three common drug therapies: glyburide (sulfonylurea group), digoxin or angiotensin converting enzyme (ACE) inhibitor. Hypoglycemia requiring hospitalization was six times higher in patients who had received cotrimoxazole. Risk of digoxin toxicity was 12 times higher in patients treated with clarithromycin, and hyperkalemia was 20 times more likely in patients treated with a potassium-sparing diuretic [Juurlink et al. 2003]. The prevalence of DDIs increases in correlation with the number of medications. It was estimated that patients taking five to nine medications had a 50% probability of DDIs but the risk increased to 100% when the number of drugs was 20 or more [Doan et al. 2013].
Consumption of an increased number of medications affects both pharmacodynamics and pharmacokinetics along several routes from drug uptake to clinical drug effect, with a variety of mechanisms, most of them probably unknown. Assessing interactions between two drugs is relatively easy. However, our chances of revealing all possible negative outcomes of DDIs are decreasing in correlation with the number of medications consumed. Several computer programs can detect DDIs for a few different drugs. However, we have not yet arrived at a situation where any scientific method or computer simulation can show all possible interactions among multiple medications, while factoring in the particular characteristics of a specific patient; this is particularly true in patients of the VOCODFLEX subpopulations [Garfinkel, 2014].
Hospitalizations are also associated with increased risk of severe DDIs. A study from Italy of 2712 patients aged 65 or older admitted to hospital showed that 1642 (60.5%) were exposed to at least one potential DDI and 512 (18.9%) were exposed to at least one ‘potentially severe’ DDI [Pasina et al. 2013].
Drug–disease and drug–food interactions
Drug effects may be altered by pre-existing diseases or health problems and vice versa; diseases may be aggravated by the new drugs prescribed. Common examples are the use of nonsteroidal anti-inflammatory dugs (NSAIDs) and salicylates that can exacerbate peptic ulcer disease and pseudoephedrine, which may result in increased blood pressure [Smalley and Griffin, 1996; Fick et al. 2003]. Obviously, the risk increases with the number of maladies (comorbidity); association exists between increased number and severity of illnesses and increased number of ADEs [Nobili et al. 2011]. Polypharmacy increases the risk of drug–food interactions when a food interferes with the drug’s absorption or effects. Poor nutritional status may interfere with drug efficacy or cause decreased excretion of some drugs, leading to higher risk of drug toxicity. Some examples are a high-fiber diet decreasing digoxin bioavailability leading to subtherapeutic serum concentrations and increased risk of treatment failure; food decreasing bisphosphonate absorption leading to treatment failure. Potassium-rich food consumption may increase the risk of hyperkalemia when potassium-sparing diuretics or ACE inhibitors are prescribed [Schmidt and Dalhoff, 2002; Akamine et al. 2007]. Herbals and dietary supplements are also of importance because of their increased consumption in this age group [Kaufman et al. 2002; Kelly et al. 2005]. In a study of 3005 community dwelling people aged 57–85 years, concurrent use of over-the-counter medications and dietary supplements were 46% and 52%, respectively. Overall, 4% of individuals were potentially at risk of having a major DDI, again being most prevalent (10%) among the oldest age group. Half of these drug reactions were due to use of nonprescription medications [Qato et al. 2008]. Other herbal remedies reported to have high risk of interactions are glucosamine, ginkgo biloba, chondroitin and garlic [Wold et al. 2005].
Prescription cascade
The term prescription cascade refers to situations when symptoms resulting from ADEs are perceived as new symptoms caused by a ‘new’ underlying disease process or aging itself [Gill et al. 2005]. Due to the age-related increase in the number of drugs consumed, this age-related phenomenon creates an ominous vicious circle of overdiagnosis, useless evaluations and overtreatment, thus further increasing the extent of IMUP. Examples of IMUP related to prescription cascades include the following: pain due to osteoarthrosis → NSAID prescribed → NSAID induces hypertension → more antihypertensive drugs; drug-induced nausea → metoclopramide → extrapyramidal symptoms → wrong diagnosis of Parkinson’s disease → levodopa → orthostatic hypotension (falls) and delirium → antipsychotics; dihydropyridine-induced leg edema → furosemide and potassium; automatically prescribing H2 blockers to patients on NSAID → delirium in older people → erroneous treatment with neuroleptics; ‘cold medications’ containing compounds with anticholinergic properties → urinary retention → α blocker → falls.
Nonadherence and poor compliance
Polypharmacy may be a potential source of therapeutic duplication [Salazar et al. 2007]. Typically, these errors occur when there is a change in care, shifting to another doctor, consultation from other specialties or upon discharge from the hospital [Omori et al. 1991; Riechelmann et al. 2007]. Thirty-two percent of recently discharged hospitalized patients incorrectly deleted or added a drug after discharge, 18% made errors in dosing, 12% of these errors had the potential for serious consequences [Omori et al. 1991]. Changes in complex medication regimens cause more confusion, especially if the older patient is already struggling with proper compliance with the old regimen [Yamada et al. 2001]. Phonetic confusion, flip-flopping errors and pill visual cue errors may also play a role [Salazar et al. 2007]. Polypharmacy may further decrease compliance and indeed the use of multiple medications is associated with nonadherence [Steinman and Hanlon, 2010]. Age itself is considered a poor predictor of nonadherence [Gellad et al. 2011] but almost one half of the older population experience adherence problems with at least one medication [Osterberg and Blaschke, 2005]. So, nonadherence, noncompliance and futile use of expired medications in older people may also increase the risk of ADEs and negative health outcomes (i.e. poor disease control, therapeutic failure, impaired functionality) and more frequent health service utilization [Malhotra et al. 2001; Haynes et al. 2008; Conn et al. 2009]. Several strategies addressed the importance of dose adjustment, trying to alert doctors to untreated conditions [e.g. the Screening Tool to Alert Doctors to Right Treatments (START) method]. However, a more thorough discussion of this problem is beyond the scope of this article, which focuses on IMUP.
Negative global health consequences of IMUP
Increased rate of hospitalizations, frailty, disability and mortality
Polypharmacy and IMU are an under-recognized cause of readmissions to hospital [Sehgal et al. 2013]. In community-dwelling ‘very old’ people, the prevalence of IMU was estimated as 18.6% and this subgroup had increased risk of at least one acute hospitalization [Klarin et al. 2005]. Analysis of 18 epidemiological studies, mostly from the USA, proved that the use of drugs on the Beers list (see section ‘Beers criteria’) was associated with higher risk of hospitalizations, both in outpatients living at home and in residents of NHs [Jano and Aparasu, 2007]. Another study following old people after hospitalizations found no association between ‘discharge medication regimen complexity’ and unplanned rehospitalization; there was a significant correlation between rehospitalization and the number of drugs upon discharge [Wimmer et al. 2014]. It was estimated that in the USA there are 99,628 emergency hospitalizations each year for ADEs in adults aged 65 years or older (nearly half among those aged 80 years or older). Nearly two thirds of hospitalizations were due to unintentional overdoses; four medication classes were implicated alone or in combination in 67% of hospitalizations: warfarin, insulins, oral antiplatelet agents and oral hypoglycemic agents. Hospitalizations due to medications designated as ‘high risk’ in older people by the 2011 Healthcare Effectiveness Data and Information Set were implicated in only 1.2% [Budnitz et al. 2011].
IMUP may also negatively affect function while increasing outpatient visits, hospitalizations, frailty and disability [Akazawa et al. 2010; Gnjidic et al. 2012a].
Gnjidic and colleagues showed that drugs with anticholinergic and sedative properties are associated with a more significant negative impact on physical functioning [Gnjidic et al. 2012b]. An association was found between polypharmacy (defined as the use of at least 10 drugs) and decreased 4 m walking speed and grip strength [Sganga et al. 2014]. Another meta-analysis has proven decreased physical activity in patients with dementia taking only four medications or more [Stubbs et al. 2014]. It may be concluded that IMUP increases the likelihood of impaired mobility, morbidity, hospitalization, NH placement and mortality [Frazier, 2005; Gomez et al. 2014].
Increased risk of cognitive impairment and dementia
Drug overdose and toxicity is obviously a leading cause of acute confusion (delirium), particularly in older people [Von Moltke et al. 2001]. The risk of drug-related cognitive impairment increases with the number of medications prescribed. In a prospective cohort study involving 294 older people, only 22% of patients taking five medications or less had impaired cognition compared with 54% in patients taking at least 10 drugs [Jyrkka et al. 2011]. Neurotransmission and signal transduction undergo age-related changes regarding regulation, sensitivity and efficacy [Pedigo, 1994; Fowler et al. 1997; Hatanpaa et al. 1999]. These changes eventually make older individuals much more vulnerable to drug effects. In an old person facing an already compromised cholinergic system, the addition of even small doses of anticholinergic drugs can significantly block postsynaptic acetylcholine receptors in the central nervous system (CNS). The results are confusion, disorientation and memory loss that might not have occurred in a younger person with a better baseline acetylcholine neurotransmission [Von Moltke et al. 2001]. Age-related decrease in renal clearance leading to accumulation and higher plasma drug concentrations, particularly in drugs that easily cross the blood–brain barrier, may result in much higher CNS drug concentrations with increased risk of brain toxicity. Cognitive impairment is commonly associated with ADEs and IMUP [Larson et al. 1987; Moore O’Keeffe, 1999; Alagiakrishnan and Wiens, 2004; Lau et al. 2010; Jyrkka et al. 2011]. Anticholinergic medication use is of specific concern older people. A recent Canadian trial has proven an association between anticholinergic drug burden (as assessed by four different tools) and increased risk of cognitive decline [Kashyap et al. 2014]. However, in two NH studies no improvement in cognitive function was proven following reduction of anticholinergic drug burden [Tollefson et al. 1991; Kersten et al. 2012]. A study of 1044 community-dwelling patients aged 75 years or older in Australia has evaluated the prevalence of anticholinergic medication load. Several patient factors were identified as possible predictors of high anticholinergic burden, including increased age, dementia, depression and polypharmacy [Mate Ke, 2015]. Anticholinergic burden is not only associated with cognitive impairment, but may also serve as a predictor of all-cause mortality in older patients [Mangoni et al. 2013; Ruxton et al. 2015]. In a systematic review, Salahudeen and colleagues concluded that studies with larger sample sizes, duration and methods for measuring anticholinergic drugs are still needed [Salahudeen et al. 2014].
Increased risk of falls and hip fractures
Falls represent a major risk factor for quality of life (QoL), morbidity and mortality, particularly if the result is fracture of the femur, other bones, subdural hematoma and head trauma. Soft tissue trauma is also of impact, increasing anxiety and fears from possible future falls. Gallagher and colleagues found that the use of potentially inappropriate medication (PIM, IMU) was associated with higher risk of falls [Gallagher et al. 2008]. In another study, the risk of falls in patients consuming at least six medications was 3.08-fold higher compared with those taking fewer medications [Chiu et al. 2014]. Drugs that are commonly associated with increased risk of falls include benzodiazepines, serotonin reuptake inhibitors and tricyclic antidepressants, neuroleptics, anticonvulsants, class IA antiarrhythmic agents, digoxin and diuretics [Thapa et al. 1998; Leipzig et al. 1999a, 1999b]. In another study, the incidence of hip fracture was associated with the use of a much larger list of drugs, including insulin, NSAIDs, loop diuretics, β blockers, anti-Parkinson drugs, anticonvulsive drugs, and drugs used for gastric protection and for chronic obstructive pulmonary disease [Rossini et al. 2014]. Polypharmacy itself is an independent risk factor for hip fractures [Lai et al. 2010; Pan et al. 2014]. Considering the serious consequences of falls on QoL, much caution is required while prescribing new medications to all older people, particularly the VOCODFLEX population who are at the highest risk of falling.
Negative impact on nutrition
Unintentional weight loss in older people is associated with adverse health outcomes, including frailty, functional decline, loss of independence [Jensen et al. 1997; Markson, 1997] and increased overall mortality [Newman et al. 2001]. IMUP can interfere with taste, result in nausea, gastrointestinal discomfort, changes in normal gastrointestinal environment and, especially with anticholinergic agents, also salivary hypofunction; all of these may result in decreased oral intake [Zadak et al. 2013; Gaddey and Holder, 2014; Singh and Papas, 2014]. Polypharmacy may also affect metabolism and elimination of some nutrients, increase energy requirements and catabolism, and induce hypovitaminoses [Heuberger and Caudell, 2011; Zadak et al. 2013]. ADEs affecting the CNS with or without depression and dementia may result in anorexia. Drug-induced hand tremor and coordination disorders may negatively affect old people’s independence and ability to eat without assistance [Zadak et al. 2013]. In older people, all these effects may aggravate an already existing status of subclinical nutritional deficiencies and low energy intake. Nutritional status may be adversely affected by drugs. For example, anorexia resulting from acetylcholinesterase inhibitors, antibiotics, digoxin and hypnotics; early satiety due to anticholinergics or sympathomimetic drugs; reduced feeding ability from sedatives and opiates; NSAID- and bisphosphonate-induced dysphagia, constipation (opiates, diuretics) and diarrhea (laxatives, antibiotics) [Visvanathan et al. 2004; Sampson, 2009].
Increased risk of other morbidities
Polypharmacy may result or aggravate urinary incontinence and other urinary tract symptoms [Gormley et al. 1993; Talasz and Lechleitner, 2012]. In a population-based longitudinal study of women aged 70 and older, polypharmacy was associated with increased risk of lower urinary tract symptoms [Nuotio et al. 2005]. A recent study showed association between IMUP and increased risk of both major and clinically relevant nonmajor bleeding in older patients with venous thromboembolism receiving vitamin K antagonists [Leiss et al. 2015]. A study from Hong Kong showed that depressive symptoms were associated with the use of more than four medications [Liu et al. 2011].
Palliative aspects
The problem of IMUP is particularly troublesome in patients with limited life expectancy. Most drugs may be regarded as bearing little or no relation to the actual needs of patients in end of life (EoL) situations. This is true for most if not all ‘preventive’ medications, for example aspirin, statins, antihypertensives and even oral hypoglycemics. Moreover, even ‘palliative’ medications for symptom relief prescribed in EoL care are often used without EBM proving a positive benefit–risk ratio in this particularly frail subpopulation. Appropriate dosing or optimal administration routes are in many cases unknown. Avoiding or discontinuing drugs may be a choice, but this approach does not represent standard practice, and therefore, prescriptions are usually not adapted to changes in the course of advanced diseases. Several researchers have suggested that in the last period of life, management of medications should be based on palliative principles: avoiding life-extending drugs; drugs for primary or secondary prevention usually have no place unless time to benefit is clearly shorter than life expectancy and ADEs are not significant; start or withdraw drugs stepwise; revise the therapeutic objectives of each comorbid disease and adapt treatments accordingly [Holmes et al. 2006; Steinman and Hanlon, 2010; Cruz-Jentoft et al. 2012].
Negative global social-economic outcomes
As already stated, aging is associated with increased number and extent of age-related diseases, comorbidity and geriatric syndromes (VOCODFLEX). The higher the number of diseases and specialists, the higher the complexity of CPGs recommended by health authorities. Combined with overdiagnosis, drug companies’ pressure and ‘defensive medicine’, this creates a negative vicious circle of IMUP with significant health risks but also huge negative economic outcomes.
IMUP is associated with higher costs resulting from the accumulating sum of costs of inappropriate medications prescribed by more physicians and experts, but also the cost of unnecessary hospitalizations resulting from IMUP. In some studies, however, the methods used to eliminate confounding factors such as comorbidities from analyses trying to avoid IMU have been highly criticized [Jano and Aparasu, 2007; Spinewine et al. 2007]. The annual cost of drug-related problems in the USA is estimated at over $150 billion hospitalizations account for most of these costs [Ernst and Grizzle, 2001]. In 2007 in Ireland, total IMUP expenditure was €45,631,319, 9% of the overall expenditure on pharmaceuticals in those aged over 70 years. In the Netherlands, the annual cost of hospitalizations related to ADEs was €355 million in 2009 [Hoonhout et al. 2009]. In Germany, the annual cost of ADEs in ambulatory practice was €816 million and the annual nationwide total treatment cost of ADEs in hospitalized patients was €1.058 billion [Stark et al. 2011; Rottenkolber et al. 2012]. In Turkey, 33.5% of health expenditure was for drugs, with a large increase in the absolute costs in the first decade of the 21st century (2005/2006) (Health Data from Turkish Health Ministry, http://www.sb.gov.tr/TR/hata/1-0/edomy1fl1cwueh4500xyppma.ex). In a study of older adults in Spain, the annual cost of polypharmacy was $2201.17 for 131 older patients [Santibanez-Beltran et al. 2013]. In Sweden, between 2005 and 2009, the total prescribed drug expenditure increased by 4.8%; in the subgroups of patients with polypharmacy and excessive polypharmacy (>10 drugs), drug expenditure increased by 6.2% and 7.3% respectively [Hovstadius and Petersson, 2013]. It may be concluded that IMUP represents a rapidly increasing burden to health economies; promoting the skill and art of appropriate prescribing in older people, including VOCODFLEX, should be regarded as a major contributor to improving not only health but also global economic outcomes.
Educational programs designed to reduce drug load in older people
Strategies to reduce high-risk prescribing, including educational interventions, pharmacist-conducted medication reviews and policymakers’ interventions have been suggested and tried in older adults [Gnjidic et al. 2013]. Interactive, case-based interdisciplinary meetings involving multiple prescribers combined with deprescribing advice from clinical pharmacologists or appropriately trained pharmacists have been shown to be beneficial with regard to doctors’ deprescribing practice [Bregnhoj et al. 2009]
In their review, Spinewine and colleagues classified educational approaches into passive (e.g. didactic courses, dissemination of printed material) and more interactive (e.g. academic detailing) approaches. They stress that though educational approaches directly address the absence of training in geriatric pharmacotherapy, they are usually restricted to specific drugs or diseases [Spinewine et al. 2007]. Passive approaches seem to be ineffective. Academic detailing includes repeated face-to-face delivery of educational messages to individual prescribers by doctors or pharmacists. They can promote changes in prescribing behaviors but these are usually not sustained without continuous intervention; therefore, audit and feedback are important to enhance the effect. A low participation rate and barriers to implementation of interactive and multidisciplinary meetings all represent disadvantages [Spinewine et al. 2007].
Martin and colleagues used a home-based educational program consisting of a document mailed to older people using benzodiazepines. The education document included information and questions about the patient’s knowledge of the risks of taking benzodiazepine. Knowledge and beliefs about inappropriate prescriptions were ascertained prior to and 1 week after the intervention. The authors found significant effects of the program on medication knowledge, beliefs and risk perception [Martin et al. 2013].
Pimlott and colleagues conducted a prospective before–after educational intervention study on the prescription of benzodiazepines in 372 family physicians in an ambulatory care setting [Pimlott et al. 2003]. After 6 months there was an absolute decrease of 0.7% in prescribing long-acting benzodiazepines in the educational intervention group and an increase of 1.1% in the control group (p = 0.036). However, the authors note that this difference was not clinically significant and there was no difference in ‘long-term use of benzodiazepines’ and in combination treatment with other psychoactive drugs [Pimlott et al. 2003]. Eide and Schjott evaluated the effects of staff education on the administration of hypnotics in NHs in Norway [Eide and Schjott, 2001]. In this before–after study they observed a reduction in the prescribing and administration of long-acting benzodiazepines, but there was an increase in the use of short-acting hypnotics [Eide and Schjott, 2001]. One study by Fossey and colleagues in the UK and two different studies by Meador and colleagues and Ray and colleagues in the USA evaluated the effect of enhanced psychosocial care training focusing on behavior management on the use of neuroleptic drugs [Ray et al. 1993; Meador et al. 1997; Fossey et al. 2006]. They reported on a decreased number of residents taking neuroleptics, reduced antipsychotic doses and reduced days on antipsychotic respectively. In another study by Avorn and colleagues, a comprehensive educational outreach program led by a pharmacist focused on reducing the overall use of psychotics by improving the selectivity of their use [Avorn et al. 1992]. This intervention resulted in decreased mean psychoactive drug use scores (a scoring tool developed by the authors).
In a prospective before–after study in an ambulatory care setting in Canada, Rahme and colleagues used small-group workshops including a ‘decision tree’ to manage osteoarthritis as an educational approach in 249 family doctors. After 10 months they observed better adherence to guidelines by the physicians [odds ratio 1.8, 95% confidence interval (CI) 1.3–2.4] and some weak indication that the combination of workshops plus a decision tree was more effective than using the decision tree alone [Rahme et al. 2005]. Nishtala and colleagues reviewed studies in NHs and LTC facilities evaluating the impact of medication reviews and educational interventions on prescribing psychotropic drugs. They concluded that both approaches were effective in reducing psychotropic drug prescribing. Furthermore, a pharmacist’s medication reviews conducted as part of a multidisciplinary team-based approach resulted in improved identification and treatment of drug-related problems [Nishtala et al. 2008].
In a systematic review, Loganathan and colleagues identified 16 eligible studies addressing prescribing strategies in care homes [Loganathan et al. 2011] and classified them into four main interventions: staff education (prescribers or care home staff), multidisciplinary team meetings, pharmacist medication reviews and computerized clinical decision support systems. Eight out of 16 studies reported on educational strategies, and although the results were mixed, those including academic detailing seemed most promising. Stein and colleagues found that a 30 min structured training session on NSAID prescribing was associated with a decreased use of NSAIDs [Stein et al. 2001]. However, in two other studies by Crotty and colleagues and Rovner and colleagues, educational programs were not associated with a significant positive effect on prescribing [Rovner et al. 1996; Crotty et al. 2004].
Scott and colleagues concluded in their review that barriers to deprescribing include underappreciation of the scale of polypharmacy-related harm by both patients and prescribers; multiple incentives to overprescribe; a narrow focus on lists of IMU; reluctance of prescribers and patients to discontinue medication due to fear of an unfavorable sequel; and uncertainty regarding the effectiveness of strategies to reduce polypharmacy [Scott et al. 2014]. Ways to overcome these barriers comprise reframing the issue to one of the highest quality patient-centered care; openly discussing benefit–harm tradeoffs with patients and assessing their willingness to consider deprescribing; targeting patients according to highest risk of ADEs; targeting drugs more likely to be nonbeneficial; accessing field-tested discontinuation regimens for specific drugs; fostering shared education and training in deprescribing among all members of the healthcare team; and undertaking deprescribing over an extended time frame under the supervision of a single generalist clinician.
In a retrospective database study in Japan, Sato and Akazawa assessed polypharmacy and ADEs in older people taking antihypertensives [Sato and Akazawa, 2013]. They found an association between polypharmacy and risk of ADEs. To ensure that older patients understand the reasons for and the correct ways of taking medications, and thereby decrease the risk of therapeutic failure as well as ADEs, the authors suggest that the role of pharmacists should be expanded to the education of patients and the monitoring of appropriate medication use, particularly in cases of polypharmacy [Sato and Akazawa, 2013].
Pitkälä and colleagues studied the effect of nurse training on the reduction of PIM/IMU, including those of the Beers’ list, anticholinergic medications, NSAIDs, proton pump inhibitors and the use of multiple psychotropic medications in 227 residents of assisted-living facilities in Helsinki [Pitkälä et al. 2014]. In a RCT, 20 wards were randomized to those in which the staff received two 4 h training sessions on appropriate medication treatment (intervention group) and those in which the staff received no additional training (the control group). During the 12-month follow up, the mean number of potentially harmful medications decreased in the intervention wards (−0.43, 95% CI −0.71 to −0.15) but remained constant in the control wards (+0.11, 95% CI −0.09 to +0.31) (p = 0.004, adjusted for age, sex, and comorbidities). The authors concluded that activating learning methods directed at nurses in charge of comprehensive care can reduce the use of harmful medications. Furthermore, they also demonstrated that educational intervention for reducing harmful medications was associated with positive impacts on residents’ QoL and use of health services in institutionalized older people [Pitkälä et al. 2014]. These results are in line with several previous trials proving the efficacy of educational interventions targeted at nurses and physicians in reducing the use of psychotropic medications [Avorn et al. 1992; Meador et al. 1997; Schmidt et al. 1998; Roberts et al. 2001; Fossey et al. 2006].
Optimizing prescribing in older people in 2016: the main approaches
Throughout the last decades there have been several studies reporting on attempts to reduce prescribing errors. Many of them had significant methodological problems, they used different methods for measuring IMUP, and above all, most of them lacked clinical outcome measures with little attention given to measurement of tangible health outcomes such as medication-related ADEs, overall functioning or general health. These factors prevent comprehensive meta-analyses that might help clinicians determine the clinical value of individual interventions.
Structured medication management represents the main approach suggested to decrease the negative effects of IMUP. A number of ways for reducing IMUP have been suggested and they may be categorized as explicit (criteria based) and implicit (judgment based). Explicit tools [e.g. computers, Beers criteria, START/Screening Tool of Older Person’s Prescriptions (STOPP) criteria] usually include lists of ‘drugs to avoid’ or indicators to avoid IMU/PIM for several drugs or diseases. Implicit tools take into consideration both EBM data from research and clinical circumstances, but also incorporate preferences of the individual patient to judge drug appropriateness.
Computer-assisted digital tools versus patient-centered methods
A variety of computer programs have been developed in many countries in an attempt to detect DDIs and to reduce drug load. Two reviews have concentrated on the effectiveness of computerized decision-making support system interventions designed to improve IMUP in older people. The first review in 2008 [Yourman et al. 2008] showed that 8 of 10 studies have shown at least modest improvements in primary outcomes, such as appropriateness of prescribing, rate of ADEs and prescribing choices. The second review in 2012 [Topinkova et al. 2012] evaluating five studies concluded that computerized decision-making support systems are modestly but significantly effective in reducing IMU and ADEs across healthcare settings. Ghibelli and colleagues studied the applicability of a computerized prescription support system in hospitalized older patients. The use of a computerized prescription support system was associated with significant reduction in IMU and new-onset potentially severe DDIs. As the mean anticholinergic burden score upon admission was relatively low, the utility of the system in reducing the anticholinergic burden could not be evaluated [Ghibelli et al. 2013]. Seidling and colleagues showed that implementation of a highly specific algorithm-based clinical decision support systems substantially improved prescribing quality; the final prescription rate of excessive doses was reduced to 3.6%, with 20% less excessive doses compared with baseline (p < 0.001) [Seidling et al. 2010].
There is sufficient evidence indicating that implementation of computerized decision-making support systems can significantly though modestly reduce prescribing errors across multiple healthcare settings. However, we have very limited information regarding the beneficial effects of these approaches on patient health outcomes, such as mortality, morbidity, functional and cognitive status, and overall healthcare services’ utilization and costs.
Some countries already have electronic medical records with full medication information. It may be useful to apply universal electronic medical record systems for improving inappropriate prescribing in older people. These systems, which contain patients’ complete prescription lists, medical and drug history, may provide alarms that alert clinicians to a variety of potential drug interactions as they turn on their computers and try to prescribe a new drug [Lynch, 2011]. However, several authors warn that relying too much on computers may be misleading and even harmful to older patients. Most computer programs can detect DDIs for two or maybe three different drugs. However, our chances of revealing all possible negative outcomes of DDIs are decreasing with increasing numbers of medications consumed, and with the heterogeneity of age-related diseases, complications and other patient-specific characteristics. Even if the computer does not detect a simple interaction in a pair of drugs, prescribing more than 10 let alone 15 medications to older people is still likely to do more harm than good [Garfinkel and Mangin, 2010]. Garfinkel and Mangin suggested a much broader patient-centered approach that can accommodate to changing evidence, taking into consideration not only EBM but also clinical judgment and ethical issues, particularly patient and family preferences [Garfinkel and Mangin, 2010; Garfinkel, 2014].
Beers criteria
The Beers lists were originally created in an attempt to quantify the extent and type of IMU in NH residents [Beers et al. 1991]. The Beers list has been repeatedly updated [Beers, 1997; Fick et al. 2003, 2012], and the 2012 criteria identified 53 medications or medication classes to be avoided in older adults; they are classified into three groups of IMU in NH: drugs to be always avoided in older people, IMU and classes to avoid in older adults with certain diseases and syndromes, and list of medications ‘to be used with caution’ in older adults. The lists stand as the most widely cited criteria for evaluating IMUP. However, a study assessing the association between IMU and emergency department visits of people 65 years and older showed that the drugs included in the Beers criteria were responsible for only 3.6% of emergency room visits [Budnitz et al. 2007]. There is no RCT proving reduced rates of ADEs, hospitalization, costs, morbidity and mortality by using Beers criteria; predicting hospital admissions due to ADEs using Beers criteria is questionable [Hamilton et al. 2011]. The challenges and controversies will probably be addressed in the coming 2015 update.
Improved Prescribing in the Elderly Tool
Improved Prescribing in the Elderly Tool (IPET) was first published in 2000 [Naugler et al. 2000] and represented an attempt to update McLeod’s previously published inappropriate prescribing criteria [McLeod et al. 1997] to 362 inpatients, resulting in 45 different medications in 14 classes of drugs considered inappropriate while presenting a workable shortlist of the ‘more common’ inappropriate prescription instances in routine clinical practice. Although the IPET is similar to the Beers criteria, the latter identifies more medications that are potentially inappropriate [Barry et al. 2006]. IPET is not based on physiological systems; its criteria are not comprehensive enough, having only 14 cited situations to be avoided. IPET is heavily directed towards cardiovascular, psychotropic and NSAID use, while many other drug categories are under represented; it has been criticized mainly for the avoidance of β blockers in heart failure and of benzodiazepines with long half lives under any circumstances. There is insufficient convincing evidence regarding the benefit of IPET in reducing the incidence of ADEs, health resource utilization or mortality [O’Mahony and Gallagher, 2008].
STOPP and START
Most PIM lists and tools focus on deprescribing. However, inappropriate prescribing encompasses PIM/IMU and also the potential prescribing omissions. Older people are often denied potentially beneficial, clinically indicated medications without a valid reason. STOPP/START criteria for potential inappropriate prescribing in older people recognize the dual nature of inappropriate prescribing by including a list of both PIM (STOPP criteria) and the potential prescribing omissions (START criteria). Both START and STOPP tools were developed by interdisciplinary teams of geriatricians, geriatric psychiatrists, primary care physicians, pharmacologists and pharmacists in 2008 [Barry et al. 2007; Gallagher and O’Mahony, 2008]. Comparative studies of STOPP and the Beers criteria to detect inappropriate prescribing and ADEs showed higher sensitivity of the STOPP criteria [Gallagher and O’Mahony, 2008; Hamilton et al. 2011]. STOPP/START criteria as an intervention, applied at a single time point during hospitalization for acute illness in older people, significantly improved medication appropriateness; this beneficial effect was maintained for 6 months following the intervention [Gallagher et al. 2011]. The STOPP/START criteria have been updated [O’Mahony et al. 2014]. Version 2 of STOPP/START with its 114 criteria represents a 31% increase in the total number of criteria included in version 1.
Country-specific PIM lists
PRISCUS is a consensus list of PIM developed for use in Germany. It consists of 83 drugs and recommendations for monitoring laboratory values, dose adaptation and therapeutic alternatives [Holt et al. 2010]. Patient-focused drug surveillance [Olsson et al. 2010] was developed for older people in NHs in Sweden. The intervention involved a physician-led, patient-focused approach taking into account the patient’s health condition to appropriately optimize medication therapy and reduce polypharmacy. The advantage of this approach was the recognition of the need to discuss benefits and risks of drug therapy with frail older people, accompanied by close monitoring and reevaluation. In addition to the tools mentioned above, in other countries including Australia, France and Norway, specific PIM lists have been developed [McLeod et al. 1997; Naugler et al. 2000; Rancourt et al. 2004; Laroche et al. 2007; Rognstad et al. 2009; Basger et al. 2012].
Prescribing Indicators in Elderly Australians (PIEA) is based on common medical conditions and most common medications used in Australia [Basger et al. 2008]. In a study comparing the frequency and type of PIM, some PIEA criteria detected large numbers of ADEs compared with Beers, STOPP/START and even pharmacist findings, suggesting further refinement may be required [Curtain et al. 2013].
Other suggested explicit approaches
In the process of drug selection, ‘SMART therapeutic objectives’ may enhance therapeutic effectiveness in geriatric patients [Vogt-Ferrier, 2010]. This acronym stands for specific, measurable, acceptable, realistic and well-time-framed goals for each individual medication and is suited for reviewing a patient’s complicated geriatric regimen. Another list of drugs suggested for improving IMUP was entitled Assessing Care of Vulnerable Elders (ACOVE) [Shekelle et al. 2001], a set of quality care indicators. Underprescribing can also be detected with the ACOVE criteria. Geriatric risk assessment Medguide [Lapane et al. 2011] is a clinical informatics tool that generates prospective monitoring plans based on potential risk for falls or delirium within 24 h of NH admission. Its efficacy was evaluated in 25 NHs assessing not only falls and delirium but also hospitalizations and mortality resulting from ADEs.
Drugs with anticholinergic properties have long been regarded as dangerous, particularly in older people. To create the Anticholinergic Risk Scale (ARS) [Rudolph et al. 2008], the 500 most commonly prescribed drugs in the veteran’s administration system were ranked according to anticholinergic potential and assigned a point value; an individual score was calculated by summarizing the points for each drug. The advantages of the ARS score are the ease of calculating the score using a table given in the manuscript and the potential to reduce anticholinergic side effects; however, it could be time consuming and impractical in clinical settings compared with research settings.
A drug burden index (DBI) has been modelled incorporating drugs with anticholinergic or sedative effects, total number of medications and daily dosing [Hilmer et al. 2007, 2009]. Increased DBI was associated with impaired performance, mobility and cognitive status in high-functioning community-based older adults and with increased risk of falls in residents in LTC facilities [Wilson et al. 2011]; the total number of medications was not associated with impaired performance when sedatives and anticholinergics were excluded.
Depending on evidence for safety, efficacy and overall age appropriateness, the ‘Fit for the Aged Criteria’ (FORTA) drug classification ranks drugs into groups from A to D; A: indispensable with obvious benefit; B: proven efficacy but limited effects or possible safety concerns; C: questionable efficacy or safety; and D: avoid [Wehling, 2009]. As an implicit tool, it is only applicable if medical details of the patient are known; the drug selection process and secondary assessments are compiled into a manual for successful, embedded use of FORTA.
CRIME (Criteria to Assess Appropriate Medication Use Among Elderly Complex Patients) represents 19 explicit pharmacological recommendations for coping with IMUP in five common chronic diseases (diabetes mellitus, hypertension, congestive heart failure, atrial fibrillation and coronary heart disease) [Onder et al. 2013]. According to CRIME, conditions related to aging may negatively affect a drug’s benefit–risk ratio and therefore reduce its efficacy. CRIME was developed in Italy by Onder. It only offers recommendations for clinical guidelines of these five diseases to patients with limited life expectancy, functional and cognitive impairment and geriatric syndromes (actually VOCODFLEX).
Implicit tools
The prescribing optimization method (POM) is based on six questions. Is undertreatment present and addition of medication indicated? Does the patient adhere to his/her medication schedule? Which drug(s) can be withdrawn or which drugs(s) is(are) inappropriate for the patient? Which adverse effects are present? Which clinically relevant interactions are to be expected? Should the dose, dose frequency or form of the drug be adjusted? Optimization was significantly better when general practitioners used the POM [Drenth-Van Maanen et al. 2009]. Use of this tool can give the advantage of an open and allowed for clinical judgment that can lead to better prescribing. However, it could be time consuming.
The medication appropriateness index (MAI) uses implicit criteria to measure elements of appropriate prescribing. It consists of 10 elements considered necessary for appropriate prescribing, including indication, effectiveness, appropriate dose, practical and correct directions, absence of interactions, lack of therapeutic duplication, appropriate duration and low cost [Hanlon et al. 1992]. The MAI involves the use of clinical judgment to assess each criterion. The main disadvantages are that it takes at least 10 min to complete the entire tool, and it does not address the underuse of appropriate prescribing. The MAI has been linked to adverse outcomes in smaller studies [Schmader et al. 1997] but has not been extensively used in various larger settings.
Assess, Review, Minimize, Optimize, Reassess (ARMOR) is a functional and interactive evidence-based practice tool designed for the NHS [Haque 2009] (http://www.annalsoflongtermcare.com/content/armor-a-tool-evaluate-polypharmacy-elderly-persons). The tool takes into account patients’ clinical profiles and functional status, the primary goal for using this systematic approach is to improve functional status and mobility. It also incorporates decision making on changing or discontinuing medications. ARMOR has been shown to reduce polypharmacy, healthcare costs and hospitalizations.
In Canada, Moorhouse and Mallery developed the Palliative and Therapeutic Harmonization (PATH) (PATH) program, which provides a standardized, clinical approach to decision making for patients who are frail. The goal was to achieve frailty-specific treatment guidelines to replace conventional CPGs. The PATH model [Moorhouse and Mallery, 2012] offers a standardized clinical approach to the assessment of frailty and simplifies health decisions in older people with multiple health problems. Based on evidence review, the guidelines consider the clinical relevance of commonly accepted outcomes when there is frailty, due to the multiple competing risks of mortality. According to this group, when individuals are severely frail, higher blood pressure targets are preferable and we should taper or discontinue antihypertensive medications to achieve a systolic blood pressure target between 140 and 160 mmHg; these authors see no reason to continue statins in older people who are severely frail. As for diabetes mellitus, the PATH program recommends maintaining hemoglobin A1c (HbA1c) above 8%, meaning that any medication that keeps HbA1c below 8% can be discontinued.
The Garfinkel Good Palliative Geriatric Practice (GPGP) method and algorithm combines EBM, when it exists, with clinical judgment, giving high priority to ethical issues and particularly to patient/family preferences. This was the first method to prove that effective reduction in polypharmacy by simultaneous deprescribing of as many ‘nonlife saving’ medications as possible resulted in significantly improved clinical outcomes. Just like the PATH perception, the GPGP calls for a less aggressive approach in reaching rigid target goals (e.g. blood pressure, serum glucose and lipid concentrations). GPGP has been implemented in both geriatric departments [Garfinkel et al. 2007] and in community-dwelling older people [Garfinkel and Mangin,2010], and was proven beneficial in both. In patients with a disability in nursing departments, the Garfinkel GPGP method was associated with a significant decrease in annual mortality, morbidity and referrals to acute care hospitals, as well as a reduction in costs. Applying this method in community-dwelling independent and frail older people resulted in improved functional, mental and cognitive status, with a high level of patient and family satisfaction. Eighty-four percent of patients reported an improvement in health with no significant adverse reactions to the substantial drug discontinuation. The advantage is that this method is translatable into any setting and combination of drugs and comorbidities; it also addresses underuse of appropriate prescribing. However, it requires current knowledge, beyond a standardized guideline type approach, of the research evidence and some critical appraisal skills in interpreting the research data in the context of the individual patients. The GPGP is time consuming. Its main recommendations include the following: rethinking and reevaluation is needed for each and every drug in the elderly; discuss with the patient/family/guardian the pros and cons of each drug; when no EBM exists, combine clinical judgment with patient/family/guardian preferences, the main goal being QoL; with their consent, stop as many ‘nonlife saving’ drugs as possible, simultaneously; be less aggressive in reaching rigid target goals, for example blood pressure, serum glucose and lipid levels. An important medicolegal byproduct is that having the patient/family/guardian involved in establishing the therapeutic approach reduces the doctor’s fear of lawsuits.
The GPGP approach is not ageist; the authors do not extrapolate from single-disease guidelines in adults to children; there is no rational basis for doing this in VOCODFLEX. Like children, the VOCODFLEX subpopulation is also much more vulnerable to ADEs [Garfinkel and Mangin, 2010]. Therefore, individualization of drug therapy is a must. Obviously, customizing drug therapy in older people not only includes deprescribing but also changing to other drugs with a higher benefit–risk ratio and sometimes new medications if new diagnoses (mostly depression) are established.
The GPGP method was recently suggested as a basic perception in two large publications [Scott et al. 2015; Sengstock et al. 2014].
Barriers to routine deprescribing
Globally, the main obstacle to deprescribing is an emotional, psychological one; the concept seems to counteract and shutter a basic, almost ‘religious’ worldwide belief that we were raised upon, regarding life–death, health–disease and patient–care giver interactions. The good medical doctor is supposed to heal diseases, and throughout history, the patient–doctor interaction has turned out to be perceived as DDI. Nowadays, most people are disappointed if the interaction with any doctor is not eventually translated into some prescription. ‘Ask your GP [general practitioner] to give something for your (whatever) problem’, or ‘at least give me something’, or ‘doctor, you recommend stopping this drug, what will you give me instead?’ All of these have become common idiomatic expressions because intuitively and traditionally the physician is perceived mainly as the expert prescriber who wisely chooses the right medications to treat diseases. This perception is heavily fueled by the diagnostic and drug companies whose main initiative is to define more and more people diagnosed as ‘not healthy’ and therefore ‘must take some medications’. A major breakthrough of the 20th century health perception was highlighting the importance of prevention, proving and persuading societies that not only is a specific cure for a specific disease important, but prevention to postpone complications to a later stage in life may be even more important and possible. The increased rate of overdiagnosis starts a vicious circle leading to many more apparently healthy people taking more and more medications starting earlier and earlier and for a longer period in life, sometimes almost ‘from birth to death’. The main barriers to routine deprescribing are presented in Table 1. The main obstacle is an emotional/psychological global belief based on traditional myths regarding the unique importance of the medical doctor as an expert in prescribing drugs to heal all maladies. Another nonprofessional major factor is the bias created by diagnostics and drug companies whose main incentive is to sell products and make profit. These two major forces form the basis for pressures and barriers, affecting all medical doctors who prescribe. Furthermore, doctors are afraid not to follow current CPGs (not to mention pay for performance issues), even realizing there are no proven CPGs for older people, particularly VOCODFLEX. GPs are afraid of unfavorable consequences even if unrelated to deprescribing, afraid of lawsuits and afraid of their superiors if they do not precisely follow current CPGs. They are also afraid of the patients and their families if they dare to stop drugs recommended by experts. GPs may also be frustrated because they have no EBM RCTs indicating when to stop medications and much uncertainty regarding the effectiveness of strategies to reduce polypharmacy [Anderson et al. 2014; Ostini et al. 2012; Scott et al. 2014].
Summarizing the barriers to routine deprescribing.
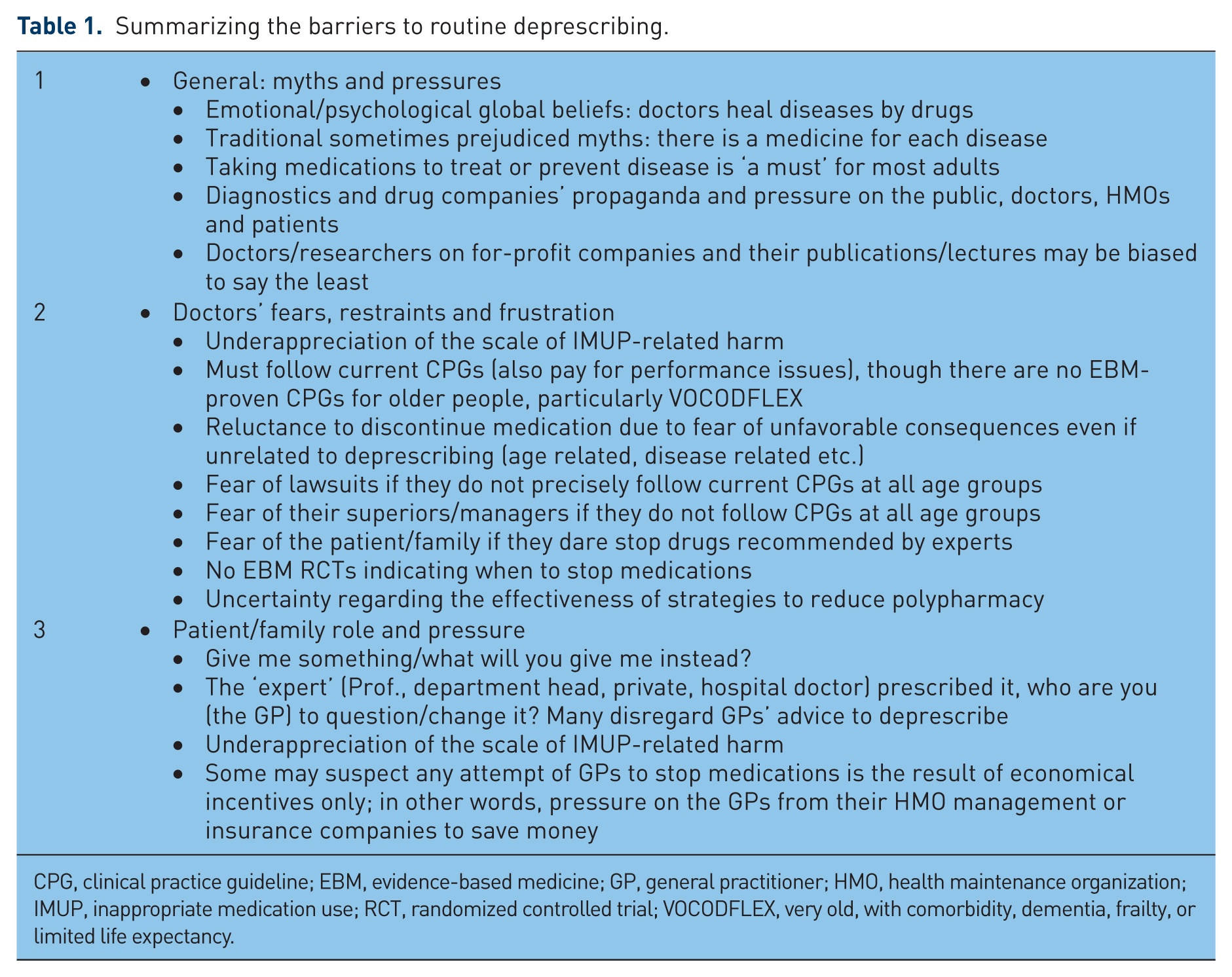
CPG, clinical practice guideline; EBM, evidence-based medicine; GP, general practitioner; HMO, health maintenance organization; IMUP, inappropriate medication use; RCT, randomized controlled trial; VOCODFLEX, very old, with comorbidity, dementia, frailty, or limited life expectancy.
The patient and family also contribute to the negative vicious circle of pressure on medical doctors. Many disregard GPs’ advice to deprescribe unless the ‘expert’ approves (Table 1).
Conclusion and suggestions: a completely new medicine is needed for VOCODFLEX
In a systematic review, Scott and colleagues concluded that, in older patients, the single most important predictor of inappropriate prescribing and risk of ADEs is the number of prescribed medications [Scott et al. 2014]. IMUP is becoming a leading global health and economical problem in general and in older people in particular. Therefore, reducing inappropriate prescribing should be regarded as a leading global goal of the highest priority in the 21st century. Facing the huge negative global consequences of IMUP, an integrated international effort towards the shared goal of reducing the negative impact of IMUP seemed urgent. We therefore established in 2013 ‘IGRIMUP’, the International Group for Reducing Inappropriate Medication Use and Polypharmacy, to provide a focus for those trying to improve medical practice to combat IMUP via information sharing, collaboration and communication, with as many working in the field as possible. At the International Association of Gerontology and Geriatrics - European Region (IAGG-ER) 8th Congress in Dublin, in April 2015, IGRIMUP presented as a group 36 abstracts from 22 different centers of 15 different countries in eight symposia and workshops, each concentrating on another facet of the topic.
In the present article, we review several aspects of IMUP and present current methods suggested to improve the problem. We believe that in each patient, particularly in older people and mostly in the VOCODFLEX subpopulation, rethinking and reevaluation should be performed for each drug. However, the barriers mentioned above will continue to outweigh the enablers, being too high to overcome; most current attempts seem to be only ‘scratching the tip of the iceberg’ and extinguishing the remaining ashes of fires, contributing in very few cases, very little and very late. In order to solve the problem in most older people and give them a better QoL much earlier, for an increased period of time before death, we must change, in a way shutter, our own perceptions regarding good medical practice that have been heavily implanted ‘in our veins’ since medical school and even before as lay people in the 20th century.
For centuries, medical doctors have been raised on the ethical axiom ‘primum non nocera’, meaning do not rush to treat when no treatment is needed. This somewhat sacred rule is brutally shuttered by IMUP [Scott et al. 2014].In the 20th century, strict rules have been established for scientifically introducing new drugs and keeping them on the market. The very simple, basic demand from each medication is that the benefits should outweigh all possible risks or harm (a positive benefit–risk ratio). However, for all drugs the knowledge gap regarding this parameter is increasing in correlation with age, comorbidity, dementia, frailty and limited life expectancy (VOCODFLEX). We implement existing though unproven EBM and CPGs, mostly with a negative benefit–risk ratio in these rapidly increasing and mostly vulnerable subpopulations. Our older patients are in a strange position; they (and we) believe we are acting based on EBM for the benefit of the patient. In reality, this is not the case because we do not really have CPGs for most older people. Doctors’ unawareness of their lack of knowledge represents the highest level of risk for their patients. ‘Knowing that we do not know’, caregivers are much more cautious to prescribe because no one knows whether prescribing would be better than not prescribing. In older people, having no EBM RCTs for most medications, while realizing the harm of IMUP, many physicians feel that deprescribing many nonlife-saving medications represents ‘good clinical practice’.
In line with this reality, one of the authors (DG) has suggested that a completely different approach entitled GPGP is adopted in the 21st century. This approach requires completely new principles and guidelines regarding research, medical education, diagnosis and treatment in older people. First, we must accept the fact that most principles of the so-called good EBM RCTs that researchers have somewhat fanatically adopted in the 20th century are useless and inappropriate in older people, particularly the VOCODFLEX subpopulation. Even inside the study and control groups, heterogeneity is huge as the impact of VOCODFLEX increases; also in deprescribing projects, finding a comparable control group is impossible statistically. In order to do it ‘ properly scientifically’ we should discontinue versus continue (in study and control groups respectively) the same five to eight drugs out of exactly the same 15–20 medications while having comparable demographic and comorbidity characteristics in both groups. This may require sample sizes that are greater than the whole subpopulation in question, maybe more than the world’s population. So ‘traditional’ RCT tools are practically impossible; forget statistics, RCTs, EBM and computers as they are not there to support us. We have not yet arrived at a situation where any computer simulation can show us all the possible interactions among multiple medications, while factoring in the particular characteristics of a specific older patient [Garfinkel 2014].
Completely new research tools are needed for our older VOCODFLEX patients; furthermore, they need answers now, having no time to wait until we solve our confusion or design time-consuming studies that provide decisive results that satisfy our 20th century rigid scientific rules and beliefs. Let us not underestimate the importance of detailed case reports and feasibility studies showing that deprescribing results in significant clinical outcomes. The main reason for this is that the natural history of aging and particularly VOCODFLEX is always bad; all chronic diseases and geriatric syndromes have a one-way direction of negative impacts and deterioration.
Therefore, no statistics are needed to determine that any significant improvement following excessive drug discontinuation is indeed the result of deprescribing. Researches showing such results, even if not traditionally classified as RCTs, should be considered appropriate enough for encouraging doctors to deprescribe, obviously with the consent of the older patient or their family or guardian. Our older patients cannot wait until we have traditional EBM RCTs or computer solutions that accurately define CPGs for their individual optimal drug regimen. In reality, we will never have such information.
If medical doctors do not wake up quickly, our older patients are going to suffer, not only from their inevitable diseases (God’s will if you wish…); sadly and increasingly, their major suffering will be the result of iatrogenic harm due to physicians who, being afraid for themselves, continue to use the wrong ‘sanctified guidelines’ that prevent them from stopping supposedly safe but actually deceiving single-disease CPGs.
We do have the advantage of knowing the exact diagnosis. IMU correlates with the number of drugs, so polypharmacy is the disease, and therefore, the specific treatment is simple: stopping as many medications as possible; in other words, deprescribing is the cure or rehabilitation for IMUP. We still have no consensus as to the best way to deprescribe. In our view and that of others [Steinman et al. 2009], drugs-to-avoid criteria are insufficiently accurate to use as standalone measures of prescribing. The Beers approach or similar tools may be misleading: prescribing 10 to 15 ‘non-Beers list’ medications to patients is still likely to do more harm than good. We must not spend our time, energy and money looking for specific medications that should be avoided, thus artificially separating the bad ‘forbidden drugs’, suggesting in a way that all other drugs or drug combinations are ‘good’ and safe [Garfinkel and Mangin, 2010]. Furthermore, in a state of polypharmacy, the policy of stopping one medication considered ‘inappropriate’ and evaluate the outcomes is not effective and may even be unethical; since we have no idea of all the possible interactions and the whole scope of damage caused by the numerous remaining, supposedly ‘appropriate’ drugs, our main approach should be deprescribing of as many medications as possible simultaneously to cure the 21st century global epidemic we call polypharmacy or inappropriate medication use.
Footnotes
Author’s Note
The authors are members of IGRIMUP - international group for reducing inappropriate medication use & polypharmacy
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.