
Abstract
Objective:
To evaluate (1) the metabolic and endocrine effects of metformin combined with exenatide versus only metformin treatments in patients with polycystic ovary syndrome (PCOS) and abdominal obesity (AO) and (2) to determine the molecular mechanisms by which the combined treatment acts on PCOS patients.
Design:
Randomized controlled trial of PCOS patients with AO to receive combined treatment with metformin–exenatide or metformin alone, and network pharmacology of gene expression in PCOS patients under the combined exposure.
Setting:
Tertiary teaching hospital.
Patients:
Women with PCOS and AO who fulfilled the Rotterdam Criteria under combined treatment with daily cyclical ethinylestradiol (35 μg/day) and cyproterone acetate (2 mg/day).
Intervention:
Patients were randomized to either combined oral metformin (1500 mg/day) and exenatide (2 mg weekly subcutaneous injection, n = 35 women) treatment or metformin alone (n = 31 women) for 12 weeks. Network pharmacological prediction of gene expression under the combined exposure was studied.
Main outcome measures:
(1) Basal and after both treatments anthropometric, endocrine, and metabolic changes were compared. (2) Network pharmacological prediction and gene expression were studied in patients under metformin–exenatide treatment. Venn diagram and Markov Cluster Algorithm diagram of core targets for AO were applied to identify key targets.
Results:
Both treatments displayed (1) reductions of total testosterone, insulin, and lipoprotein levels and (2) increases of high-density lipoprotein cholesterol and apolipoprotein A1. We identified PCOS, AO, and comorbid genes further intersected with 269 combination therapy genes. Network pharmacology identified 154 key PCOS genes for drug regulation, including 29 closely related to AO and metabolism.
Conclusion:
Both treatments improved glucose and lipid metabolism, weakening insulin resistance and improving some biochemical indexes. Network pharmacology identified genes related to AO and metabolism in patients with PCOS under the metformin–exenatide treatment.
Trial registration:
ClinicalTrials.gov NCT04029272.
Plain language summary
The aim of this study was to evaluate (i) the metabolic and endocrine effects of metformin combined with exenatide versus only metformin treatments in patients with polycystic ovary syndrome (PCOS) and abdominal obesity (AO); and (ii) to determine the molecular mechanisms by which the combined treatment acts on PCOS patients. Randomized controlled trial of PCOS patients with AO to receive combined treatment with metformin-exenatide or metformin alone, and network pharmacology of gene expression in PCOS patients under the combined exposure were conducted at tertiary teaching hospital. Women with PCOS and AO who fulfilled the Rotterdam Criteria under combined treatment with daily cyclical ethinylestradiol (35 μg/day) and cyproterone acetate (2 mg/day). Patients were randomized to either combined oral metformin (1,500 mg/day) and exenatide (2 mg weekly subcutaneous injection, n = 35 women) treatment or metformin alone (n = 31 women) for 12 weeks. Network pharmacological prediction of gene expression under the combined exposure was studied. Both treatments displayed (i) reductions of total testosterone, insulin, and lipoprotein levels; and (ii) increases of HDL-cholesterol and apolipoprotein A1. We identified PCOS, AO, and comorbid genes further intersected with 269 combination therapy genes. Network pharmacology identified 154 key PCOS genes for drug regulation, including 29 closely related to AO and metabolism. Both treatments improved glucose and lipid metabolism, weakening insulin resistance and improving some biochemical indexes. Network pharmacology identified genes related to AO and metabolism in patients with PCOS under the metformin-exenatide treatment.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is the most frequent female endocrinopathy during reproductive years, and with health risks even beyond menopause. It is characterized by the presence of menstrual disorders, excessive body weight, metabolic syndrome, hyperandrogenic features, insulin resistance, and increased risk of type 2 diabetes mellitus and nonalcoholic fatty liver disease.1–3 A combination of genetic, endocrine, lifestyle, and environmental factors determines PCOS development, evolution, and severity, being at the same time factors and complications of the syndrome. 4 In addition, genetic and environmental factors are also involved in the development and progress of PCOS.5,6
Network pharmacology provides a system-level approach to understanding drug mechanisms by integrating bioinformatics, pharmacology, and molecular biology. It enables the identification of protein–protein interactions (PPIs) that exhibit how genes and proteins are linked with characteristic clinical conditions, such as PCOS and abdominal obesity (AO). 7 PPIs are complex networks that represent the physical contact between two or more proteins. These interactions are involved in signal transduction, gene expression regulation, metabolic processes, and cell cycle control. Understanding PPIs can provide insights into the underlying mechanisms of various biological processes and diseases, and they are an important area of study in systems biology and bioinformatics. In the modular analysis of PPI networks, researchers identify modules or groups within the network to understand how proteins work together to perform biological functions and as possible markers of PCOS pathogenesis. 8 Each module may contain a set of functionally related proteins that might be involved in specific biological processes or pathways. 9
The correlation of insulin resistance, excessive adipose accumulation, and variable therapeutic responses to combined treatments may have a critical role in PCOS pathophysiology and management. 10 Metformin is a therapeutic option for PCOS patients that has been widely studied. It improves insulin sensitivity in peripheral tissues by reducing hepatic glucose production. 11 New glucagon-like peptide-1 receptor agonist (GLP-1RA) drugs, like exenatide, liraglutide, rosiglitazone, or canagliflozin, have been developed to treat excessive body weight, 12 and have been combined with metformin to improve clinical, biochemical, and endocrine outcomes, and quality of life in PCOS patients.13–15 However, there is limited information concerning the genes that might be involved in the mechanism of action of these compounds. The purposes of this study are (1) to evaluate the clinical, metabolic, and endocrine effects of metformin combined with exenatide treatment compared to only metformin therapy among PCOS patients with AO under daily cyclical ethinylestradiol (EE) and cyproterone acetate (CA) and (2) to study the pharmacological prediction and experimental validation of metformin–exenatide treatment to identify genetic factors that might affect women with PCOS with AO.
Materials and methods
This study was approved by the Ethics Committee of Peking Union Medical College, Chinese Academy of Medical Sciences, and Peking Union Medical College (No. HS-2032), and conducted according to the Declaration of Helsinki. A written informed consent was obtained from all the participants.
Study population and clinical assessment
Patients fulfilling the Rotterdam Criteria of PCOS were invited to participate in the study. 3 They were under combined treatment with cyclical daily doses of EE (35 μg) and CA (2 mg). The exclusion criteria were as follows: (1) The presence of endocrine diseases such as diabetes mellitus, adrenal or thyroid pathology, acromegaly, hyperprolactinemia, androgen-secreting tumors, thyroid disorders, multiple endocrine neoplasia type 2, and any other endocrine disorder. (2) Patients with severe or unstable physical disease, including liver, kidney, cardiovascular, respiratory, neurological, hematological, thromboembolic, and tendency toward thrombosis, malignancies, or mental diseases. (3) Women who smoke or drink heavily. (4) Pregnant women or breastfeeding. (5) Patients treated during the past 3 months with statins or other drugs known or suspected to alter reproductive or metabolic functions. (6) Patients with allergy or intolerance to the studied drugs. (7) Women participating in other clinical trials.
The sample size was calculated based on the average change in body weight; according to the results of existing literature, the estimated weight loss of the combined treatment group was estimated at 2.6 ± 0.5 kg after 12 weeks of therapy. 16 To ensure the stability, accuracy, and reliability of the research results and to achieve the expected efficiency of hypothesis testing, we adjusted the sample size to 35 cases per group. A total of 78 PCOS patients, aged 18–40 years, with a body mass index (BMI) ⩾25 kg/m2 and AO (waist circumference ⩾80 cm) were recruited. They were under treatment with doses of EE (35 μg/day) and CA (2 mg/day) from the first day of menstruation or progesterone withdrawal bleeding for 21 consecutive days, and the next cycle began after 7 days of steroid hormone treatment withdrawal.
Seventy PCOS patients were randomized to either metformin (n = 35, 1500 mg/day) combined with exenatide microsphere injection (2 mg/weekly injection tube (Astra Zeneca Co. Ltd., AstraZeneca UK Limited, Cambridge, United Kingdom), or to metformin-alone treatment (n = 35, 1500 mg/day) and completed the follow-up (Figure 1). Finally, 35 patients treated with metformin and exenatide, and 31 treated with only metformin completed the follow-up. There was a dropout rate of 5.7%. Two patients left the study due to nausea and vomiting, one due to personal reasons, and one due to noncompliance. PCOS patients had clinical examinations including weight, waist circumference, and BMI (kg/m2). Fasting blood glucose and insulin, lipid profile, a 75-g oral glucose tolerance test (OGTT), luteinizing hormone, follicle-stimulating hormone, estradiol, total testosterone (TT), and dehydroepiandrosterone sulfate (DHEA-S) and other variables were measured (Table 1). Physical examination includes weight, waist and hip circumferences, and BMI (weight, kg/height, as m2). In addition, laboratory results include a blood lipid profile, a 75-g OGTT insulin release test, and hormones. Table 1 details measured variables, including anthropometric characteristics, lipids, steroid hormones, apolipoprotein A1, apolipoprotein B, estradiol, TT, and DHEA-S. Lipid, metabolic, and endocrine indexes include total cholesterol, triglycerides, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein cholesterol, apolipoprotein A1, apolipoprotein B, lipoprotein (a), free fatty acid, high-sensitive C-reactive protein, white blood cell count, alanine aminotransferase, and creatinine.

The process of study from screening of PCOS patients with AO to completion during the 12 weeks treatment period. The diagram exhibits patient allocation into metformin-only and metformin–exenatide groups, giving detailed inclusion and exclusion criteria, randomization, and follow-up outcomes.
Clinical characteristics and biochemical data in PCOS patients before and after combined treatment with metformin and exenatide or with only metformin.

DHEA-S, dehydroepiandrosterone sulfate; HDL, high-density lipoprotein; LDL, high-density lipoprotein; ns, not significant; OGTT, oral glucose tolerance test; PCOS, polycystic ovary syndrome.
This study involved the systematic recording of adverse events through direct inquiry at each follow-up visit, prompt self-reporting by providing a dedicated phone number and email, physical examination (such as weight and visible signs) by the study team at baseline and follow-up visits, and clinical laboratory findings especially by blood, liver, and kidney monitoring, followed by their classification into mild, moderate, or severe adverse events. Finally, all the reported adverse events were evaluated to assess their potential linkage with study treatment.
Network pharmacology and gene acquisition of combined metformin–exenatide drug targets
The PCOS and AO medical terminology was inputted into the Human Gene Database GeneCards (version 4.8.0, Weizmann Institute of Science, Rehovot, Israel) to obtain disease gene targets. 17 GeneCards were searched to obtain gene targets linked with PCOS and AO. For the combined metformin–exenatide treatment, we focused on intersecting genes relevant to PCOS and AO. While metformin-specific genes were not analyzed independently, the approach underscored the combined treatment effects, as metformin’s modes are well-studied in PCOS management. Future studies should emphasize metformin-specific gene interactions for better network analysis. The next step was the target acquisition and analysis of the metformin–exenatide combined treatment for patients with AO. The next step was to import key targets into Metascape, select humans, use the Markov Cluster Algorithm for clustering, and set the inflation parameter to 5. Key targets were introduced into Metascape, and species were selected as humans for bio-enrichment analysis (biological process, molecular function, and cell composition). Finally, bioinformatics was used to draw a cubic graph diagram of bio-enrichment analysis and a bubble diagram of pathways according to the degree of enrichment.18,19
Randomization process
Before the commencement of the study, a randomization list with two groups was generated by a statistician not otherwise engaged in the study. A laboratory technician consecutively allocated participants to the respective treatment groups according to this list.
Statistical analyses
The Shapiro–Wilk test was used to determine whether variables were normally distributed. Results are reported as means ± standard deviations, or medians and quartiles. The normally distributed data were tested by paired sample t-tests, for intra-group and inter-group comparisons. The nonnormal distribution data were analyzed with the Mann–Whitney U-test or the Wilkerson signed-rank tests. For categorical data, we use the Chi-squared test. Differences were considered significant for p < 0.05. Statistical analysis was performed using the IBM SPSS 26.0 software, IBM Corporation, New York, USA.
Results
Clinical study of PCOS patients
Table 1 displays the anthropometric characteristics, metabolic and endocrine results, and other variables for both groups of studied PCOS patients. There were significant reductions in blood glucose after 120 min of the OGTT in both studied populations and significantly lower insulin after 2 h of the OGTT in women under the combined treatment but not in women treated only with metformin. Blood triglycerides, HDL-cholesterol, and apolipoprotein A1 levels were significantly increased with both studied treatments. Total circulating testosterone levels were significantly reduced after both treatments. There were no other changes in measured related variables in women with both treatments (Table 1).
Target acquisition of combined metformin–exenatide therapy genes
The 269 genes indentified for the combined exenatide-metformin therapy were sourced through systematic integration of data from GeneCards and Metascape. GeneCards provided comprehensive lists of 6495 genes associated with AO and 4103 genes associated with PCOS. The 1269 gene were recognized via the integration of GeneCards and Metascape, underscoring overlaps between PCOS, AO, and the drug-specific targets of metformin and exenatide. Overlaps between drug-specific targets (metformin and exenatide) and disease-linked genes (PCOS and AO) were analyzed using a Venn diagram, resulting in 269 intersecting genes. The 269 genes underwent clustering and functional enrichment analysis via Metascape. The results highlighted key pathways related to glucose and lipid metabolism, as indicated by significant enrichment of genes involved in adipocytokine signaling, insulin resistance, and Peroxisome Proliferator-Activated Receptor (PPAR) signaling pathways. Among these, PPARγ and IRS1 emerged as core genes due to their central roles in regulating glucose homeostasis, lipid metabolism, and insulin signaling, as identified in the pathway enrichment analysis. Figure 2 shows that among the 269 combination targets, 8 genes were involved in the PCOS treatment alone, 56 genes in AO alone treatment, and 154 key genes involved in the combined drug treatment with AO characteristics. Among the 154 intersecting genes, core genes such as PPARγ and IRS1 were prioritized on the basis of their central contributions in glucose and lipid metabolism pathways. These genes may act as crucial targets for future therapeutic interventions. In addition to the 154 key genes that were the focus of our study, there were 2702 crossover genes of AO and PCOS to be further developed. Figure 3 shows 154 key genes identified using the Markov clustering algorithm. Five modules were clustered, forming a network of 142 nodes and 2370 edges: average node degree was 33.4, the local clustering coefficient was 0.648, the expected number of edges was 764, and PPI enrichment. 20 The red color block with a large number of clustered genes, the module accounts for a large proportion of the overall gene, indicating that the PCOS onset of this type of patient is mainly related to abnormal glucose and lipid metabolism. When the body has impaired glucose tolerance, fat mobilization is reduced, and its accumulation increases, which is not only the body characteristic of this group of women who become obese in a visible form. Also, it will be effectively converted into invisible forms, such as affecting cholesterol metabolism and maintaining the normal physiological functions of women, which in turn promotes an increase in the levels of hormones that maintain masculine phenotype characteristics. Secondly, the number of light-yellow modules show combined defects in oxidative phosphorylation and fatty acid beta-oxidation in mitochondrial disease.

Venn diagram showing the overlap of gene targets recognized for PCOS, AO, and combined metformin–exenatide treatment. The 269 genes were identified as targets of the combination therapy (metformin–exenatide). Among these, 154 genes overlapped (intersected) with PCOS- and AO-related genes. Further analysis identified 29 key genes specifically associated with AO and metabolism.

Markov Cluster Algorithm clustering diagram showing the core gene modules from the 269 intersecting targets for PCOS and AO under combined metformin–exenatide treatment. The network comprises 142 nodes and 2370 edges, with clusters indicating functional modules involved in glucose and lipid metabolism. Key targets including PPARγ and IRS1 are highlighted, underscoring their central role in the therapeutic pathways.
Figure 4 shows the results of the bio-enrichment analysis arranged by the score size where the biological process displayed phosphatidylinositol 3-kinase complex, and very-low-density lipoprotein particles are key cell components (orange bar graph). The biological function of the drug by binding to the insulin receptor (purple) positively regulates the metabolism of glycogen and fat, and the ameliorating effect of this biological process (green) on the condition needs to be further confirmed by clinical trials. Figure 5 displays the Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analyses. 21 The study shows that it is related to the adipocytokine signaling pathway, FoxO signaling pathway, longevity regulating pathway, and insulin resistance. As shown, (1) the larger the bubble the more genes it contains; (2) the redder the color the larger the p-value; and (3) the higher the degree of enrichment, the more important it is. The analysis shows that involved genes are related to (1) adipocytokine signaling pathway, (2) FoxO signaling pathway, (3) longevity regulating pathway, and (4) insulin resistance.
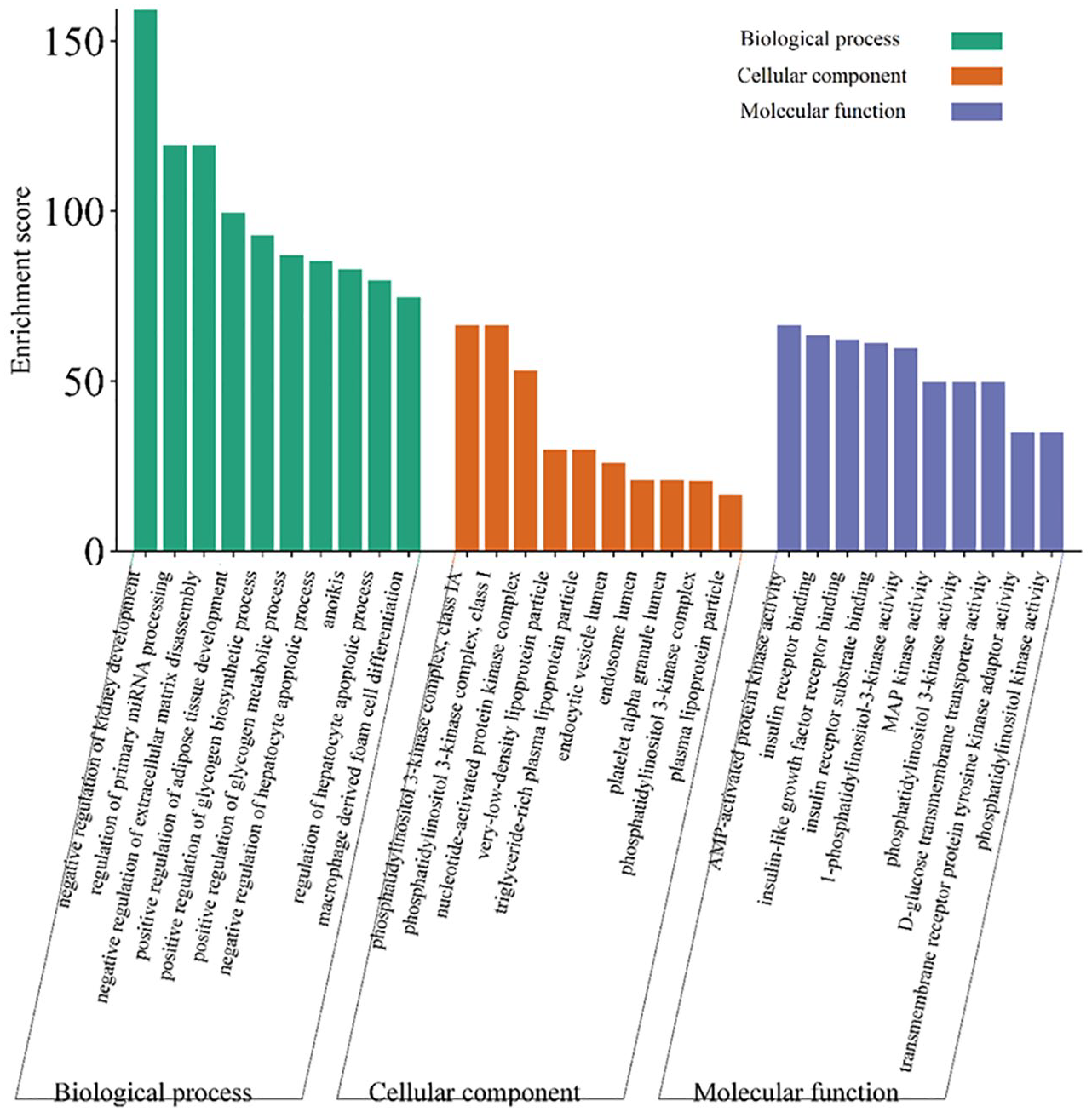
Cubic graph diagram of bio-enrichment score analyses and biological process, cellular component, and molecular function of PCOS patients under combined treatment with metformin and exenatide and combined contraceptive with cyclical daily EE and CA contraceptive treatment. Ten biological processes (e.g., regulation of lipid metabolism), 10 cellular components (e.g., P13K-kinase complex, VLDL particles), and 10 molecular functions (e.g., insulin receptor binding) were identified in these patients.

Bubble diagram of Kyoto Encyclopedia of Genes and Genomes pathway analyses and enrichment showing different factors involved in PCOS under treatment with metformin and exenatide. Larger and redder bubbles indicate pathways with higher enrichment scores and significance. Key pathways are adipocytokine signaling, longevity regulating, and insulin resistance, which altogether narrate the molecular mechanisms involved in the noted clinical improvements.
Discussion
We reported the clinical, metabolic, and endocrine results in Chinese women with PCOS under combined EE-CA submitted to treatment with the combined metformin–exenatide or only metformin treatments. We updated our previous clinical results with a small sample of PCOS patients, 16 and the current studied population provided more clinical and endocrine–metabolic details without significant changes in BMI and anthropometric outcomes. This finding might be related to the fact that the studied women were under combined treatment with a combined EE-CA contraceptive in both groups of studied PCOS patients. We also provide network pharmacological information of the combined treatment with exenatide+metformin showing that genes related to AO, PCOS, and 269 genes involved in the combined therapy of PCOS patients.
Endocrine and metabolic findings
Both study groups received EE and CA as part of their baseline therapy. While EE and CA are generally recommended in PCOS therapy to regulate menstrual cycles and diminish androgen levels, it is observed that their impact on body weight, lipid metabolism, and hormonal regulation could have affected the outcomes of the combination therapy. EE and CA are reported to influence metabolic variables, including increased triglyceride levels and modified glucose metabolism. Especially, EE caused weight gain and modified lipid profiles in some patients, while CA exerted an anti-androgenic effect that may diminish serum testosterone levels. These factors may partially mask the impact of metformin–exenatide combination, particularly in association with weight loss and insulin sensitivity, as noted our study. Nonetheless, the potential interference of EE and CA in the explanation of the combined therapy’s influence should be considered when assessing the results. However, the addition of EE and CA in both treatment groups was necessary for standardizing the treatment regimen in women with PCOS and AO. Future studies could be aimed to investigate the impact of combined metformin–exenatide therapy in PCOS patients who were not using oral contraceptives to better isolate the role of the individual drugs.
This contraceptive treatment is well tolerated, although may produce some side effects such as weight gain, breast tenderness, an increase of triglycerides and glucose levels, and other consequences among PCOS patients. 22 In our clinical study, we found that patients under EE-CA contraception treated with metformin alone or combined with exenatide did not reduce their body weight as expected when patients did not receive EE-CA. A recent meta-analysis reported that the combination of EE-CA treatment combined with metformin results was inferior on different outcomes compared with the metformin-alone treatment: metformin lowered insulin and triglyceride levels, and the association of EE-CA was inferior on insulin markers compared with combined hormones. 23
GLP-1RA drugs have been used in PCOS patients as monotherapy or combined with metformin, being effective in reducing weight and improving glucose and androgen levels.15,24,25 A previous randomized trial of PCOS patients compared the effect of the EE-CA contraceptive alone or combined with either metformin, orlistat, or metformin+orlistat on different hormones and body composition outcomes. 26 Exenatide is a drug frequently used for diabetes therapy, and its use is growing in overweight PCOS patients improving lipid, glucose, and amino acid metabolism, insulin resistance, and oxidative stress. 27 Our results suggest that the clinical effects of the combined treatment with metformin and exenatide may be driven by complementary modes targeting glucose and lipid metabolism pathways. This hypothesis is supported by our network pharmacology findings, where pathway enrichment analysis identified key genes (PPARγ, IRS1) involved in glucose homeostasis and lipid metabolism. These molecular targets align with the observed improvements in insulin resistance, androgen levels, and lipid profiles in the clinical trial, reinforcing the mechanistic basis of the therapy. Metformin mainly increases insulin sensitivity by activating Adenosine Monophosphate (AMP)-activated protein kinase and reducing hepatic gluconeogenesis, resulting in improved glucose uptake and lipid oxidation. Exenatide, a GLP-1 receptor agonist, stimulates insulin secretion, inhibits glucagon release, and delays gastric emptying, thereby ameliorating postprandial glucose regulation. Network pharmacology recognized PPARγ and IRS1 as targets, both of which are important regulators of glucose and lipid metabolism. 25 PPARγ, known for its role in adipogenesis and lipid storage, assists the redistribution of adipose tissue and increases insulin sensitivity. IRS1 mediates insulin signaling by enhancing downstream activation of the P13K-Akt pathway, necessary for glucose transport and glycogen synthesis. The combined therapy possibly synergizes these pathways, as shown by the enrichment of genes involved in the adipocytokine and insulin resistance signaling pathways. 11 These mechanisms are in accordance with the noted clinical advantages, such as reduction in insulin resistance, androgen levels, and improvements in lipid profiles. In PCOS patients with excessive body weight, the combined treatment with metformin and exenatide improved menstrual rhythm, ovulation rate, androgen outcomes, insulin sensitivity, and reduced fat mass. 28 Devarbhavi et al. 29 compared the effect of exenatide, metformin, and the combination therapy for 12 weeks in patients with PCOS and prediabetes, obtaining a remission rate of prediabetes in 64% of women under combined treatment, 56% under exenatide, and 32% under metformin. In addition, exenatide was associated with higher postprandial insulin secretion compared to metformin alone. 30
The observed decrease in TT levels and improvements in lipid profiles with the combined therapy could be associated with the inhibition of androgen synthesis through modulation of key enzymes, such as aromatase and 17alpha-hydroxylase, which are indirectly modulated by insulin and adipocytokine signaling. Metformin’s effect on hepatic insulin sensitivity may diminish ovarian androgen release, while exenatide’s weight reducing features enhance hyperinsulinemia-induced ovarian dysfunction. These results align with previous findings, arguing that combination therapies targeting multiple metabolic pathways provide better outcomes in PCOS patients compared to monotherapy.
In the present study, we evaluated the combined effect of exenatide and metformin compared to metformin alone in PCOS women under combined EE-CA treatment, finding that there was no improvement in weight probably due to the contraceptive steroid hormones since there is evidence that this endocrine treatment is associated with significant increases in body weight, total cholesterol, triglycerides, and sex-hormone binding globulin. Therefore, PCOS patients under complex combined endocrine treatments as reported here should receive instructions to reduce caloric ingestion and increase physical activity to overcome the effect of the used contraceptive on body weight.
Network pharmacological prediction of gene expression
In this study, network pharmacology assisted the recognition of important gene targets and pathways involved in therapeutic impact of metformin and exenatide, for instance, PPARγ and IRS1 genes. These results exhibit the use of network pharmacology concluding the molecular basis of combination therapies for PCOS and AO, especially in associating clinical outcomes to the involved biological mechanism.
The interpretation and verification of clinical results and understanding of the biological significance is a complex task to integrate pharmacological results to understand. 31 Key genes involved in PCOS and elucidating their mechanisms of action are important to improve clinical management and treatments. 32 Zhang et al. 33 reported the 327 genes potentially involved in PCOS patients with hyperandrogenism and normal androgen levels using PPI networks, and of which MYC, CAV1, and HGF were mainly related in the cancer pathway. Zhang et al. 34 identified key genes involved in type 2 diabetes mellitus and PCOS.
The recognition of the 29 genes closely linked to AO and metabolism was acquired through a multi-step process utilizing network pharmacology and bioinformatics tools: (1) For gene selection and data sources, GeneCards was used to extract genes linked with PCOS (4103 genes) and AO (6495). Simultaneously, drug targets for metformin and exenatide were acquired. Venn diagram analysis was conducted to screen 269 intersecting genes that overlapped between PCOS, AO, and the combined metformin–exenatide therapy. (2) For bioinformatic analysis, the 269 genes were put to clustering and functional enrichment analysis using Metascape. This involved the use of the Markov Clustering Algorithm to group genes into functional modules on the basis of their participation in biological pathways. (3) For pathway enrichment and prioritization, genes were enriched in pathways relevant to metabolism, including the adipocytokine signaling pathways, FoxO signaling pathways, and insulin resistance pathways, as found via KEGG analysis. PPARγ and IRS1 emerged as central nodes within these pathways because of their considerable contribution in glucose metabolism. (4) Of the 269 genes, 29 were observed as closely associated with AO and metabolism on the basis of their participation in core regulatory pathways and their biological relevance to glucose homeostasis, lipid metabolism, and insulin sensitivity. These genes were prioritized for their assessment owing to their ability as therapeutic targets for PCOS and AO.
Further cohort studies in PCOS patients without EE-CA treatment are needed to define the roles of genes in PCOS endocrine disorders, body weight changes, and clinical response to treatments. Previous evidence suggests the involvement of genes and common polymorphism variants in PCOS pathogenesis and etiology.
Limitations and strengths
Chinese ethnicity, lifestyle, and nutrition might influence the results, and further studies should be provided on other populations with different characteristics.35,36 A comparison between the use of combined EE-CA hormone therapy in PCOS along with patients not receiving hormone contraception is needed. This randomized trial presents useful findings about the metabolic and endocrine impact of the combined metformin and exenatide therapy compared to metformin monotherapy in PCOS patients with AO undergoing EE-CA contraceptive treatment. A notable strength is the study’s potential to exhibit how hormonal contraceptives may manage weight and BMI reductions generally noted with these treatments, emphasizing the complications of treating PCOS under combined therapies. Moreover, the integration of network pharmacology proposes an innovative direction by recognizing key gene targets (PPARγ and IRS1) and pathways involved in glucose and lipid metabolism, guiding to a molecular framework to comprehend the additive effects of the combined therapy. This approach advances the field associating clinical findings to specific genetic modes, making a way for targeted therapeutic approaches in PCOS management.
It is stated that the analysis did not involve a metformin-only group for target recognition. This limitation could affect the explanation of genes specific to the combined treatment versus metformin only. Adding metformin-specific targets may provide additional findings into the differential effects of the two therapies and should be pursued in the future studies. While network pharmacology provided preliminary insights, further experimental confirmation, such as gene expression investigations in cell models, is needed to validate the modes underlying the combined therapy.
Conclusion
PCOS patients under EE-CA contraceptive treatment show some benefits from either treatment with metformin and exenatide or metformin alone. Genes play a pivotal role in the occurrence of PCOS with AO, and genes that might influence the PCOS clinical, endocrine, and metabolic course, and the response to combined treatment with metformin and exenatide in PCOS patients under EE-CA contraception. Future directions should address research about the gene differences among women with PCOS with and without AO or even other dominant variables or variants of the syndrome like dominant cases of hyperandrogenism, insulin resistance, muscle strength, or body composition.
Footnotes
Acknowledgements
Aijun Sun provided lab facilities for this study.