
Abstract
Background:
Oncocytic adrenocortical neoplasms (OANs) are extremely rare adrenal tumors whose diagnosis is challenging. This study aimed to identify risk factors for predicting poor prognosis in patients with OAN of uncertain malignant potential (OANUMP) and oncocytoma, OAN subtypes, and to evaluate the diagnostic utility of the current Lin-Weiss-Bisceglia (LWB) criteria.
Methods:
We retrospectively reviewed 14 patients diagnosed with OANUMP or oncocytoma after adrenalectomy from February 2002 to May 2022. Patients re-classified as oncocytic adrenocortical carcinoma by the LWB criteria were excluded. We compared the clinicopathological and radiological features between patients with and without recurrence.
Results:
Among the 14 patients, recurrence occurred in 3 (21%; 2 (67%) and 1 (33%) patients with OANUMP and oncocytoma, respectively). The proportion of patients with necrosis (66.7% vs 9.1%, p = 0.093), a Helsinki score >5 (66.7% vs 9.1%, p = 0.093), and malignancy by the reticulin algorithm (66.7% vs 9.1%, p = 0.093) were higher in the recurrence group than in the no-recurrence group but were not statistically significant. The percentages of patients with an indeterminate pathological resection margin (100% vs 63.6%, p = 0.192) tended to be higher in the recurrence group than in the no-recurrence group. Of the three patients with recurrence, two had tumor necrosis on the final pathology and were classified as malignant by the reticulin algorithm. One patient diagnosed as OANUMP by the LWB criteria had tumor necrosis and was classified as malignant by the reticulin algorithm and Helsinki scoring system.
Conclusion:
Necrosis was associated with the recurrence of disease in patients with OANUMP according to the LWB criteria. The absence of necrosis as a major criterion in the current LWB criteria highlights its potential limitation in accurately assessing disease aggressiveness in OANs.
Plain language summary
This study focuses on oncocytic adrenocortical neoplasms (OANs), a rare type of adrenal tumor, specifically analyzing two subtypes: OANUMP (oncocytic adrenocortical neoplasm of uncertain malignant potential) and oncocytoma. The objective was to assess the diagnostic utility of the LWB criteria, a tool used for diagnosis. A total of 14 patients were included in the study, and the factors found to be linked to poor prognosis in OANUMP and oncocytoma was necrosis. However, necrosis is currently not included as a major criterion for determining aggressiveness within the LWB criteria, including that it should be considered as such. Due to the limited number of patients in this study, further study with a larger sample size is recommended.
Introduction
Oncocytic adrenocortical neoplasms (OANs) are very unusual variants of adrenocortical tumors. OANs exclusively or predominantly comprise oncocytes, which are large polygonal cells characterized by granular eosinophilic cytoplasm owing to the accumulation of abnormal mitochondria. 1 Although occasionally found in the thyroid, kidney, and salivary glands, these tumors are rare in the adrenal cortex. Typically, OANs are considered nonfunctioning and benign and are larger than other adrenal tumor variants. 2 According to the Lin-Weiss-Bisceglia (LWB) criteria proposed in 2004, OANs can be classified as oncocytic adrenocortical carcinoma (OAC), OAN of uncertain malignant potential (OANUMP), and benign oncocytoma. Recent studies indicated the potential hormonal functionality of OANs, including cortisol and androgen excess.3–5
The standard therapy for OANs mainly relies on adrenalectomy because OANs typically present as a large adrenal mass. Laparoscopic adrenalectomy is more widely performed than conventional open adrenalectomy owing to its lower morbidity and shorter duration of hospitalization.6,7 This procedure is undertaken assuming the absence of capsular or vascular invasion and invasion of surrounding structures, as well as the possibility of achieving complete resection without disrupting the capsule during surgery. Moreover, adrenalectomy using robotic systems for OANs has been reported recently. 8
There are three diagnostic algorithms for OAN: the reticulin algorithm, the Helsinki scoring system, and the LWB criteria. The LWB criteria are divided into two categories, with major criteria including >5 mitoses per 50 high-power fields (HPFs), atypical mitosis, and venous invasion, and minor criteria including large size (>10 cm), necrosis, capsular invasion, and sinusoidal invasion. OANs with one or more major criteria are classified as OAC, those with one or more minor criteria are classified as OANUMP, and those with neither major nor minor criteria are classified as oncocytoma. 3 According to a recent systematic review focused on OANs, the overall survival rates of patients with OAC, OANUMP, and oncocytoma were 47%, 88%, and 100%, respectively, with a median follow-up duration of 24 months. The authors found that of 89 patients with OANs, 14 experienced recurrences, of whom one was diagnosed with oncocytoma. 9
Factors that influence the aggressiveness of OANUMP remain poorly explored. In a previous report, a patient initially diagnosed with oncocytoma of low-grade malignant potential post-adrenalectomy and expected to have a favorable postoperative prognosis was subsequently diagnosed with bone and liver metastasis. 10 Given the markedly low incidence of OANs, including OANUMP and oncocytoma, follow-up studies presenting the long-term prognosis of such neoplasms remain scarce.
This study aimed to analyze patients pathologically confirmed to have OANUMP and oncocytoma after adrenalectomy, determine the risk factors associated with a poor prognosis, and evaluate the diagnostic utility of the current LWB criteria for OANs.
Materials and methods
Patients and data collection
This retrospective study involved patients who underwent adrenalectomy for adrenal incidentaloma from February 2000 to May 2022 at a tertiary medical center. In total, 760 patients were diagnosed with nonfunctioning adrenal incidentaloma, of whom 143 underwent adrenalectomy during the study period. In the initial pathological reports, 26 patients were categorized as having OANs, among whom 6 were diagnosed with OAC, 13 were diagnosed with OANUMP, and 7 were diagnosed with oncocytoma. Six patients diagnosed with OAC were excluded from the current study. The pathology slides of 20 patients with OANUMP and oncocytoma were reviewed by 2 endocrine pathologists. In the revised pathology reports, six patients were re-classified as OAC, nine patients were classified as OANUMP, and five patients were classified as oncocytoma using the LWB criteria. Finally, 14 patients were included in the current study for further evaluation (Figure 1).

Flowchart of the study population.
Subsequently, the patients were divided into two groups according to their recurrence status. Recurrence was defined as the tumor reoccurring in the same place (local recurrence), nearby (regional recurrence), or in another location (distant recurrence) after the initial adrenalectomy. Follow-up assessments included computed tomography (CT), magnetic resonance imaging, and/or positron emission tomography imaging performed every 3–6 months postoperatively. The patients’ data included demographics such as age, sex, weight, height, and body mass index (BMI), preoperative CT scan features (e.g., tumor size, Hounsfield unit (HU), and washout), operative factors (e.g., operation type and resection margin status), and postoperative pathological features (e.g., tumor size, resection margin status, histochemical features, and immunohistochemical features). This retrospective study was approved by the Institutional Review Board of our institution. The need for informed consent from patients was waived owing to the retrospective nature of the study. In addition, this study was registered at the Research Registry in accordance with the World Medical Association’s Declaration of Helsinki, 2013. The work has been reported in line with the STROCSS criteria. 11
Preoperative CT scan findings
Contrast-enhanced adrenal or abdominal CT scans were performed, and washout of intravenous contrast medium was calculated at 60–90 s (portal venous phase) and 10–15 min (delayed enhancement phase) after contrast administration. To calculate the washout of intravenous contrast medium for the tumor, HU was measured during the precontrast, portal venous, and delayed phases. Absolute washout was calculated as the difference between the attenuation value in HU on an early enhanced CT image and HU on a delayed CT image. This difference was divided by the HU difference between the early enhanced and unenhanced CT images, and the result was multiplied by 100%. Relative washout was calculated by subtracting the HU on a delayed CT image from that on an early enhanced CT image. The resulting value was divided by the HU on an enhanced CT image and then multiplied by 100%. 12 The adrenal tumor size was measured by identifying the longest diameter of the tumor on the image displaying the largest lesion area in the cross-sectional view of the CT scan. Malignant features on CT scans were defined as tumor size ⩾4 cm, precontrast HU >10, absolute washout <60%, and relative washout <40%. Benign features on CT scans were defined as tumor size <4 cm, precontrast HU ⩽10, absolute washout ⩾60%, and relative washout ⩾40%. 13
Surgical techniques and intraoperative findings
Among the 14 patients, 8, 2, 3, and 1 underwent laparoscopic and robotic retroperitoneal posterior adrenalectomy, laparoscopic transperitoneal adrenalectomy, and conventional open adrenalectomy, respectively. During the surgical procedure, the status of the gross resection margin was assessed by examining the edges or borders of the excised tissue. The gross resection margin was established using the intraoperatively identified margin through instrumental inspection via telescope view or palpation of the operative field during open adrenalectomy. In addition to negative and positive margins, an unknown gross margin was recorded when there was no record of margin safety in the clinical data. For the pathological resection margin, an indeterminate margin was recorded when the negativity or positivity of the margin could not be confirmed, which was the case for intraoperatively fragmented specimens in specimen retrieval bags.
Samples and postoperative pathological evaluation
Paraffin-embedded blocks from 20 patients (13 with OANUMP and 7 with oncocytoma) based on the initial pathology reports were evaluated. In all cases examined, 4 µm-thick tissue sections were obtained from representative paraffin-embedded samples. All adrenal tumors were reviewed according to the LWB criteria and classified into three subtypes. The mitotic grade was determined by counting mitotic figures in 50 HPFs or 10 mm2 from areas with high mitotic densities in all tumor samples. Figure 2 presents a representative pathology image of OANs.

Oncocytic adrenocortical neoplasm. Diffuse proliferation of large polygonal cells with abundant eosinophilic cytoplasm and occasionally enlarged atypical nuclei detected by hematoxylin-eosin staining.
Histochemistry and immunohistochemistry
Representative markers related to the aggressiveness of adrenocortical neoplasm were selected for staining based on previous studies. 14 Hematoxylin-eosin (HE) staining was performed to confirm the diagnosis of OAN. In addition, staining was performed with monoclonal antibodies against Ki-67 (mouse clone MIB-1; Dako, Carpinteria, CA, USA) at 1:200 dilution, p53 (mouse clone DO-7; Dako) at 1:1000 dilution, β-catenin (mouse clone 14; Cell Marque, Rocklin, California, USA) at 1:200 dilution, and phospho-histone H3 (PHH3; rabbit clone POLY; Cell Marque) at 1:200 dilution.
Immunohistochemical staining was performed using an automated stainer (BenchMark XT automatic immunostaining device; Ventana Medical Systems, Tucson, Arizona, USA), in accordance with the manufacturer’s recommendations. Sections were placed on silanized charged slides, dried, and then incubated. Cell Conditioning 1 buffer and an autoimmunostrainer were utilized for epitope retrieval and antigen-antibody reactions, respectively. Thereafter, slides were counterstained and prepared for microscopic analysis.
Expression of p53 was evaluated based on overall positive nuclear or cytoplasmic staining and was classified into four categories, namely, 0, 1, 2, and 3, which corresponded to <5%, 5%–33%, 33%–66%, and >66% positivity, respectively. Expression of Ki-67 was determined by manually calculating the percentage of 1000–2000 tumor cells in the hotspot area that exhibited positive nuclear staining. The antibody expression ratios were compared and analyzed categorically, indicating positive expression or loss of antibody expression. Regarding β-catenin expression, specimens with only membranous staining were deemed negative, whereas those with cytoplasmic or nuclear staining were classified as positive. Mitotic figures were counted in 50 successive HPFs on HE-stained slides. Atypical mitoses were evaluated in HE-stained slides or slides stained for PHH3. In these stained sections, mitotic figures and atypical mitoses were identified based on positive staining and specific morphological characteristics.
The reticulin framework was examined using Gomori’s silver impregnation method. An altered reticulin network was defined as reticulin fibrils with variable, irregular thickness, and a frayed appearance surrounding single or small groups of cells (qualitative alteration) and loss of the reticulin framework (quantitative alteration). A normal reticulin network was defined as intact when reticulin fibrils of the same thickness completely surrounded adrenal cortical cells in nests and cords. 15 The present study primarily evaluated the loss of the reticulin framework.
Diagnostic algorithm and scoring system of OANs
In addition to LWB criteria-based classification of OAC, OANUMP, and oncocytoma, the aggressiveness of OANs was assessed using the reticulin algorithm and Helsinki scoring system. In the reticulin algorithm, malignancy is defined as an altered reticulin framework associated with one of the following three parameters: necrosis, high mitotic rate, and vascular invasion.15–17 The Helsinki score was calculated as follows: 3 × mitotic rate (>5 mitoses/50 HPFs) + 5 × presence of necrosis + proliferation index in the most proliferative area of the tumor. The aggressiveness of the neoplasm was classified as follows based on previous studies: Helsinki score 0–8.5, 8.5–17, and >17.17,18 The Helsinki score range of 0–8.5 was subdivided into 0–5 and 5–8.5.
Statistical analysis
Statistical analyses were performed using SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were reported as median (minimum−maximum) and compared using the Mann–Whitney U test. Categorical variables were reported as numbers (percentages) and were examined using Fisher’s exact test and the χ2 test. p Values <0.05 were considered statistically significant.
Results
Changes in diagnosis after retrospective pathological review
Figure 3 presents a flowchart depicting the changes in diagnosis after pathological review. Of 13 patients initially diagnosed with OANUMP, four suffered recurrence and nine remained recurrence-free. Of seven patients initially diagnosed with oncocytomas, one suffered recurrence and six remained recurrence-free. After pathological review, two of the four patients with recurrent OANUMP and three of the nine patients with nonrecurrent OANUMP were reclassified as OAC. Following pathological review, the initial diagnosis was retained in the one patient with recurrent oncocytoma, while among the six patients with nonrecurrent oncocytoma, one was re-classified as OAC and one was re-classified as OANUMP. The median follow-up duration was 30.8 months (range: 0.6–64.6 months). Among the 14 patients, 2 (14.2%) had a follow-up duration of less than 1 year.

Flowchart depicting the changes in diagnosis after pathological review.
Baseline clinical characteristics
Table 1 summarizes the clinical characteristics of the 14 patients with OANUMP or oncocytoma according to the LWB criteria based on their recurrence status. Age, sex, height, weight, BMI, sites of tumors, diagnosis, and types of operation did not significantly differ between the recurrence and no-recurrence groups. The tumor gross resection margins, which were confirmed during surgery, were clear in all patients.
Clinical features of patients with OANUMP and oncocytoma diagnosed according to the LWB criteria based on their recurrence status.
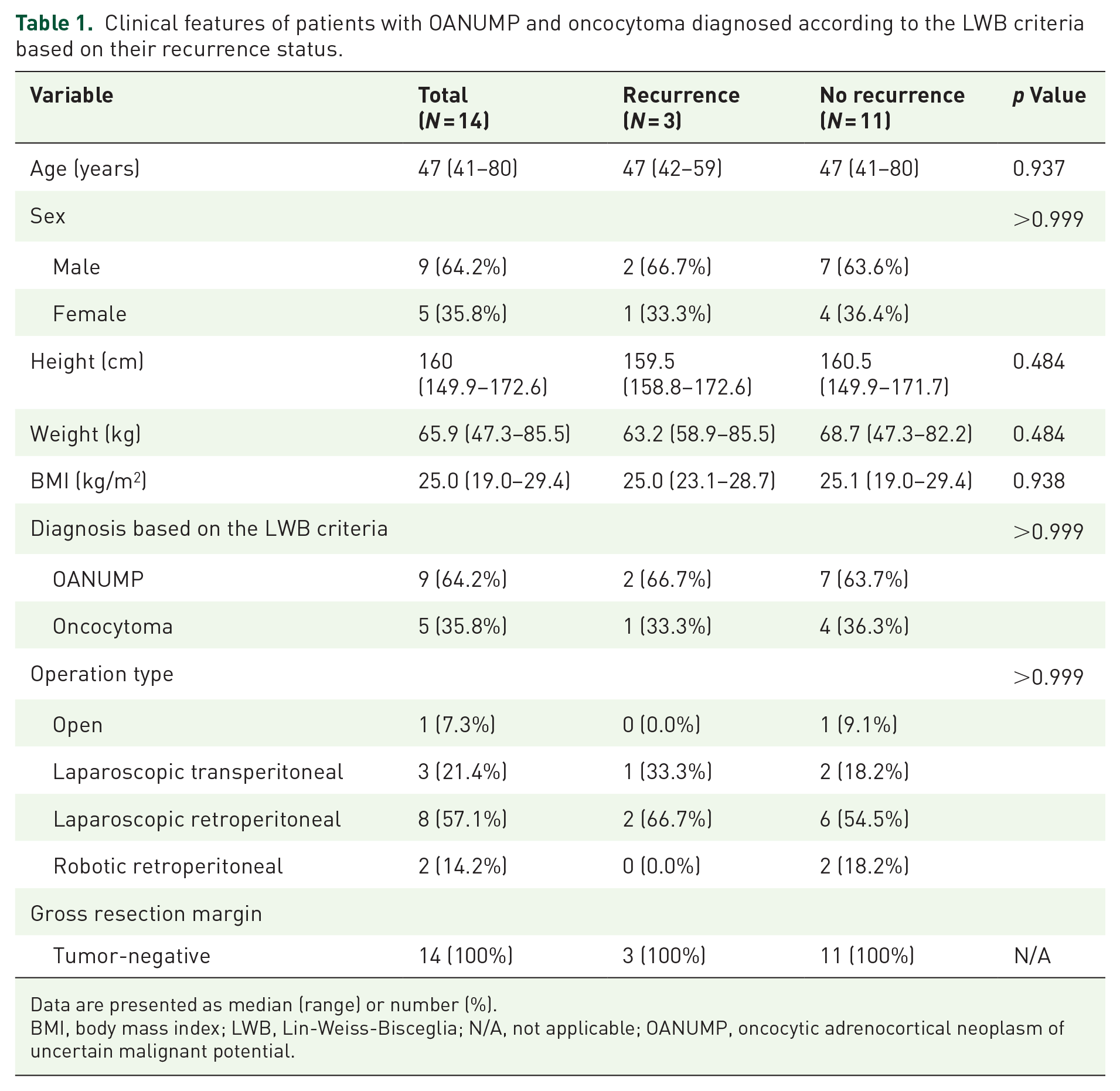
Data are presented as median (range) or number (%).
BMI, body mass index; LWB, Lin-Weiss-Bisceglia; N/A, not applicable; OANUMP, oncocytic adrenocortical neoplasm of uncertain malignant potential.
Preoperative CT scan features
Table 2 summarizes the preoperative CT scan features of the 14 patients with OANUMP and oncocytoma diagnosed according to the LWB criteria based on their recurrence status. The median tumor size was larger, albeit insignificantly, in the recurrence group than in the no-recurrence group (6.7 vs 5.5 cm, p = 0.102). The median precontrast HU values were above 10 in both groups. In contrast to the group without recurrence, the median values of absolute washout and relative washout in the recurrence group were both below 60 and 40, respectively, without statistical significance. The percentages of patients with all malignant features on CT scans, including tumor size ⩾4 cm, precontrast HU >10, absolute washout <60%, and relative washout <40%, was higher, albeit insignificantly, in the recurrence group than in the no-recurrence group (66.7% vs 22.2%, p = 0.236).
Preoperative CT features of patients with OANUMP and oncocytoma diagnosed according to the LWB criteria based on their recurrence status.

Data are presented as median (range) or number (%).
Malignant features on CT scans were defined as tumor size ⩾4 cm, precontrast HU >10, absolute washout <60%, and relative washout <40%.
CT, computed tomography; HU, Hounsfield unit; LWB, Lin-Weiss-Bisceglia; OANUMP, oncocytic adrenocortical neoplasm of uncertain malignant potential.
Postoperative pathological features
Table 3 summarizes the pathological features of patients with OANUMP and oncocytoma diagnosed according to the LWB criteria based on their recurrence status. All patients lacked major LWB criteria including a high mitotic rate, atypical mitosis using PHH3 as a mitosis marker, and venous invasion. Among minor LWB criteria, the percentage of patients with pathological necrosis was higher in the recurrence group than in the no-recurrence group (66.7% vs 9.1%, p = 0.093), indicating approximate statistical significance. The percentages of patients with capsular invasion and sinusoidal invasion were higher and median tumor size was larger, albeit insignificantly, in the recurrence group than in the no-recurrence group (66.7% vs 36.4%, p = 0.538; 66.7% vs 36.4%, p = 0.538; and 7.3 vs 4.8 cm, p = 0.368, respectively). The score of minor LWB criteria did not significantly differ between the two groups (p = 0.368).
Pathological features of patients with OANUMP and oncocytoma diagnosed according to the LWB criteria based on their recurrence status.

Data are presented as median (range) or number (%).
The score was calculated by summing minor LWB criteria (large size (>10 cm), necrosis, capsular invasion, and sinusoidal invasion).
The Helsinki score integrated the Ki67 proliferation index with scores assigned for an increased mitotic rate (score of 3 for >5 mitoses/50 HPFs) and tumor necrosis (score of 5).
Malignancy was diagnosed when an altered reticulin framework was seen in association with one of the following parameters: mitotic rate >5 mitoses/50 HPFs, tumor necrosis, and vascular invasion.
HPF, high-power fields; LWB criteria, Lin-Weiss-Bisceglia criteria; N/A, not applicable; OANUMP, oncocytic adrenocortical neoplasm of uncertain malignant potential; PHH3, phospho-histone H3.
The Ki-67 proliferation index did not significantly differ between the two groups (1.2% vs 1.6%, p = 0.738). The Helsinki score was higher, albeit insignificantly, in the recurrence group than in the no-recurrence group (5.9 vs 1.8, p = 0.240). The percentage of patients with a Helsinki score >5 was higher in the recurrence group than in the no-recurrence group (66.7% vs 9.1%, p = 0.093), indicating approximate statistical significance.
The percentage of patients with an altered reticulin framework did not significantly differ between the two groups (66.7% vs 45.5%, p > 0.999). The percentage of patients with malignancy by the reticulin algorithm tended to be higher in the recurrence group than in the no-recurrence group (66.7% vs 9.1%, p = 0.093). The percentage of patients with soft tissue extension did not significantly differ between the two groups (33.3% vs 9.1%, p = 0.396).
The percentage of patients with an indeterminate resection margin tended to be higher in the recurrence group than in the no-recurrence group (100.0% vs 63.6%, p = 0.192). The percentage of patients with nuclear β-catenin expression did not significantly differ between the two groups (33.3% vs 45.5%, p > 0.999). Regarding p53 expression, all patients in both groups were classified as category 1 (5%–33%).
The pathological features of each patient with OANUMP and oncocytoma diagnosed according to the LWB criteria are shown in Table 4. Among the three patients with recurrence, two demonstrated necrosis on the final pathology and were classified as malignant according to the reticulin algorithm (Patient No. 1, Patient No. 3). Patient No. 13, diagnosed with oncocytoma based on the LWB criteria, was not classified as malignant by either the reticulin algorithm or the Helsinki score, yet experienced recurrence. In contrast, Patient No. 4, diagnosed as OANUMP by the LWB criteria, presented with tumor necrosis on the final pathology, was classified as malignant by the reticulin algorithm, and had a Helsinki score of 10.9 (>8.5), indicating malignancy.
Pathological features of each patient with OANUMP and oncocytoma diagnosed according to the LWB criteria.
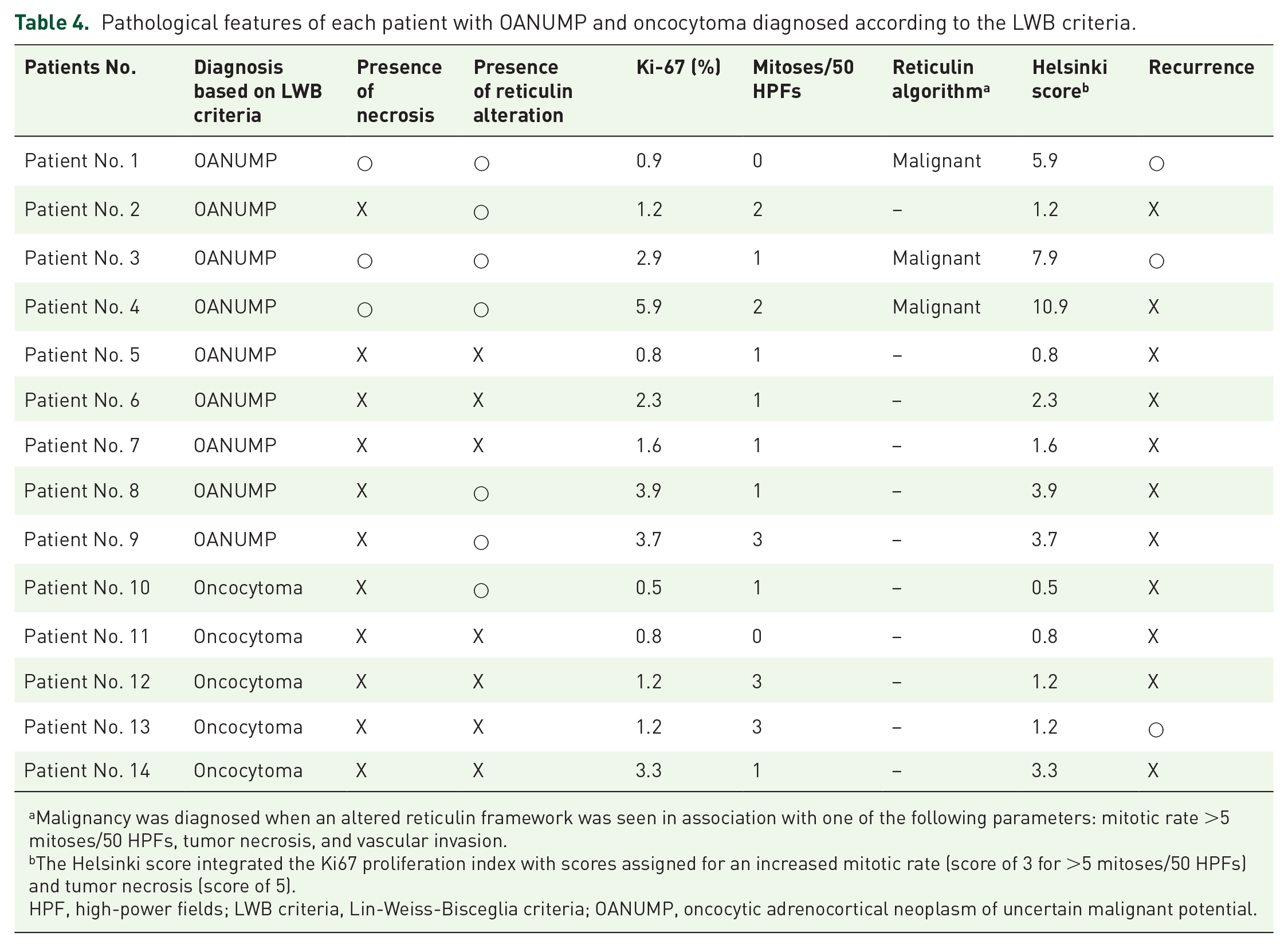
Malignancy was diagnosed when an altered reticulin framework was seen in association with one of the following parameters: mitotic rate >5 mitoses/50 HPFs, tumor necrosis, and vascular invasion.
The Helsinki score integrated the Ki67 proliferation index with scores assigned for an increased mitotic rate (score of 3 for >5 mitoses/50 HPFs) and tumor necrosis (score of 5).
HPF, high-power fields; LWB criteria, Lin-Weiss-Bisceglia criteria; OANUMP, oncocytic adrenocortical neoplasm of uncertain malignant potential.
Table 5 summarizes the detailed recurrence, treatment, and radiological features of three recurred patients. Figure 4 presents a summary comparing the histopathological and radiological features of patients in the recurrence and no-recurrence groups.
Characteristics of patients who suffered recurrence after adrenalectomy.
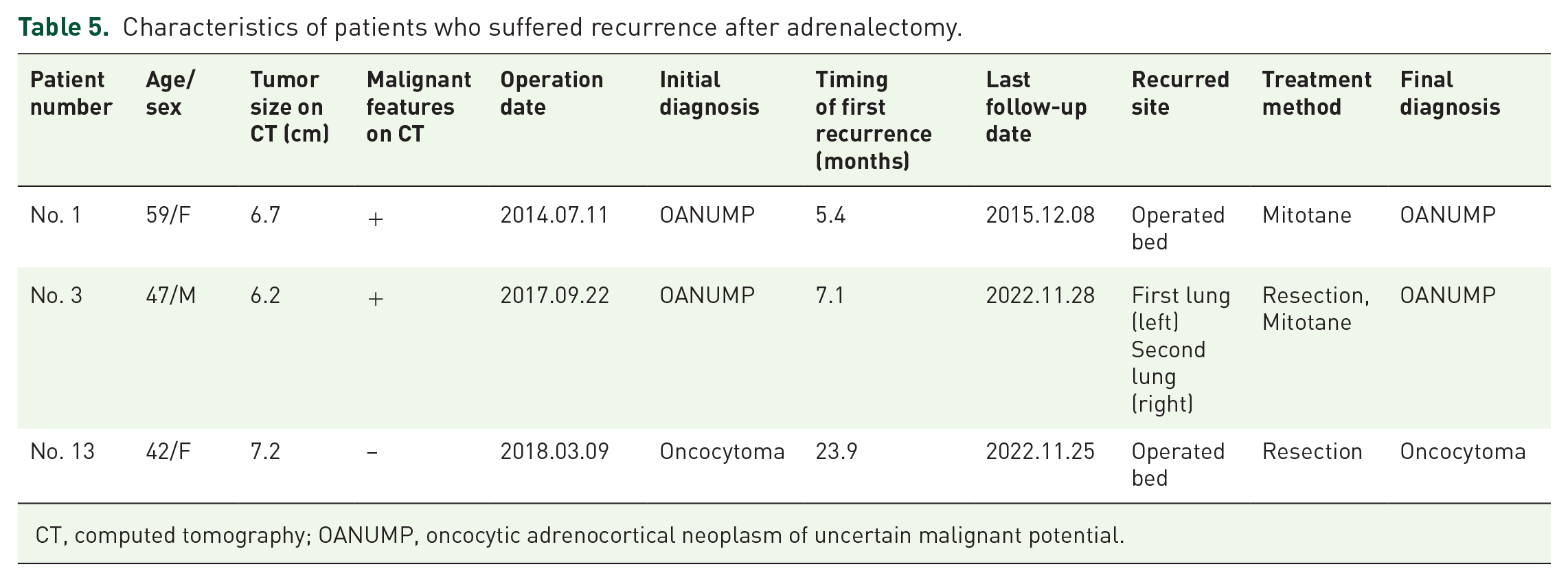
CT, computed tomography; OANUMP, oncocytic adrenocortical neoplasm of uncertain malignant potential.

Comparison of histopathologic features between the recurrence and no-recurrence groups in patients with OANUMP or oncocytoma based on the Lin-Weiss-Bisceglia criteria.
Discussion
In the present study, we evaluated the risk factors associated with poor prognosis in patients diagnosed with OANUMP and oncocytoma after adrenalectomy. A higher percentage of patients with recurrence exhibited necrosis. In addition, a higher percentage of patients with recurrence had a Helsinki score >5. Likewise, the percentage of patients with malignancy according to the reticulin algorithm was higher in the recurrence group than in the no-recurrence group. However, none of these factors showed a statistically significant difference. Of the three patients with recurrence, two had necrosis on the final pathology and were classified as malignant by the reticulin algorithm. All patients with recurrence exhibited indeterminate margins. Patients with recurrent OANUMP or oncocytoma had absolute and relative washout values less than 60% and 40% on CT scans, respectively; these values were lower than those of patients without recurrence. Furthermore, the percentage of patients with a combination of three factors (tumor size ⩾4 cm, precontrast HU >10, and absolute washout <60% with relative washout <40%) indicative of malignant features was higher in the recurrence group than in the no-recurrence group.
Juliano et al. 10 reported a change in the diagnosis of the OAN subtype in one patient. A patient initially diagnosed with oncocytoma of low-grade malignant potential after adrenalectomy exhibited a disturbing malignant potential upon secondary pathological review. Subsequently, the patient developed liver and bone metastasis. In addition, Huang et al. 19 reported a patient who was initially diagnosed with OANUMP, which was later confirmed as OAC with concomitant scalp and lung metastases. In the present study, among the 20 patients initially diagnosed with OANUMP or oncocytoma using the LWB criteria, the diagnosis of seven (35%) was altered following pathological review, and two of these patients experienced recurrences. These findings clearly indicate the challenges associated with the pathological diagnosis of OAN subtypes. Moreover, our results imply that the currently used LWB criteria have limitations in terms of classifying OAN subtypes.
According to the LWB criteria, evidence of malignant OANs includes atypical mitosis, >5 mitoses/50 HPFs, and venous invasion. In the present study, following pathological review, all six patients who were re-classified as OAC and subsequently excluded exhibited atypical mitosis. Among them, recurrence was observed in two cases. However, patients diagnosed with OANUMP according to the LWB criteria without atypical mitosis also exhibited malignant features, including recurrence. Accordingly, the discriminatory power of the LWB criteria to predict malignancy may need to be reassessed in future investigations.
In previous reports, radiological features of OANs have been scarcely described, with the majority of patients exhibiting tumors measuring ⩾4 cm on CT scans.9,20,21 In 2021, a treatment algorithm and imaging features were published for patients with adrenal incidentalomas. On CT scans, adrenal tumors ⩾4 cm in size, precontrast HU >10, and contrast washout <40%–60% were described as displaying a suspicious malignant appearance. 13 Khan et al. 22 reported that malignant OANs, similar to adrenocortical carcinoma (ACC), display an absolute washout of <60% and a relative washout of <40%. In the present study, a higher percentage of patients with recurrence than without recurrence had all three of these features without statistical significance, and all patients, regardless of recurrence status, exhibited precontrast HU >10. Accordingly, adrenal tumors ⩾4 cm in size, precontrast HU >10, and contrast washout <40%–60% alone may not effectively discriminate the aggressiveness of OANUMP or oncocytoma; however, the combination of these three features on CT scans may suggest a potential risk factor for recurrence among patients diagnosed with OANUMP or oncocytoma.
Microscopic tumor necrosis is associated with the aggressiveness of adrenocortical neoplasms.23,24 A study by Stojadinovic et al. compared 67 patients with conventional ACC and 37 patients with adrenocortical adenoma (ACA). All patients with microscopic tumor necrosis were diagnosed with ACC. Our findings are consistent with those of Stojadinovic et al. The percentage of patients with microscopic tumor necrosis was significantly higher among those who experienced recurrence than among those who did not. Duregon et al. 18 reported that a Helsinki score >8.5 is a diagnostic factor for ACC and that a Helsinki score of >17 may help to predict metastasis in cases of adrenal cortical neoplasms. In addition, they reported a reticulin algorithm incorporating an altered reticulin framework, which is indicative of malignancy of adrenal cortical neoplasms. 25 In the present study, among the three patients with recurrence, two were diagnosed with ONAUMP and one with oncocytoma based on the current LWB criteria. Both OANUMP patients exhibited necrosis and were classified as malignant according to the reticulin algorithm and had a Helsinki score <8.5. One patient, who had no recurrence and was diagnosed as OANUMP based on the LWB criteria, demonstrated necrosis on final pathology and was classified as malignant according to the reticulin algorithm, with a Helsinki score of 10.9 also indicating malignancy. As with other cases, the classification as malignant by the reticulin algorithm was due to the presence of necrosis. These findings suggest that the presence of tumor necrosis is strongly associated with the aggressiveness of OANs. However, since the presence of necrosis is not included as a major criterion in the current LWB criteria, this highlights a potential limitation of the LWB criteria in accurately discriminating the aggressiveness of the disease in OANs. Moreover, the observation that all patients with recurrence had a Helsinki score <8.5 indicates that the threshold, regarded as a criterion for ACC aggressiveness, may warrant reassessment in OANs.
Involvement of the microscopic resection margin is associated with aggressiveness in cases of adrenocortical neoplasms.23,24 A study by Stojadinovic et al. found that 60.3% of patients with ACC had positive or unknown microscopic resection margins, while all patients with ACA had negative microscopic resection margins. Regarding the status of the pathological margin, an indeterminate margin was observed in all patients with recurrence but only in 63% of patients without recurrence. In contrast with the results of the aforementioned study, no patient showed positive involvement of the resection margin. This may be because specimen fragmentation occurred during intraoperative retrieval in all patients with an indeterminate margin. Accordingly, retrieval of the tumor as a whole during surgery is crucial to accurately assess the pathological margin. Recurrence in the patient with oncocytoma may also be associated with the indeterminate status of the pathological resection margin.
Zhang et al. 26 reported that the Ki-67 labeling index with a cutoff value of 20% and 3% was an independent prognostic factor for overall and recurrence-free survival, respectively, in 66 patients with ACC. Conversely, in the present study, the highest Ki-67 index was 5.9%, and the mean Ki-67 index was unexpectedly higher, albeit insignificantly, in patients without recurrence. In their analysis of 24 patients with ACC, Angelousi et al. 14 reported that p53 expression was ⩾50% in 66.7% of patients with recurrence but was 21%–50% in 75% of patients without recurrence. In the present study, p53 expression ranged from 5% to 33% in all patients. These findings suggest that the relationship between the Ki-67 labeling index and the aggressiveness of OANUMP or oncocytoma, as well as the relationship between p53 expression and aggressiveness, may be limited.
This study has several limitations. First, it was a retrospective single-center study and there may be selection bias in the study population. Second, the sample size was too small to demonstrate statistically significant trends. Consequently, we identified several factors associated with recurrence through univariate analysis but were unable to identify an independent factor associated with poor prognosis. Third, during adrenalectomy, all fragmented specimens were evaluated as having indeterminate resection margins. Consequently, accurate microscopic assessment of the resection margins of these specimens was unavailable. Finally, the short follow-up duration in two patients may have limited the ability to adequately observe and detect disease recurrence. Nevertheless, to the best of our knowledge, this is the first report to identify risk factors associated with the aggressiveness of OANUMP and oncocytoma, while also highlighting a potential limitation of the LWB criteria.
In conclusion, in patients with OANUMP according to the LWB criteria, the presence of necrosis of the minor criteria is associated with the aggressiveness of the disease. Since the presence of necrosis is not included as a major criterion in the current LWB criteria, this highlights a potential limitation of the LWB criteria alone in accurately discriminating the aggressiveness of the disease. However, investigations of larger populations are needed to conclusively determine the discriminatory power of the LWB criteria in assessing disease aggressiveness in OANs.