
Abstract
Introduction
Polycystic ovary syndrome (PCOS) is a common endocrine/metabolic disorder in women of reproductive age, characterized by chronic anovulation and hyperandrogenism. PCOS affects 5–10% of women of reproductive age, and is responsible for 50–70% of cases with anovulatory infertility. Therefore, PCOS is the most frequent cause of anovulation infertility and probably the most common endocrine disorder among women.
PCOS is characterized by oligomenorrhea or amenorrhea, hyperandrogenism (the findings of hirsutism, acne, increasing androgen hormone plasma level or combinations of these conditions) [Leo et al. 2003]. It has long been recognized that PCOS is frequently associated with insulin resistance accompanied by compensatory hyperinsulinemia. In the early stages of insulin resistance, hyperinsulinemia occurs as an effort to maintain glucose tolerance.
The insulin resistance with hyperinsulinemia has an important role in initiating hyperandrogenism through the increase in ovarian androgen hormone biosynthesis. In addition, insulin resistance and the resultant hyperinsulinemia increases the risk of long-term metabolic disorders, such as impaired glucose tolerance and type 2 diabetes, as well as cardiovascular disease. It is estimated that 44% of women with PCOS suffer from obesity and it is characterized by the distribution of central fat. In PCOS, hyperinsulinemia, dyslipidemia and/or hypertension are strongly related with obesity, which itself will aggravate the clinical symptoms [Panidis et al. 2003].
Obesity is related to an increase in adipose tissue produced by many adipocytokines, which are known to have a substantial connection with insulin resistance [Carmina et al. 2005]. Adiponectin and resistin are adipocytokines produced by adipose tissue with contradictory effects, and both are implicated in linking obesity with insulin resistance, type 2 diabetes and cardiovascular disease (CVD).
Decreased adiponectin levels are associated with obesity, coronary artery disease, type 2 diabetes and insulin resistance [Lindsay et al. 2002; Weyer et al. 2001; Hotta et al. 2000] In contrast, elevated resistin level is associated with obesity and insulin resistance [Azuma et al. 2003].
Insulin resistance and hyperinsulinemia are established pathogenic mechanisms for hyperandrogenism in PCOS patients, and the adipokines adiponectin and resistin, among other molecules and hormones secreted by adipose tissue, have been proposed to play a role in the pathogenesis of PCOS [Carmina et al. 2005]. Serum adiponectin level is low in PCOS patients [Pangaribuan et al. 2006; Panidis et al. 2003; Carmina et al. 2005] due to the concurrence of insulin resistance [Pangaribuan et al. 2006; Sepilian and Nagamani, 2005]. A similar causal relationship is seen due to the high serum resistin levels in PCOS [Panidis et al. 2004; Carmina et al. 2005]. Resistin was originally described as an adipocyte-derived polypeptide that provided the link between obesity and insulin resistance [Steppan et al. 2001; Holcomb et al. 2000].
As obesity possibly acted as a major confounding factor in this study in the results published to date [Pangaribuan et al. 2006], this part of the study is aimed at defining the influence of the serum levels of adiponectin and resistin on PCOS, and assessing possible correlations with the hormonal and metabolic parameters of the syndrome based on the body mass index (BMI) status.
Research methods and procedures
Study participants
This study continued a case—control study that had finished recruiting 24 subjects of reproductive women with PCOS as case group, and 24 subjects of normal ovulatory reproductive women, without hyperandrogenism, as a control group. Because the study was aimed at exploring further the contribution of obesity, only 18 subjects of the control group were included in the data analysis. The other six subjects who were obese based on the BMI ≥25 kg/m2 [The Asia Pacific Perspective, 2002] were excluded. In this study, patients’ data were divided to three subgroups. A total of 24 PCOS patients of reproductive women, aged between 20 and 40 years, all of whom were outpatients at the Obstetrics and Gynecology Clinic of Hasan Sadikin Hospital in Bandung, and Akademik Hospital in Makassar, were included as the case group in the study. The case group was allocated into two subgroups, group A (n = 14) women had PCOS + BMI≥25 kg/m2; group B (n = 10) had PCOS + BMI <25 kg/m2. Subsequently, 18 subjects of the control group with BMI <25 kg/m2, aged between 20 and 40 years were included in this study as group C. The women with PCOS had been diagnosed using the Rotterdam consensus [The Rotterdam ESHRE/ASRM – Sponsored PCOS Consensus Workshop Group, 2004]. Informed consent was obtained from all 42 women, and the study was approved by the Institutional Ethical Clearance Board of Hassanuddin University.
Clinical and anthropometrical variables, BMI and clinical blood pressure were determined in all of the subjects. Blood samples were collected between days 3 and 5 of a spontaneous menstrual cycle, at 07:00 to 09:00, after overnight fasting. Blood samples were drawn for the measurement of serum gonadotropins levels (follicle-stimulating hormone [FSH] and luteinizing hormone [LH]), total testosterone, estradiol, prolactin, sex hormone-binding globulin (SHBG), glucose, insulin, adiponectin and resistin. The FSH:LH ratio was also calculated. The Homeostasis Model of Assessment—Insulin Resistance (HOMA-IR) index was calculated using the formula: fasting glucose (mmol/l) × fasting insulin (μIU/ml)/22.5.
Assay methods
All assays of hormonal levels and plasma glucose were performed at Prodia Clinical Laboratory.
Glucose serum level determinations were performed using a glucose oxidase technique with an autoanalyzer. LH and FSH were measured with a competitive chemiluminescent enzyme immunoassay technique, using commercial kits (LH® Siemens Advia Centaur and FSH® Siemens Advia Centaur). Testosterone was measured with an electrochemiluminescent immunoassay technique, using commercial kits (Testosterone II Cobas, Roche). SHBG were measured with electrochemiluminescent immunoassay technique (SHBG Cobas, Roche), and insulin with a competitive chemiluminescent enzyme immunoassay technique (Immulite® 2000 Insulin). Adiponectin levels were measured with a quantitative sandwich enzyme immunosorbent assay technique, using commercial kits (Human Adiponectin ELISA kit for Total and Multimers, Daiichi Pure Chemicals®), and resistin with a sandwich enzyme immunoassay technique (Human Resistin ELISA, BioVendor Laboratory Medicine Inc.).
Statistical analysis
Statistical analyses were performed using SPSS software v.16. All data were given as mean ± SD unless otherwise stated. All values did not achieve a more normal distribution after log-transformation, except for adiponectin. Mean values of adiponectin were compared with the analysis of variance (ANOVA) test, and others with the Kruskal–Wallis test. Means between every groups of every parameters were compared with a post hoc ANOVA test and Mann–Whitney U-test for adiponectin and other parameters, respectively. Relationships between serum adiponectin and resistin levels, and also resistin-to-adiponectin ratio (R:A) to each parameter, were evaluated by calculation of Spearman’s correlation coefficient. Adiponectin and R:A in this study had normal distributions significantly, then independent relationships between them and those parameters to which they were found to correlate significantly were assessed using multiple linier regression analysis. We considered p < 0.05 as statistically significant.
Results
The clinical features of the PCOS and control groups are shown in Table 1. The ages of the women that had PCOS and were obese (group A) were higher than those with PCOS who were not obese (group B) and than those women in the control group (group C).Hormonal and metabolic characteristics are shown in Table 2. LH levels were higher in women with PCOS + normal BMI (group B) compared with women with PCOS + BMI ≥25 kg/m2 (group A), but this difference was not statistically significant. LH levels were significantly higher in women with PCOS + BMI ≥25 kg/m2 (group A) compared with controls (group C, p < 0.001), and in women with PCOS + normal BMI (group B) compared with control (group C, p < 0.05). Women with PCOS + BMI ≥25 kg/m2 (group A) and controls (group C) had lower FSH levels compared with women with PCOS + normal BMI (group B), but this difference was not significant. The LH:FSH ratio values in women with PCOS were significantly lower than controls (group A versus C, p < 0.001; group B versus C, p < 0.05), and not significantly different between women with PCOS + BMI ≥25 kg/m2 (group A) and PCOS + normal BMI (group B).
Clinical features of study samples.

Values expressed as mean ± SD; values in parentheses are ranges.
PCOS, polycystic ovary syndrome; BMI, body mass index; NS, not significant.
Hormonal and metabolic parameters of study samples.

Values expressed as mean ± SD; values in parentheses are ranges.
LH, luteinizing hormone; FSH, follicle-stimulating hormone; SHBG, sex hormone-binding globulin; HOMA-IR, Homeostatic Model of Assessment—Insulin Resistance; R:A ratio, ratio of resistin to adiponectin; NS, not significant.
Compared with controls, women with PCOS had significantly higher serum levels of testosterone (group A versus C, p < 0.001; group B versus C, p < 0.05), and there was no significant difference in testosterone level between group A and group B. SHBG levels were lower in women with PCOS than in the control, but only women with PCOS + BMI ≥25 kg/m2 (group A) had significantly different levels compared with the control (p < 0.005).
PCOS is frequently associated with insulin resistance accompanied by compensatory hyperinsulinemia and obesity. The degree of insulin resistance, which was greater in women with PCOS, was found to be exacerbated by obesity. In this study, insulin resistance was assessed by HOMA-IR value. In women with PCOS + BMI ≥25 kg/m2 (group A) the value was significantly higher than in the control group (group C, p < 0.005). There was no significant difference in HOMA-IR value between PCOS + BMI <25 kg/m2 (group B) and control (group C), and between PCOS + BMI ≥25 kg/m2 (group A) and PCOS + BMI <25 kg/m2 (group B).
Serum adiponectin levels in women with PCOS + BMI ≥25 kg/m2 (group A) were significantly lower than women with PCOS + BMI <25 kg/m2 (group B, p < 0.05) and control (group C, p < 0.001), whereas no significant difference existed between women with PCOS + normal BMI (group B) and controls (group C).
Serum resistin level was higher in women with PCOS + BMI ≥25 kg/m2 (group A) than in women with normal BMI (group B) and the control group (group C), whereas no significant difference existed between all groups. The summarized values of BMI and HOMA-IR, serum concentrations of SHBG, testosterone, adiponectin and resistin, are shown in Figure 1. However, the ratio of resistin to adiponectin (R:A ratio) was significantly higher in women with PCOS + BMI ≥25 kg/m2 than in women with PCOS + BMI <25 kg/m2 (p < 0.05) and controls (p < 0.005), whereas no significant difference existed between women with PCOS + normal BMI and control (Figure 2).

Body mass index (BMI), Homeostasis Model of Assessment—Insulin Resistance (HOMA-IR) and concentrations of sex hormone-binding globulin (SHBG), testosterone, adiponectin and resistin, in women with polycystic ovary syndrome (PCOS) and controls.

Resistin-to-adiponectin ratio (R:A ratio) in women with polycystic ovary syndrome (PCOS) and controls.
Calculation of Spearman’s correlation coefficient showed that the change in serum adiponectin was negatively correlated with changes of LH, LH:FSH ratio, testosterone, HOMA-IR and BMI, and positively correlated with changes of SHBG (Table 3).
Correlation of serum adiponectin level with hormonal and metabolic parameters.

LH, luteinizing hormone; FSH, follicle-stimulating hormone; HOMA-IR, Homeostatic Model of Assessment—Insulin Resistance; SHBG, sex hormone-binding globulin; BMI, body mass index.
ρ = Spearman’s correlation coefficient, p* = significance value of multiple linier regression analysis.
Considering that women with PCOS in group A and group B, and the control group differed in serum LH levels, LH:FSH ratio, BMI, hyperandrogenemia and insulin resistance, the decrease in serum adiponectin levels observed in women with PCOS groups could be related to any of these variables. To further explore these influences, this study applied multivariate linear regression analysis, considering women with PCOS subjects and controls as a whole, with serum adiponectin concentrations as the dependent variable and LH, LH:FSH ratio, testosterone, HOMA-IR and BMI as independent variables. The results found that the change in serum adiponectin level was negatively correlated with changes of testosterone and insulin resistance (HOMA-IR) (Table 3).
Bivariate correlation analyses were performed to assess relationships of R:A ratio with variables of hormones (LH, LH:FSH ratio, testosterone), insulin resistance (HOMA-IR) and BMI. Furthermore, the findings for the bivariate correlation analyses were explored using multivariate analysis to control for potential confounders. The results showed that the change in R:A ratio was positively correlated with changes of LH:FSH ratio, HOMA-IR and BMI, and negatively correlated with changes of SHBG. The multivariate results showed that the change of R:A ratio was negatively correlated with changes of BMI (Table 4).
Correlation of R:A ratio with hormonal and metabolic parameters.

LH, luteinizing hormone; FSH, follicle-stimulating hormone; HOMA-IR, Homeostatic Model of Assessment—Insulin Resistance; SHBG, sex hormone-binding globulin; R:A ratio, ratio of resistin to adiponectin.
ρ = Spearman’s correlation coefficient, p* = significance value of multiple linier regression analysis.
Discussion
The results of the present study showed that PCOS patients have hypoadiponectinemia and that this finding is dependent on obesity state. It has been established that adiponectin is almost exclusively produced in adipose tissue [Berg et al. 2002]. In this study serum adiponectin levels were found to be significantly lower in women with PCOS + BMI ≥25 kg/m2 compared with women with BMI <25 kg/m2, with or without PCOS. No difference was found in adiponectin levels between group B and C, women with BMI <25 kg/m2 and the control group. This significant negative correlation between adiponectin concentration in the serum and BMI was also observed and is shown in Figure 3. These findings agrees with the results of others, who established adiponectin as the only adipokine that is suppressed by increased body fat [Panidis et al. 2003; Tschritter et al. 2003; Weyer et al. 2001].

Correlation of body mass index (BMI) with serum adiponectin levels.
Insulin resistance of PCOS and its compensatory hyperinsulinemia are most marked when there is an interaction between the syndrome and obesity. This study showed that HOMA-IR values, as a parameter of insulin resistance, in PCOS women with and without obesity were significantly different to the women in the control group. Also, serum testosterone levels were found to be significantly different in PCOS women with and without obesity compared with women in control groups. It suggests that insulin resistance and hypertestosteronemia are actively involved in the pathogenesis of PCOS in women with or without obesity.
Bivariate correlation analysis, showed that adiponectin levels were significant negatively correlated with HOMA-IR, BMI and testosterone levels, but significantly positively correlated with SHBG levels. It has been suggested that hypoadiponectinemia associated with obesity and the metabolic syndrome might be a consequence of increased adiposity and/or insulin resistance [Xita et al. 2005]. This study showed that hypoadiponectinemia is associated with HOMA-IR and BMI. As mentioned, serum adiponectin levels were found to be significantly lower in women with PCOS + BMI ≥25 kg/m2 compared with women with BMI <25 kg/m2, with or without PCOS. That is, adiponectin levels were found to correlate significantly with some obesity-associated parameters. This finding might indicate the involvement of adiponectin in the dysregulated metabolic state of PCOS. A significant negative correlation between serum adiponectin levels with BMI and insulin resistance (HOMA-IR) is shown in Figures 3 and Figure 4. Hypoadiponectinemia might contribute to insulin resistance in women with PCOS, because adiponectin normally reduces the triglyceride content of muscle, upregulating signaling and activates of PPAR-γ, increasing fatty acid combustion and energy combustion, and by activating AMP-activated protein kinase, adiponectin enhances muscle fat oxidation and transport, which inhibits the expression of gluconeogenic enzymes, reducing hepatic glucose production [Kadowaki and Yamauchi, 2005]. Furthermore, a significant and independent correlation with testosterone levels was observed (Figure 5), and this suggests an interaction between adiponectin and steroid synthesis or action.

Correlation of Homeostasis Model of Assessment—Insulin Resistance (HOMA-IR) to serum adiponectin levels.

Correlation of circulating testosterone to serum adiponectin levels.
This study showed that serum SHBG levels are reduced in PCOS, and the reduction is further induced by obesity. Nonetheless, serum testosterone levels are induced in PCOS and the increase is further induced by obesity, and similar to HOMA-IR as insulin resistance parameter (Figure 1). Furthermore, prenatal androgen exposure leading to abdominal adiposity and insulin resistance during adult life has been proposed recently to play a role in the pathogenesis of PCOS [Franks et al. 2006; Xita and Tsatsoulis, 2006]. Therefore, hyperandrogenemia might indirectly promote insulin resistance in PCOS, by inducing abdominal adiposity and decrease in the insulin sensitizer adipokine.
The interactions between adiponectin and gonadal function and development in mice have been reported recently [Combs et al. 2003]. In this study, significant correlation was found between serum adiponectin levels with serum LH levels, LH:FSH ratio and serum testosterone levels, the hormone mainly responsible for PCOS-associated clinical hyperandrogenism. Adiponectin levels were found to correlate significantly with gonadotropin, testosterone, SHBG, insulin resistance and BMI parameters. This finding might indicate the involvement of adiponectin in the dysregulated metabolic state of PCOS.
Therefore, a multiple linear regression analysis was performed in order to assess independent relationships. The results found that adiponectin levels correlated with the nutritional status of obesity (BMI), testosterone levels (one of the PCOS criteria), and HOMA-IR values as parameter of insulin resistance (Table 4). These findings appear to favor a direct link between adiponectin and obesity in PCOS-associated insulin resistance.
The results of our study were consistent with substantial evidence that explained and suggested a role of hypoadiponectinemia in the pathophysiology of the metabolic abnormalities of PCOS-associated resistance to insulin. Women with PCOS who have low adiponectin levels had a higher BMI and insulin resistance, lower SHBG levels, higher gonadotropins (LH level and LH:FSH ratio) and testosterone levels, than women with higher adiponectin levels.
Regarding serum resistin level, resistin has been described as a potential link between obesity and insulin resistance [Steppan et al. 2001]. Resistin might therefore be expected to play a role in PCOS, and serum levels in these patients might be expected to be elevated. However, our study found that serum resistin levels in PCOS did not significantly differ from those in the control group (women without PCOS and normal BMI). It should be noted that none of the 24 PCOS women studied displayed hyperresistinemia. Furthermore, serum resistin levels did not correlate with BMI and HOMA-IR as parameter of insulin resistance. These results may indicate that serum resistin levels did not affect insulin sensitivity in PCOS, and may have a local paracrine action in the regulation of insulin resistance in obesity and PCOS [Seow et al. 2004].
In addition, investigations reported that resistin and adiponectin can play a role in the inflammatory process, where resistin acts as a proinflammatory adipokine and adiponectin acts as an anti-inflammatory adipokine [Bokarewa et al. 2005; Vendrell et al. 2004]. Furthermore, the ratio of these adipokines might represent the adipokine inflammatory condition. Our study showed that the R:A ratio had a moderately negative correlation with changes of BMI (R = 0.39, p < 0.05); see Figure 6.
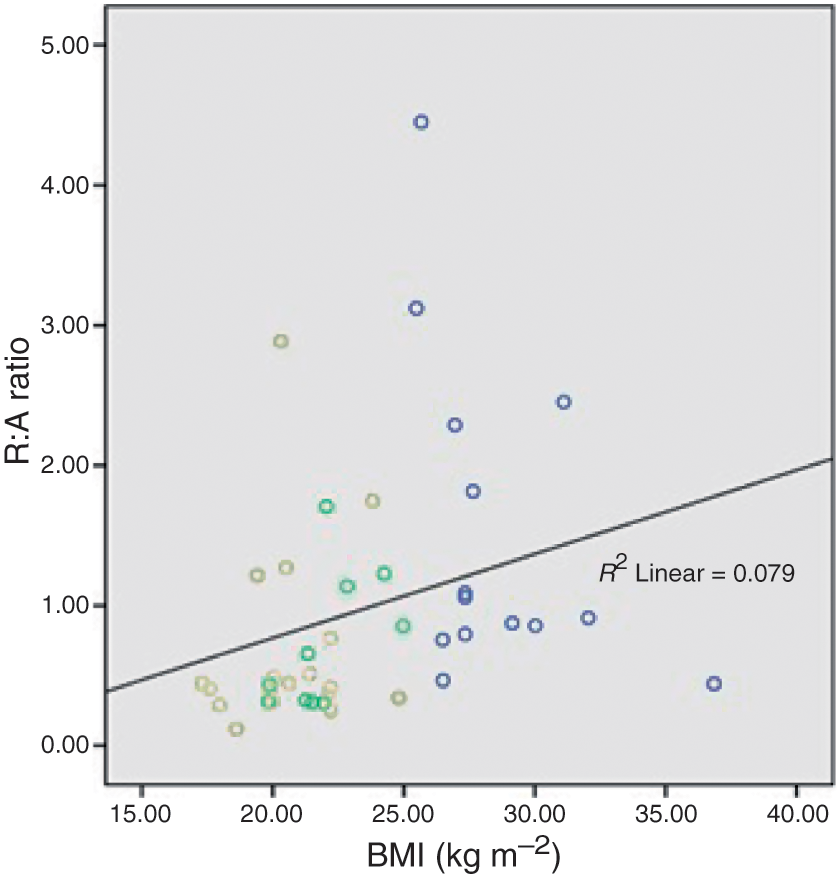
Correlation of body mass index (BMI) to resistin-to-adiponectin ratio (R:A ratio).
Increasingly, evidence indicates that adiposity contributes to a proinflammatory milieu, and the reduction in fat mass correlates with the decrease in the serum levels of many of these proinflammatory adipokines [Cottam et al. 2002; Das, 2001]. This study demonstrated that resistin does not seem to be actively involved in PCOS; it is probable that this hormone might act as local determining factor in this syndrome, suggesting a different regulatory mechanism. Furthermore, when resistin was expressed as a ratio with adiponectin, it showed that resistin plays a role in the inflammation process that correlated with obesity in women with PCOS.
In conclusion, the above findings suggest that adiponectin is involved in the pathogenesis of PCOS-associated insulin resistance, and that the ratio of resistin to adiponectin might play a role in the complicated metabolic abnormalities of the syndrome in obese women.
Footnotes
Acknowledgements
The authors thank Dr Nusrattuddin, OBGYN Department, Akademik Hospital, for patient recruitment. Mr Miswar Fattah, Mrs Wiwik Rositawati and Mr Mulyana, Research Laboratory, Prodia Clinical Laboratories, for excellent technical help.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare no conflicts of interest in preparing this article.