
Abstract
Diabetes mellitus (DM) is a chronic, progressive, and multifaceted illness resulting in significant physical and psychological detriment to patients. As of 2019, 463 million people are estimated to be living with DM worldwide, out of which 90% have type-2 diabetes mellitus (T2DM). Over the years, significant progress has been made in identifying the risk factors for developing T2DM, understanding its pathophysiology and uncovering various metabolic pathways implicated in the disease process. This has culminated in the implementation of robust prevention programmes and the development of effective pharmacological agents, which have had a favourable impact on the management of T2DM in recent times. Despite these advances, the incidence and prevalence of T2DM continue to rise. Continuing research in improving efficacy, potency, delivery and reducing the adverse effect profile of currently available formulations is required to keep pace with this growing health challenge. Moreover, new metabolic pathways need to be targeted to produce novel pharmacotherapy to restore glucose homeostasis and address metabolic sequelae in patients with T2DM. We searched PubMed, MEDLINE, and Google Scholar databases for recently included agents and novel medication under development for treatment of T2DM. We discuss the pathophysiology of T2DM and review how the emerging anti-diabetic agents target the metabolic pathways involved. We also look at some of the limiting factors to developing new medication and the introduction of unique methods, including facilitating drug delivery to bypass some of these obstacles. However, despite the advances in the therapeutic options for the treatment of T2DM in recent years, the industry still lacks a curative agent.
Introduction
Diabetes mellitus (DM) is a global epidemic posing a significant health threat to people around the world. According to the International Diabetes Federation (IDF) estimates in 2019, 463 million people aged 20–79 years suffered from DM worldwide, which is projected to rise to a staggering 700 million in the next 25 years 1 (Figure 1). DM is the fastest growing health challenge of the 21st century, and its scale is such that 1 in 11 adults (20–79 years) have DM, bleeding $760 billion in funds, which is 10% of the worldwide health expenditure. 2 DM confers a risk of early mortality, and in 2019 the IDF projected that 4.2 million adults would die as a result of DM and related complications, which, when put into perspective, is equivalent to one death every 8 s. 2 T2DM accounts for approximately 90% of all DM cases, and the global exponential growth of this epidemic is mainly attributable to a sedentary lifestyle, obesity, an ageing populace, urbanization, and economic development.3,4

Management of T2DM requires a patient-centred approach in bringing about lifestyle changes and optimizing glycaemic control using the available pharmacological options to preserve the quality of life and minimize complications.5,6 The Kumamoto 7 and UK Prospective Diabetes Study (UKPDS)8,9 confirmed that intensive glycaemic control in patients with newly diagnosed T2DM significantly decreased rates of microvascular complications and, therefore, early and adequate treatment is of paramount importance. T2DM is a progressive condition, and to prevent long-term complications, improving and sustaining glycaemic control is vital. Timely treatment escalation can help achieve this; however, this is often delayed, and people remain with suboptimal glycaemic control for several years. 10 Comorbid state, insulin resistance (IR), and beta-cell dysfunction render many available treatments, either inadequate or contra-indicated. An intricate scenario is further complicated when treatment choices have to be informed to avoid hypoglycaemia and weight gain. 11
Due to the introduction of new oral and injectable pharmacological agents, which are potent and well tolerated, clinicians nowadays have more options for treating T2DM. However, based on the commonly encountered constraints mentioned above, there is a requirement for developing new agents which are effective individually and can be safely co-prescribed with the currently available array of treatment options. In addition to this, the medical community is longing for preparations that positively impact complications arising from T2DM and have little or no limitations to their use in patients with significant multiorgan comorbid states.
In this article, we discuss the pathophysiology of hyperglycaemia in T2DM, followed by recently included therapeutic agents and novel medication under development for the treatment of T2DM.
Methodology
We systematically searched PubMed, MEDLINE, and Google Scholar for original articles, review articles, systematic reviews, randomized control trials (RCTs), and meta-analysis published in English from 01 January 2011 to 05 March 2021. Relevant and important articles published before 2011 were also included. We developed a search string of medical subject headings (MeSH) including the terms ‘diabetes’ OR ‘non-insulin-dependent diabetes mellitus’ OR ‘hyperglycaemia’ OR ‘T2DM’, ‘insulin resistance’, ‘novel agents’ OR ‘future medications’ AND ‘updates’, ‘medical treatment’ OR ‘pharmacological treatment’ OR ‘therapy’, ‘novel delivery methods’ OR ‘administration’, ‘genome-wide association and type 2 diabetes’, ‘insulin pump systems’ AND ‘closed-loop pump systems’.
Pathophysiology of hyperglycaemia in T2DM
In contrast to type-1 diabetes mellitus (T1DM), where the driving force behind hyperglycaemia is autoimmune destruction of β-cells, T2DM results from β-cell dysfunction and IR. There is high insulin demand from the peripheral tissues due to IR resulting in β-cell expansion and hyperinsulinemia. 12 As a result of this compensatory response from the β-cells, in the presence of a hyperglycaemic milieu, there is a steady loss of β-cell mass thought to occur from accentuated apoptosis.13–15 The development of T2DM is a continuum from a state of impaired glucose tolerance (IGT), where patients exhibit a very high level of IR and have lost an estimated 80% of their β-cell function to T2DM. To explain the pathophysiologic defects in T2DM, eight key collaborators have been described which include pancreatic β-cells (decreased insulin secretion), pancreatic α-cells (increased glucagon secretion), liver (increased hepatic glucose output), muscle (decreased glucose uptake), adipose tissue (increased lipolysis), kidney (increased glucose re-absorption), gut (decreased incretin effect), and the brain (impaired appetite regulation) which were collectively called the ominous octet. 16 In DM, the complex system required to maintain euglycemia independent of glucose load and clearance fails 17 (Figure 2) and the fascinating interplay between IR, impaired insulin secretion and loss of β-cell mass, have long been targeted with therapeutic agents to treat this condition.

A brief illustrative explanation of molecular mechanisms responsible for insulin resistance in T2DM followed by a discussion on organ-specific contributions. Insulin resistance in the muscles; defective insulin signalling, glucose transport, glucose phosphorylation, glycogen synthesis, pyruvate dehydrogenase complex activity, and mitochondrial oxidative activity.16,18,19 Events in the liver; insulin resistance/deficiency, hyperglucagonaemia, enhanced glucagon sensitivity, and increased substrate (fatty acids, lactate, glycerol, and amino acids) delivery, leads to increased gluconeogenesis, which is responsible for the increased basal rate of glucose production and fasting hyperglycaemia.20–22 Renal contribution; renal insulin resistance and augmented renal gluconeogenesis contribute to fasting hyperglycaemia. 23 Vascular endothelium; impaired vasodilation due to insulin resistance resulting in reduced insulin and glucose delivery. 24 Finally, post-prandial hyperglycaemia ensues due to increased hepatic glucose output, muscle insulin resistance, reduced non-insulin-mediated glucose uptake, and excessive renal glucose re-absorption.25,26
Combined peptide injectables
By increasing β-cell insulin secretion, delaying gastric emptying, and reducing glucagon secretion, glucagon-like peptide-1 (GLP-1) analogues successfully target and suppress post-prandial hyperglycaemia in T2DM.27,28 On the contrary, basal insulin therapy targets fasting hyperglycaemia and theoretically, when combined, their complimentary action should result in significant improvement in glycaemic control. This materialized with the introduction of IDegLira (50 U insulin degludec and 1.8 mg liraglutide) and iGlarLixi (100 U insulin glargine and 50 μg lixisenatide) in a titratable fixed-ratio combination. The FDA approved both combination injections for clinical use in 2016. Results from the DUAL (Dual Action of liraglutide and Insulin Degludec in T2DM) clinical development programme demonstrated the efficacy and safety of iDegLira in 1393 adults with T2DM, who had inadequate glycaemic control on liraglutide or basal insulin alone. Switching to iDegLira resulted in a mean reduction in HbA1c up to 1.94%. Lixilan-O (ClinicalTrials.gov NCT02058147) compared iGlarLixi with insulin glargine or lixisenatide alone for treatment of insulin-naive patients on metformin29,30 while lixiLan-L (ClinicalTrials.gov NCT02058160) compared iGlarLixi with insulin glargine alone in patients already using basal insulin with or without oral hypoglycaemic agents.30,31 As evidenced by several studies,29,31–33 both IDegLira and iGlarLixi achieved more significant HbA1c reductions without increasing the risk of hypoglycaemia in patients with T2DM, compared to individual insulin or GLP-1 analogues. In addition to the described benefits, there is a lower risk of hypoglycaemia, weight gain, and gastrointestinal side effects.34,35 All these attributes make these injections suited for the management of T2DM and can be utilized at the treatment intensification stage of the management algorithm.
GLP-1 and GIP dual-receptor agonists
GIP is an incretin hormone like the much talked about GLP-1. Together, they are responsible for enhancing glucose-dependant insulin secretion from the pancreatic β-cells termed the incretin effect.36,37 Under normal physiological circumstances, the incretin effect is mainly driven by GIP.38,39 Developed by Eli Lilly, Tirzepatide (TZP), LY3298176, is a GLP-1 receptor and GIP receptor (GLP-1R/GIPR) dual agonist, which has achieved superior HbA1c and weight reductions compared to injectable semaglutide as an add-on to metformin in adults with T2DM in the phase-3 SURPASS-2 clinical trial (ClinicalTrials.gov NCT03987919). In this 40-week, multi-centre, randomized, parallel, open-label trial, participants taking weekly TZP 15 mg (highest dose) achieved an HbA1c reduction of 2.46% and weight loss of 13.1% compared to weekly semaglutide 1 mg. An estimated 51% of patients who received the higher TZP dose achieved an HbA1c of <5.7% (non-diabetic range) compared to 20% in the semaglutide arm. 40 Previously in patients with T2DM, once weekly TZP at doses of 1, 5, 10, or 15 mg has been compared to once weekly dulaglutide 1.5 mg; in a double-blind phase-2 study. Patients were randomly assigned (1:1:1:1:1:1) to receive either once weekly subcutaneous (SC) TZP (1, 5, 10, or 15 mg), dulaglutide (1.5 mg), or a placebo for 26 weeks. The change in HbA1c with TZP at 26 weeks was −1.06% (1 mg), −1.73% (5 mg), −1.89% (10 mg), and −1.94% (15 mg) compared with −0.06% for placebo and −1.21%. Reassuringly, the change in HbA1c with TZP did not plateau. At 26 weeks, 33%–90% of patients treated with TZP achieved the HbA1c target <7% versus (vs) 52% with dulaglutide and 12% with placebo. At 26 weeks, changes in mean body weight ranged from −0.9 to −11.3 kg for TZP versus −0.4 kg for placebo versus −2.7 kg for dulaglutide. Gastrointestinal events including nausea, diarrhea, and vomiting were the most reported side effects, were dose dependent, mostly mild-moderate and self-limiting. There were no reports of severe hypoglycaemia. 41 Although the mechanism of its action is not fully understood, studies suggest that TZP binds to the GIPR with the same affinity as native GIP while its affinity with the GLP-1R is five times lower than the endogenous molecule. 42 As a result, TZP engages GIPR more than the GLP-1R, and the unique signalling properties at the GLP-1R may form the basis of its profound efficacy.43,44 GLP-1R/GIPR dual agonists (Table 1) have shown significantly better efficacy in terms of glycaemic control and weight loss compared to GLP-1R agonists with satisfactory tolerability and so will be a welcome addition to the therapeutic options in T2DM.
A list of recently developed GLP-1R/GIPR dual agonists. 45 .

GLP-1R, GLP-1 receptor; GIPR, GIP receptor.
Sodium-glucose co-transporter and dual SGLT1 and SGLT2 inhibitors
Sodium-glucose co-transporters (SGLTs) regulate sodium and glucose transport across cell membranes. Six SGLT isoforms have been identified in human beings; 46 however, only SGLT1 and SGLT2 inhibition has translated into pharmacotherapy in T2DM so far. SGLT1 is a high-affinity but low-capacity transporter, 47 which mediates the absorption of glucose in the small intestine and accounts for the re-absorption of approximately 3% of the filtered glucose from the S3 segment of the proximal convulated tubule (PCT) in the nephrons.48,49 In contrast, SGLT2 is a low-affinity but high-capacity transporter, 47 which is responsible for the bulk (>90%)48,49 of glucose re-absorption from the S1 and S2 segments of the PCT.50,51 Targeting the inhibition of SGLT2 could lead to glucosuria and improved glycemia.
In 2012, dapagliflozin was approved by the European Medicines Agency (EMA) for clinical use, marking the first approval of a drug from this class anywhere around the world. 52 The following year, canagliflozin was approved by the Food and Drug Administration (FDA) for clinical use in the United States, 53 and thereafter several agents have been approved and marketed around the world. These approvals came on the back of large-scale clinical trials, where, in addition to improving glycaemic control, SGLT2 inhibitors led to weight loss and demonstrated cardio-renal benefits. For instance, not only did empagliflozin reduce the 3-point major adverse cardiac events (cardiovascular death, non-fatal myocardial infarction, and stroke), it was shown to reduce cardiovascular death (by 38%), hospitalization with heart failure (by 35%), and all-cause mortality (by 32%) aswell.54–57 These remarkable results have led to a rapid uptake of this class in the management of T2DM.
Recent pharmacological research suggested that combined SGLT1 and SGLT2 inhibition resulted in significant post-prandial glucose reduction, the elevation of endogenous GLP-1, and urinary glucose excretion. First-in-class of dual SGLT1 and SGLT2 inhibitors, sotagliflozin has been developed. 58 It has 20-fold higher selectivity for SGLT2 than SGLT1, is as effective as dapagliflozin and canagliflozin in inhibiting SGLT2 but is greater than 10-fold more potent than them in inhibiting SGLT1.59–61 From phase-2 and -3 clinical trials, sotagliflozin has demonstrated improved glycaemic control, reduced post-prandial glucose, reduced insulin requirements, appetite suppression, and weight loss in patients with type-1 62 and type-2 diabetes.63,64
Encouraging results from phase 3, inTandem 1–3 trials 65 among others, 62 have led to its approval in the EU as an adjunct to insulin in patients with T1DM with a body mass index (BMI) ⩾ 27 kg/m2 who have failed to achieve adequate glycaemic control despite optimal insulin therapy. 66 A higher incidence of ketoacidosis with sotagliflozin (3%) compared to placebo (0.6%) was seen in the inTandem study which is of some concern,61,65 an effect also seen with dapagliflozin in the past. 67 Goldenberg and colleagues have developed the ‘STOP DKA Protocol’, a practical tool that may potentially help in reducing this risk in clinical pratice 68 in addition to appropriate patient selection and down titration of basal insulin. In the SOLOIST-WHF clinical trial (ClinicalTrials.gov NCT03521934), sotagliflozin therapy resulted in a significantly lower total number of deaths from cardiovascular causes, hospitalizations, and urgent visits for heart failure compared to placebo in patients with T2DM. 69 Moreover, in the SCORED clinical trial (ClinicalTrials.gov NCT03315143), treatment with sotagliflozin resulted in a similar effect in patients with T2DM and chronic kidney disease with or without albuminuria. 70 Another dual SGLT1 and SGLT2 inhibitor, licogliflozin has been shown to exert a favourable metabolic effect leading to weight loss, reduced PPG excursion, and elevation of total GLP-1 levels in patients with obesity and T2DM.71,72 Based on the overwhelmingly encouraging results from sotagliflozin, it seems that approval for use in T2DM is not far away. At the same time, other agents from this novel class can emerge as clinically beneficial entities for the treatment of T2DM in the years to come.
Peroxisome proliferator–activated receptor α (alpha)/γ (gamma)/δ (delta) pan-agonists
Peroxisome proliferator–activated receptors (PPARs) are ligand-activated transcription factors of nuclear hormone receptors. Their subtypes include PPAR-α (liver, muscle, and heart); PPAR-γ (adipose tissue and vascular endothelial cells), and PPAR-δ (widespread whole-body distribution) which play an integral part in energy metabolism, where PPAR- δ regulates energy expenditure while PPAR-γ mediates its storage.73–75 Thiazolidinediones (TZDs) are anti-diabetic agents in clinical use since 1997. 76 They are PPAR-γ agonists, which enhance insulin sensitivity by increasing adiponectin, GLUT4 expression and oppose the effect of tumour necrosis factor (TNF)-alpha in adipocytes. These actions result in reduced hepatic gluconeogenesis and increase insulin-dependent glucose uptake in muscle and fat. 77 Chiglitazar, a novel PPARα/γ/δ pan-agonist, has been investigated in phase-3 multi-center, randomized, double-blind, and placebo-controlled trials (ClinicalTrials.gov NCT02121717), 78 as well as sitagliptin, controlled (ClinicalTrials.gov NCT02173457) 79 trials in patients with T2DM with insufficient glycaemic control despite diet and exercise. Compared to placebo, at 24 weeks, both doses of chiglitazar were superior to placebo in HbA1c reduction and the effects were sustained for 52 weeks. The mean change in HbA1c from baseline was −0.45% ± 1.22% with placebo, −1.30% ± 1.07% with chiglitazar 32 mg, and −1.52% ± 1.19% with chiglitazar 48 mg. Although hypoglycaemia, weight gain, and oedema were relatively more common with chiglitazar, the overall adverse events were comparable across all groups with no major safety concerns. 80 MHY2013 and IVA337 are other examples of PPAR pan-agonists that have been shown to suppress inflammation and hepatic lipid accumulation and may emerge as useful candidates for treating non-alcoholic fatty liver disease (NAFLD) in the future.81,82
GLIMINS
A novel oral anti-diabetic drug, imeglimin is a tetrahydrotriazine compound that is the first member of the ‘glimins’ class of agents and has been investigated in many landmark clinical trials. 83 In patients with T2DM, imeglimin has shown sustained improvement in hyperglycaemia without disabling hypoglycaemia and was not associated with a concerning side-effect profile.84,85 Its unique mechanism of action (MOA) (Figure 3) not only increases glucose-dependant insulin secretion but also reduces IR.86,87 It acts by inhibiting the process of oxidative phosphorylation in the mitochondria of aerobic cells which in turn leads to favourable metabolic effects. 86 Imeglimin counteracts a variety of metabolic disruptions at play in T2DM. It accelerates the phosphorylation of Akt (protein kinase B) leading to enhanced insulin signalling 88 and has also been linked to the induction of insulin sensitivity in the β-cells. 89 In addition to this, imeglimin reduces hepatic gluconeogenesis,86,90 is protective against β-cell death, increases the β-cell mass and improves glucose-induced insulin secretion (GSIS) from islets of Langerhan cells in the pancreas.87,89,91 Interestingly, Lachaux et al. 92 reported a reduction in left ventricle (LV) end-diastolic pressure and increased LV tissue perfusion with imeglimin treatment in Zucker fa/fa rats. These findings suggest that imeglimin is potentially cardioprotective in addition to its anti-diabetic properties and thus once approved for commercial use, will be a useful inclusion to the arsenal against T2DM.

Potential mechanisms via which glucose homeostasis is improved by imeglimin therapy. 86
A systematic review and meta-analysis of the available evidence from Crabtree et al. 93 showed that imeglimin therapy, at a dose of 1500 mg twice a day, lead to a reduction in HbA1c (0.63%) and fasting plasma glucose (FPG) (0.52 mmol/L) in patients with T2DM when used alone or in combination with metformin or sitagliptin. These results are similar to those reported for other classes of glucose-lowering therapies inducted in clinical practice in recent times. Based on the available evidence, imeglimin use is not related to any significant adverse effects and is overall well tolerated. 94 Based on its potent anti-diabetic effect as monotherapy and as an adjunctive treatment, 93 the lack of major adverse effects and potential cardioprotection, imeglimin is poised to occupy a crucial role in the future of T2DM pharmacotherapy.
Therapies targeting the glucagon receptor
GLP-1R and glucagon receptor dual agonists
Around 90% of patients with T2DM are overweight, making it an important risk factor for its development. 95 GLP-1R agonists improve glycaemic control and reduce weight in patients with T2DM, making them an effective pharmacological agent. 96 Glucagon is a peptide hormone, produced by the α-cells of the islets of Langerhans. Acting via the glucagon receptor (GCGR), it increases glucose concentration in the bloodstream via gluconeogenesis and glycogenolysis, increases lipolysis, improves energy expenditure and can activate the GLP-1R leading to a glucose-lowering effect.97,98 In diet-induced obese (DIO) mice, Pocai et al. demonstrated that GLP-1 and GCGR dual agonism lead to superior weight loss compared to GLP-1R agonists alone while the lipid-lowering and antihyperglycemic activity of both classes were comparable. Chronic administration of GLP-1/GCGR dual agonist leads to a more pronounced improvement in plasma metabolic parameters (insulin, leptin, and adiponectin) compared to GLP-1R agonist alone. 99 Oxyntomodulin, JNJ-64565111, and MEDI-0382100,101 are examples of some agents being developed in this emerging class with some encouraging results being reported with MEDI-0382 recently. 102
GCGR antagonist
Glucagon and insulin exhibit opposite metabolic effects. Glucagon regulates glucose homeostasis through hepatic glucose production via gluconeogenesis and glycogenolysis. Glucagon receptor antagonists (GRAs) are a novel class of anti-hyperglycaemic agents designed to target hyperglycaemia in diabetes by blocking glucagon action through its receptor.103,104 GRAs differ chemically, and on this basis, can be classified into small molecule, monocloncal antibody, and anti-sense oligonucleotide agents. A variety of GRAs studied in clinical trials have shown to improve glycaemic control in terms of HbA1c, but clinically significant adverse effects have precluded their use as therapeutic options in clinical practice. Weight gain, elevated hepatic enzymes, increase in low-density-lipoprotein-C (LDL-C) levels and liver fat content, rise in systolic blood pressure, and α-cell hyperplasia are some of the concerns reported with GRA use.105,106 Efforts are underway to minimize side effects of GRAs, 107 and many agents are currently being developed from this class 101 (Table 2).
Examples of GRAs in various stages of development.

GRA, glucagon receptor antagonists.
GLP-1R/GCGR/GIPR triple agonists
Following Roux-en-Y gastric bypass (RYGBP) surgery, it was noted that the endogenous GLP-1, GIP, and glucagon (Incretins) secretion was increased. It was theorized that these incretins’ synergistic metabolic action could lead to weight reduction.112,113 HM15211, currently in phase-1 clinical trials, is a weekly SC GLP-1R/GCGR/GIPR tri-agonist peptide being developed by Hanmi Pharma to treat obesity, NAFLD, and T2DM. It is a modified human glucagon molecule formed by conjugating to human immunoglobulin G Fc fragment through PEG linkage.
To assess the efficacy in treatment of obesity, HM15211 was compared with liraglutide in DIO mice, where early results have shown a ~three-fold reduction in weight and increased energy expenditure with HM15211 compared to liraglutide. Moreover, in methionine choline–deficient (MCD) mice, HM15211 administration resulted in reduction in hepatic TGs (−82.6% vs vehicle) and thiobarbituric acid reactive substances (TBARS) (−60.7% vs vehicle). A concurrent fall in serum alanine-aminotransferase (ALT) and bilirubin was also observed. HM15211 resulted in increased intracellular cAMP through GLP-1R, GCGR and GIPR. Its robust glucagon activity caused weight loss and improved lipid profiles by accelerated lipid oxidation. GLP-1R and GIP served to neutralize the glucagon-induced hyperglycaemia.101,114,115 By affecting weight loss and improving lipid profiles, this class could provide an attractive therapeutic option for treating obesity and related diseases, for example, T2DM and NAFLD. NN9423 (NNC9204-1706) by Novo Nordisk and GGG tri-agonist by Eli Lilly are examples of some other GLP-1R/GCGR/GIPR triple agonists which are currently under development. 101
G-protein-coupled receptor ligands
A variety of mediators acting through G-protein-coupled receptors (GPCRs) can enhance and inhibit GSIS. 116 Gs, Gi, Gq, and G12 are involved in signalling pathways modulating insulin secretion. Gs and Gq stimulate insulin release while Gi inhibits it. 117
GPR119 agonists
GPR119 is a Class-A orphan GPCR found in the pancreas and the gastrointestinal tract and can regulate insulin and incretin release. Its activation leads to the intracellular accumulation of cAMP, resulting in GSIS from the pancreatic β-cells and incretin release from the gut.118,119 Due to the dual effect of GSIS and incretin release coupled with a low risk of hypoglycaemia, these agents have drawn considerable interest as a therapeutic entity in the management of T2DM. Unfortunately, no synthetic GPR119 ligand has been approved for treatment, nor has any passed beyond phase-2 clinical studies.120,121 DS-8500 is a GPR119 agonist being developed by Daiichi Sankyo Company and is currently in phase-2 clinical trials. 122
Free fatty acid receptor
Several agents have been identified to have anti-hyperglycaemic action by stimulating or blocking the free fatty acid receptor (FFAR). Among the FFARs, FFAR1 (GPR40), FFAR2 (GPR43), FFAR3 (GPR41), and FFAR4 (GPR120) have emerged as anti-diabetic targets. 123 Long-chain free fatty acids (FFAs) activate FFAR1 and FFAR4, and agonists of these two receptors have been proven to enhance insulin and incretin release. 124 Short-chain FFA activates FFAR2 and FFAR3 and as opposed to FFAR1 and 4, antagonism of these receptors has shown anti-diabetic potential. 125 Mice studies have demonstrated that FFAR2 and FFAR3 antagonists can enhance insulin secretion and glucose tolerance. 126 Agents targeting the FFAR are still in the early stages of development, and it remains to be seen whether an effective and safe drug can be delivered and inducted into clinical practice from this class in the future. P1736 and P11187 by Piramal Enterprises and LY2922470 by Eli Lilly are examples of recently studied FFAR1 agonists.123,127
Takeda G-protein-coupled receptor 5 (TGR5 agonists)
Discovered in 2002, TGR5 (also known as GPBAR1 and GPR131) is a bile acid–specific receptor found in the gastrointestinal tract, pancreas, liver, gallbladder, and adipose tissue. 128 A lot of research has gone into establishing a link between bile acids and glucose metabolism, with numerous studies showing bile acid–mediated TGR5 activation resulting in impactful gluco-metabolic sequelae including GLP-1, insulin, and glucagon release.129–132 The ability to stimulate GLP-1 secretion 133 has attracted considerable interest; however, this effect may be limited as TGR5 receptors are predominantly present in L-cells’ basolateral membrane, leading to insufficient luminal activation required to produce the desired metabolic impact.134,135 Studies in rodents suggest an important role for TGR5 in GLP-1 secretion, 129 and therefore, it is an important target for the development of pharmacotherapy directed against metabolic disease, including T2DM. 136 However, data from animal studies showed significant safety concerns with TGR5 agonists treatment, foremost of which were gall bladder dilation, pancreatitis, and hepatic necrosis. Human studies have reported no beneficial effects on GLP-1 secretion or plasma glucose levels, and as such, currently, a viable pharmacological option using this concept is not on the horizon.137,138 SB 756050, originated by GlasgowSmithKline, was TGR5 agonist studied for the treatment of T2DM. Fifty-one participants were randomized to receive either placebo or one of four doses of SB-756050 for 6 days. A single 100 mg dose of sitagliptin was co-administered on Day 6 to all participants. It was well tolerated, however, exhibited variable pharmacodynamic effects with rise in glucose at the two lowest doses and no fall in glucose at the two highest doses. The glucose effects of SB-756050 and sitagliptin were comparable to those of sitagliptin alone (ClinicalTrials.gov NCT00733577). 139 Studies on SB-756050 were eventually discontinued in Phase-2 clinical trials. 140
Melatonin receptor
Peripheral and central IR, glucose intolerance and reduced expression of the GLUT4 gene have been observed in pinealectomized animals, which improved with melatonin administration.141,142 Furthermore, a reduction in melatonin formation has been reported in animal models with T2DM.143,144 MT1 and MT2 are isoforms of melatonin receptors expressed on hepatocytes and pancreatic cells, forming part of the glucose regulation pathway. Various studies demonstrate that melatonin-mediated activation of these receptors improves insulin sensitivity and suppress gluconeogenesis.145,146 In the past, MT1 and MT2 knockout mice have been shown to have systemic IR and reduced insulin sensitivity, with the latter exhibiting increased insulin release.147–149 Ramelteon is a selective melatonin receptor (MT1 and MT2) agonist, approved by the FDA for the treatment of insomnia; 150 however, as noted by Tsunoda et al., 151 its use did not improve glycaemic control in patients with T2DM suffering from insomnia.
In contrast, piromelatine, a novel melatonin receptor agonist, has been shown to exert a protective effect on insulin sensitivity and lipid metabolism in sleep-deprived rats. 152 Melatonin receptor is a potential target for developing therapies to address hyperglycaemia. However, substantial research is required in this class to produce a clinically relevant agent in the future. Shiraz University of Medical Sciences is conducting a clinical study on Melatonin’s Effects on the Treatment of Diabetes Mellitus (METOD), which is currently in the early phase-1 stage. 153
Enzymes, hormones, and receptors as therapeutic targets
Protein tyrosine phosphatase-1B inhibitor
Protein tyrosine phosphatases (PTPs) lead to the inactivation of the insulin receptor via dephosphorylation. PTP-1B down-regulates insulin and leptin pathway and therefore has been seen as a therapeutic target for the treatment of diabetes and obesity.154,155 PTP-1B-deficient mice were observed to be sensitive to insulin and had a degree of resistance to weight gain.156,157 Selective, reversible, and high-affinity PTP-1B inhibitors have been tested in animal models, but being highly charged molecules, they could not be developed into medicinal products.158–160 KQ-791, developed by Kaneq Bioscience, has been studied in a phase-1 interventional randomized placebo control trial for treatment of T2DM (ClinicalTrials.gov NCT02445911). The study consisted of 81 participants which were divided into four groups based on the regimen of KQ-791 they receive over a period of 4 weeks. Group 1 (n = 20) received a loading dose of 100 mg on day 1, followed by single 50 mg doses on days 8, 15, 22, and 29. Group 2 (n = 20) received a loading dose of 250 mg on day 1, followed by a daily dose of 25 mg for 28 days and group 3 (n = 21) received a loading dose of 1500 mg on day 1, followed by a daily dose of 150 mg for 28 days. Group 4 (n = 20) received multiple ascending doses matching KQ-791 dose (placebo). The primary outcome measure was the difference in change in fasting blood glucose between KQ-791 and placebo from baseline to day 29. The results suggested superior improvement in fasting blood glucose in group 1 −3.28 ± 22.99 mg/dL and group 2 −3.93 ± 30.63 mg/dL compared to group 3 0.67 ± 30.82 and placebo 3.17 ± 23.17. No serious adverse event (SAE) was recorded with any intervention group. 161
Human pro-islet peptide
DM is a chronic illness and is characterized by a lack of functioning pancreatic β-cells at advanced stages. Increasing β-cell numbers to alleviate DM is the logical answer; however, this is cumbersome to deliver in clinical practice. Transplantation of donor islets has been explored but has been limited by insufficient donors. Where successful islet transplantation has been achieved, patients have been plagued with post-transplantation sequelae, including rejection and adverse effects of immunosuppressive therapies.162–166 The human pro-islet peptide (HIP) is a 14-amino acid, biologically active fragment encoded by the human REG3a gene with the ability to increase β-cell mass whereby improving glycaemic control. 167 In streptozotocin-induced diabetic mice, Jiang et al. 168 have demonstrated that HIP promotes differentiation of human foetus–derived pancreatic progenitor cells (HFPPCs) into insulin-secreting cells leading to a significant reduction in hyperglycaemia. Evidence from this landmark effort from Jiang et al. 168 suggests that ex vivo HIP-treated HFPPCs can differentiate into functional β-cells and can potentially cure diabetes in their recipients. Phase-1 clinical trials with BTI-410 (first agent in the class of HIPs) established good safety and tolerability in patients with T2DM with promising results. Boston therapeutics have now planned two 90-day phase-2 clinical trials for the study of BTI-410; one 36 patient study in immunocompromised T1DM patients post–renal transplant and another 120 patient study in otherwise healthy T2DM patients, marking the beginning of an exciting prospect. 169
Fibroblast growth factor 21 analogues
Fibroblast growth factors (FGFs) are signalling molecules responsible for wide-ranging functions from development and regeneration to maintaining metabolic homeostasis. 170 FGF-21 is an atypical member of this family, produced from the liver; it is involved in regulating glucose and lipid metabolism. 171 Elevated FGF-21 levels in obese animals have been observed to reduce hyperglycaemia, body weight, and lipid concentration. 172 Recombinant FGF-21 also demonstrates a similar effect in various diabetic animal models.173–175 Pegbelfermin (BMS-986036) is a recombinant PEGylated FGF-21 that is well tolerated and significantly reduces fat fraction in patients with non-alcoholic steatohepatitis. 176 A randomized, double-blind, placebo-controlled trial was carried out in which patients with T2DM and obesity (BMI 30–50 kg/m2) received either SC pegbelfermin (n = 96) at doses of 1, 5, or 20 mg daily or 20 mg weekly or placebo (n = 24) for a duration of 12 weeks (ClinicalTrials.gov NCT02097277). At 12 weeks, pegbelfermin therapy did not impact HbA1c concentrations compared to placebo; however, significant differences (p < 0.05) versus placebo were noted for a reduction in FPG (20 mg weekly) and an increase in whole-body insulin sensitivity (Matsuda index; 20 mg daily). In addition, significant improvements were observed in high-density lipoproteins (HDLs) and TG for the 20 mg daily regime versus placebo. Injection site bruising (5%) and reaction (4%) together with diarrhoea were among the commonly reported adverse events. 177 Based on these results, pegbelfermin warrants further investigation in evaluation of its efficacy in obesity-induced metabolic conditions.
Adenosine monophosphate analogues
Adenosine monophosphate (AMP) predominantly activates adenosine monophosphate–activated protein kinase (AMPK). Once activated, AMPK exhibits an insulin-sensitizing effect, reducing hepatic gluconeogenesis and lipogenesis via negative regulation of specific genes 178 while promoting peripheral glucose uptake and lipid oxidation in skeletal muscles. Low levels of AMPK have been noted in patients with diabetes, 179 and its activation is one of the cellular mechanisms through which metformin exerts its anti-diabetic effect.180,181 Novel agents which can activate AMPK or serve as AMP analogues have been explored as potential therapeutic modalities in T2DM. First in class, AMPK activator, O304, is a PAN-AMPK activator studied in a proof-of-concept phase-2(a), single-centre, randomized, parallel-group, double-blinded, placebo-controlled trial in patients with T2DM on metformin (TELLUS). Sixty-five patients with T2DM were studied for 28 days and O304 administration resulted in a mean absolute reduction in FPG at day 28 compared with day 1 of −0.60 mM (p = 0.010) compared to −0.10 mM in the placebo group. At day 28, O304 use resulted in a mean absolute reduction in systolic blood pressure (BP) by 5.8 mmHg (p = 0.030) and diastolic BP by −3.8 mmHg (p = 0.009). In addition to these findings, O304 use resulted in an increase in microvascular perfusion as well. These beneficial effects may allow it to play an important role in treating patient with T2DM complicated with cardiovascular disease.182,183
Glucokinase activators
Glucokinase (GK), also known as hexokinase type-IV, is part of the hexokinase enzyme family. Mainly expressed in the pancreas, liver, brain, and gastrointestinal tract, 184 it facilitates phosphorylation of glucose to glucose-6-phosphate.185,186 It regulates GSIS, hepatic glucose uptake and glycogenesis, thus regulating whole-body glucose homeostasis.187,188 Based on the characteristics mentioned above, agents activating GK have a therapeutic potential in T2DM. 189 Numerous GK activators developed thus far have shown significant glucose-lowering capabilities. However, a concomitant increase in plasma (TGs) and loss of efficacy with continued administration meant that they could not be used as therapeutic entities.190–192 TMG-123, a novel GK activator, has been shown to overcome these limitations and, in animal studies, has demonstrated glucose-lowering effects without affecting hepatic and plasma TG. As the plasma insulin levels were not increased, it is likely that TMG-123 mainly acts in the liver. 193 Although it is a viable candidate for development as a new treatment for T2DM, its safety needs to be evaluated further as Kobayashi and colleagues have shown that TMG-123 causes long-lasting hypoglycaemia and irreversibly impairs spermatogenesis in rats. 194 TTP-399 is another GK activator being investigated as a potential therapy in both T1DM and T2DM. 195
Sirtuins
Sirtuins (SIRT1-SIRT7) are a family of NAD+-dependent deacetylases which modulate a range of metabolic processes together with age-related conditions, including obesity and T2DM.196,197 SIRT1 and SIRT6 have been extensively studied and have been identified to have a role in maintaining insulin sensitivity.198,199 In the pancreatic β-cells, overexpression of SIRT1 was noted to augment insulin secretion, leading to improved glucose tolerability. 200 And by inhibiting PTP-1B (which blocks the insulin receptor), SIRT1 enhanced insulin sensitivity.156,201 Metformin is recommended as the first-line treatment for T2DM 202 and has been shown to directly activate SIRT1, 203 among various other recognized metabolic effects. This lends credence to the potential usefulness of SIRT1 activating agents in the treatment of T2DM. SIRT2, SIRT3, and SIRT6 also sustain insulin sensitivity, whereas SIRT4 and SIRT7 downregulate insulin secretion. 204 Resveratrol, a polyphenol found in grapes, has been shown to activate SIRT1. 205 It has been shown to have a positive impact on glucose homeostasis in rodents,206–208 and several studies have reported improvements in insulin sensitivity, glycaemic control, and other metabolic parameters in patients with T2DM.209–211 Jeyaraman et al. 212 reviewed RCTs comparing the effects of oral resveratrol with placebo, no treatment, other anti-diabetic medications, or diet or exercise, in adults with a diagnosis of T2DM and found that the available research was insufficient for evaluation of safety and potency of resveratrol therapy for treating T2DM. Recently, De Ligt et al. studied the effects of resveratrol 150 mg daily (n = 20) compared to placebo (n = 21), in a randomized, double-blind, placebo-controlled trial over 6 months in overweight participants with pre-diabetes (BMI 27–35 kg/m2) (ClinicalTrials.gov NCT02565979). At 6 months, although treatment with resveratrol did not affect insulin sensitivity, there was a significant (p = 0.007) difference in the post-intervention HbA1c between the two groups with the adjusted means showing a lower post-intervention HbA1c in the resveratrol group ((35.8 ± 0.43 mmol/mol) compared to placebo (37.6 ± 0.44 mmol/mol). 213 These results point towards a positive impact of resveratrol on glycaemic control; however, despite rigorous research, a clinically safe and effective SIRT activator for treating T2DM is yet to be found.214–216
11β-hydroxysteroid dehydrogenase 1 (11β-HSD1) inhibitors
11β-HSD1 is a reductive nicotinamide adenine dinucleotide phosphate (NADPH)-dependent enzyme, predominantly expressed in the liver, adipose tissue, gonads, and brain and is responsible for the formation of cortisol from its inactive metabolite, cortisone.217,218 Cortisol regulates energy homeostasis (liver and adipose tissue) and has been well characterized to impair peripheral glucose uptake and increase hepatic IR. 219 Stimson and colleagues have shown that the whole body 11β-HSD1 activity is increased in obese men with T2DM, 220 making the inhibition of 11β-HSD1 a target for treating T2DM, especially in those with high fasting blood glucose as shown by Shukla and colleagues. 221 Several compounds have entered clinical trials and have demonstrated modest improvement in glycaemic control, together with favourable changes in some metabolic syndrome parameters.222,223 11β-HSD1 inhibition will reduce the levels of circulating cortisol and, due to a lack of negative feedback, will increase levels of adrenocorticotropic hormone (ACTH). This can result in adrenal hypertrophy, accumulation of adrenal androgen precursors and depression.224,225 These unfavourable sequelae must be addressed while ensuring significant clinical benefit before a medicinal product from this class can be introduced into clinical practice. BI 135585, a selective 11β-HSD1 inhibitor, was evaluated in an open-label administration of BI 135585 200 mg as a single dose in nine healthy volunteers (ClinicalTrials.gov NCT01652742) and in a multiple-dose study with randomized, double-blind administration of BI 135585 5, 12.5, 25, 50, 100, and 200 mg or placebo once daily in 72 participants with T2DM over a period of 2 weeks (ClinicalTrials.gov NCT01282970). It was found to be safe and was well tolerated; however, adrenocorticotropic hormone was noted to be slightly raised but within the normal range. Serum cortisol levels remained unchanged and increased total urinary corticoid excretion was noted. 226 While these are positive results, its safety profile and therapeutic potency need to be investigated in further trials over a longer period of time.
Insulin
For the management of T2DM, insulin therapy is initiated generally as a last resort when patients fail to achieve their glycaemic targets with two or more oral hypoglycaemic agents (OHAs) or with non-insulin injectable medication. Various insulin preparations are now available in clinical practice, ranging from rapid to long-acting preparations. 227 As with other areas in the management of T2DM, insulin therapy has also been a focus of research, and work has been done to devise insulin preparations with alternate delivery methods. Compounds have been developed with a longer duration of action to reduce the frequency of injections.
Oral insulin
Following its endogenous release from the β-cells in the pancreas, insulin is transferred to the liver, where it undergoes degradation from the hepatic first-pass metabolism resulting in a concentration gradient between the hepatic portal and peripheral systemic circulation. 228 As parenteral insulin preparations are directly delivered to the peripheral circulation, they fail to achieve the described concentration gradient resulting in the reversal of normal physiology. Therefore, when injected, insulin reaches the liver at a lower concentration, and insulin-treated diabetic patients tend to develop weight gain and hypoglycaemia as a manifestation of peripheral hyperinsulinaemia. 229 Oral insulin, on the contrary, mimics normal physiology leading to better glycaemic regulation. Once absorbed from the gut, insulin is delivered to the liver via the portal circulation building a high portosystemic gradient. Reduced levels of systemic insulin alleviate hypoglycaemia and issues with weight gain.230–233 As a peptide hormone, insulin is susceptible to degradation from acid hydrolysis in the stomach and proteolytic cleavage in the intestine. These factors have made the production of a viable oral insulin preparation challenging.232,234 There is an emphasis on protecting and enhancing peptide drug absorption. To achieve this, researchers have employed innovative measures such as mucoadhesive polymers, micronization, absorption enhancers, protease inhibitors, and particulate carrier systems.233,235,236 A recent randomized, placebo-controlled, phase-2b trial with the novel oral human insulin, ORMD-0801, has shown promising results in subjects with poorly controlled T2DM. ORMD-0801 achieved a significant reduction in HbA1c without an increase in the frequency of hypoglycaemia or weight. 237 It can be the first commercial oral insulin preparation and has currently entered the FDA phase-3 clinical trials.
Oral devices comprising mucoadhesive patches and enterically coated capsules are another insulin delivery technique on the horizon. 238 Gupta et al. developed a mucoadhesive patch of Carbopol934, pectin, sodium carboxymethyl cellulose in 1:1:2 ratio. When loaded with bovine insulin, human insulin, and exenatide to compare the efficacies when administered through the oral route, the results indicated that mucoadhesive patches increased oral insulin absorption. They concluded that the release of the insulin from the patches was time-dependent, and the insulin loaded into the delivery system was wholly released from the patch within 5 h of administration. The results are an encouraging step towards the development of another non-invasive anti-diabetic therapeutic option in the form of sustained-release mucoadhesive patches promoting oral peptide delivery to improve patient compliance and drug adherence.239,240
Transdermal insulin
The use of the transdermal route for drug delivery has been around for a long time. In terms of insulin delivery, the transdermal route alleviates the discomfort and inconvenience of regular SC injections. This is especially true for patients on multiple daily injections (MDIs) of insulin. It bolsters compliance among patients while ensuring controlled insulin release over a while. 241 Lack of adequate permeability of the stratum corneum is the main limiting factor with this route.242,243 Over the years, researchers have been working on methods to bypass this obstacle, leading to discovering various novel techniques to achieve this.244–246 Abdul Ahad et al. 247 have summarized various transdermal insulin delivery techniques, including microneedle (MN), a chemical permeation enhancer, patches, sonophoresis, iontophoresis, nanoparticles, and microemulsions, among others. In this article, we will focus on insulin patches as a novel insulin delivery method.
Subcutaneous insulin patch-pump system
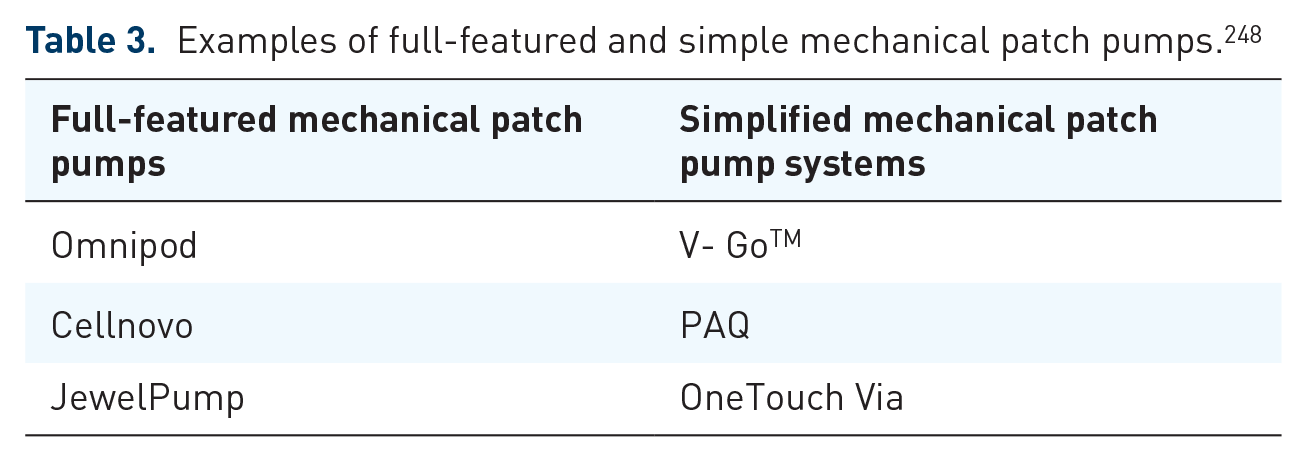
Using novel technologies, the insulin patch-pump devices provide accurate and flexible insulin delivery. Omnipod, a full-featured device available worldwide and V-GoTM, a simple specific patch pump available in the US/Europe, 248 can be seen as a sophisticated modification of the already widely used continuous SC Insulin infusion (CSII) systems (Table 3 shows examples of fully featured and simple mechanical patch pumps). Patch pumps are smaller, flexible, discreet, without tubing and cheaper, making them more attractive than CSII systems. 249 These devices do not use tubing, thus improving the user experience. The Omnipod system comprises an insulin reservoir and a handheld Personal Diabetes Manager (PDM). Using wireless technology, PDM directs the delivery of continuous basal insulin from the reservoir via a discreet needle. The V-GoTM device, on the other hand, can deliver basal and bolus insulin over 24 h and is suitable for patients on MDI insulin regimes. It replaces the insulin pens, low in price without an upfront cost and is disposable. 248 Using an adapter, the device is loaded with rapid-acting insulin analogues and then attached to the skin with a hypoallergenic adhesive strip. The basal rates are pre-set and are available as 20, 30, or 40 units of insulin per 24 h and each one also allows for 36 units of bolus insulin daily. Mader et al. evaluated PAQ®, which is a simple specific patch pump providing set basal and on demand insulin delivery. The study included 28 adults with T2DM with HbA1c ⩾53 and ⩽97 mmol/mol while treated with ⩾2 insulin injections/day. Participants were investigated in three phases: baseline (on usual insulin injections), transition, and a PAQ treatment phase. After 12 weeks of PAQ wear, HbA1c improved significantly (HbA1c –16 ± 9 mmol/mol (p < 0.0001)) while the body weight remained stable with no episodes of severe hypoglycaemia (ClinicalTrials.gov NCT02158078 & NCT02419859). 250 The patch-pump targets a large cohort within the DM population however, for patients with T2DM who are on simple insulin regimes, the simple specific patch pump is an exciting prospect as in clinical studies they have demonstrated improved glycaemic control, user satisfaction, and were cost-effective compared to MDI insulin regimes.251,252
Examples of full-featured and simple mechanical patch pumps. 248
Closed-loop pump systems
Over the last few years, particularly in the domain of blood glucose monitoring and insulin delivery, advances in technology have revolutionized diabetes care. Introduction of closed-loop (CL) pump systems are one such technological marvel, where continuous glucose monitoring (CGM) and an insulin pump function in a unified manner, achieving automation in glucose-responsive insulin delivery by the help of a computerized algorithm which adjusts basal insulin in response to data obtained from the CGM helping to maintain glucose levels in the target range. For mealtime insulin delivery, users input their carbohydrate counts into the algorithm which calculates the required insulin dose and signals the pump to deliver the dose (single hormone system). Dual hormone CL pump systems can also deliver glucagon in a glucose-responsive manner, and therefore, the CL pump systems reduce the user burden by automatically adjusting insulin delivery based on sensed glucose levels (CGM).
With the hybrid closed-loop (HCL) systems, algorithm-mediated and user-initiated insulin delivery co-exists as basal insulin delivery is adjusted automatically; however, meal time boluses are required to be programmed manually. 253 The HCL system can make regular self-directed adjustments to the basal insulin delivery rate which prevents large fluctuations in blood glucose, and overall, these novel insulin delivery systems have resulted in improved glycaemic control and reduction in hypoglycaemic events in people with T1DM.254,255 In the last 2 years numerous commercial HCL pump systems have been marketed (Table 4 describes examples of commercially available HCL pump systems and their properties while Figure 4 depicts the Medtronic 670G with the guardian 3 sensor).

The Medtronic 670G with a guardian 3 sensor; an example of a hybrid closed-loop pump system.
Interestingly, people with T1DM around the world have developed ‘Do-It-Yourself’ (DIY) artificial pancreas systems by creating their own algorithm which runs on a smartphone app and automates insulin delivery while integrating with existing CGM and insulin pumps. 256 Several studies have shown that DIY artificial pancreas systems increase the time in range (TIR) leading to a fall in HbA1c without increasing the incidence of hypoglycaemia. 259 Examples of these DIY artificial pancreas systems include OpenAPS (runs on a Linux computer); AndroidAPS (runs on an Android phone); and Loop (runs on an iPhone and communicates to the pump with the RileyLink). 259 However, these are unlicenced devices and users are responsible for any untoward events related to their use.
The HCL pump system technology is undergoing rapid development and with active trials being conducted on Insulin Only Bionic Pancreas (iLET) (ClinicalTrials.gov NCT04200313) and Omnipod Horizon™ Automated Glucose Control System (ClinicalTrials.gov NCT04196140), 256 and the future of closed-loop pump system technology appears to be bright. Although these systems are relevant to the management of T1DM which is beyond the scope of this article, we have described these systems due their novel insulin delivery method and in future we may see them being employed for treatment of people with T2DM on MDI insulin regimes.
MN patch
The MN technology provides an innovative method for transdermal delivery of proteins.260,261 The MN patch forms temporary cutaneous channels, which provide access to the epidermis and dermis for biotherapeutics delivery. Once the MN patch is removed, the micro-channels close up quickly, preventing long-term skin damage.262,263 As opposed to the 26-G hypodermic needles, MN use is tolerated much better as it causes significantly less pain, anxiety, and local tissue irritation/damage. 264 Based on the material and mechanism of drug delivery, MN’s can be classified into solid, degradable, hollow, dissolvable, and recently developed bioresponsive MNs that can respond to physiological glucose levels on-demand delivery of insulin. 265 The MN developed by Zhang et al. using cross-linked alginate coupled with maltose, were functionally robust with high cytocompatibility. These MN’s demonstrated a sustained hypoglycaemic effect in diabetic SD rats with the relative pharmacological availability (RPA) and relative bioavailability (RBA) at 94.1 ± 5.6% and 93.7 ± 4.7%, respectively, compared with that of SC injection route at similar insulin doses demonstrating their efficacy in the treatment of DM. 266 Being convenient and painless, MN is ideal for domiciliary use. However, before induction into clinical practice, a thorough investigation is required to look at their safety with regards to the potential for skin infection and irritation.
Inhaled insulin
Dance 501, from Dance Biopharm, is a front runner in the domain of pulmonary insulin delivery. It is a mist formulation of human insulin administered with a pocket-sized smart inhaler using vibrating mesh micropump technology developed by Aerogen. 267 It is small, discreet, portable, and battery-operated hence overcoming some of the major drawbacks encountered with Exubera which lead to its withdrawal from the market in 2007. 268 Data from phase-2 randomized, controlled study comparing Dance 501 to SC insulin lispro in T2DM are encouraging. Dance 501 inhaled human insulin demonstrated faster onset and greater action in the first hour of administration than SC insulin lispro, with good tolerability and without any pulmonary safety concerns. 269 The insulin release with Dance 501 is breath actuated and so requires training before use. In addition to this, before use, the inhaler reservoir needs to be loaded with insulin and may present some difficulty to patients with compromised manual dexterity, for example, in cases of tremors or severe deforming arthritis. 270 Nevertheless, if it continues to provide positive results in clinical trials, Dance 501 will be a potent option in managing T2DM.
Once weekly insulin
T2DM is a chronic illness, and to reduce the long-term morbidity burden, patients must achieve adequate glycaemic control. Due to the lack of compliance and acceptance in some patients, multiple daily basal insulin injections prove to hinder this venture. Novo Nordisk has developed a long-acting insulin analogue, insulin Icodec, which has now entered phase-3 clinical trials in the United States, United Kingdom, and Europe. By three amino acid substitutions (A14E, B16H, and B25 H) and an addition of a C20 fatty diacid containing side chain at B29 K, insulin icodec undergoes reduced enzymatic degradation and robust reversible albumin binding resulting in reduced clearance which stretches its terminal elimination half-life to 196 h. 271 These properties allow it to be used as a single weekly injection covering the basal insulin requirements for an entire week. In a randomized, double-blind, double-dummy, phase-2 clinical trial, Rosenstock et al. compared the safety and efficacy of insulin icodec with once-daily insulin glargine U100 in insulin-naïve patients with T2DM. At 26 weeks, the estimated mean change from baseline in the HbA1c was −1.33% in the insulin icodec group and −1.15% in the insulin glargine group; thus insulin icodec demonstrated similar glucose-lowering efficacy to once-daily insulin glargine U100. There were no significant safety concerns with insulin icodec either, with observed hypoglycaemia rates similar to those in the insulin glargine group. 272 From the available evidence so far, without compromising glycaemic control, insulin icodec can reduce the frequency of basal insulin injections and improve compliance, making it an exciting prospect for the future.
Genome-Wide Association Study and T2DM
Genome-Wide Association Study (GWAS) is a method used in genetics research, which can identify specific genetic variations in the form of single nucleotide polymorphisms (SNPs) linked to a variety of disease processes. 273 A recent meta-analysis of GWAS with ~16 million genetic variants in 62,892 T2DM cases and 596,424 controls of European ancestry has led to the identification of 143 variants associated with T2DM, over three dozen of which were previously unknown. 274 Impairment of pancreatic β-cell glucose sensitivity in the non-diabetic population is an independent and robust predictor of abnormal glucose tolerance and progression to T2DM.275,276 Following a genome-wide association meta-analysis, Deshmukh and Madsen et al. identified CDKAL1 and GIPR-QPCTL loci as important determinants of beta-cell glucose sensitivity. 277 Similar studies have uncovered genes that are targets for current therapeutics. KCNJ11, GLP1R, and PPARG are gene variants identified by this method for T2DM targeted by sulfonylureas (SU), GLP-1 analogues, and TZD’s, respectively.278–280 Using the knowledge obtained from GWAS, new modalities in the form of ivacaftor and lumacaftor have been developed to treat cystic fibrosis (CF).281,282 Identification of genetic variants implicated in complex pathologies, the presence of successful drug therapies against these targets and the development of new treatments using knowledge from GWAS has lent substantial credence to this approach. In the future, advances in this strategy can inform the development of effective and may be curative pharmacotherapy for T2DM.
New agents and delivery methods in pre-existing classes of medication for the treatment of T2DM
SGLT2 inhibitors, GLP-1 analogues, and dipeptidyl peptidase-4 (DPP-4) inhibitors are among the new classes of medication for the treatment of T2DM, developed over the last 15 years. Their novel MOA, ease of administration, effective glycaemic control, weight reduction capability, cardiovascular, and renal protection have had an overwhelmingly positive impact on the management of T2DM. 283 A description of these agents is beyond the scope of this review; however, we detail some of the new developments to these classes in Tables 5 and 6.
Salient features of various commercially available HCL pump systems. 256

HCL, hybrid closed-loop; RCT, randomized control trials.
Examples of new developments in pre-existing therapeutic classes in T2DM.
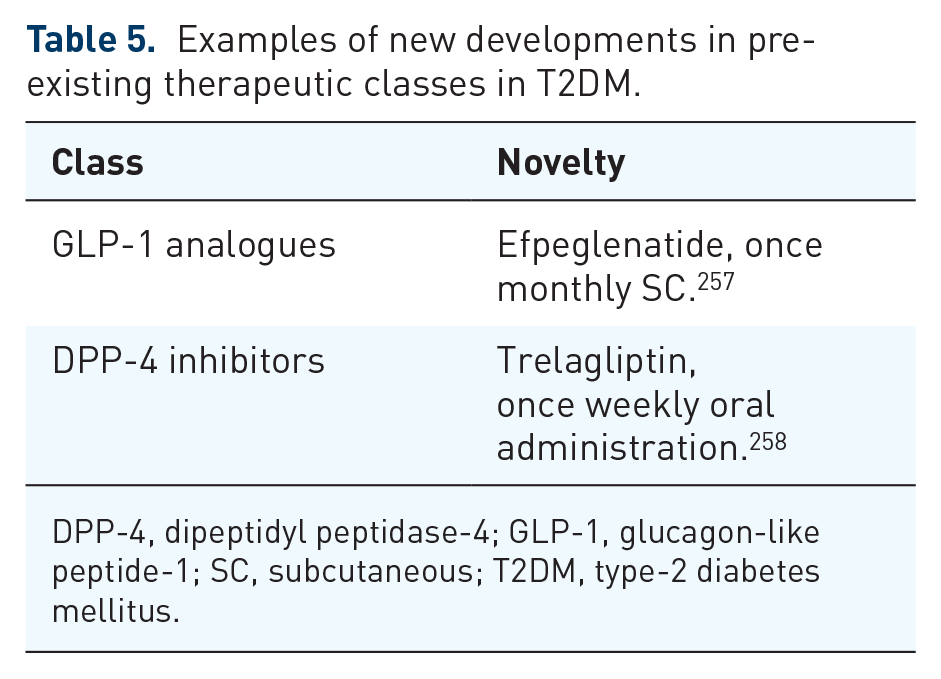
DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1; SC, subcutaneous; T2DM, type-2 diabetes mellitus.
The table summarizes some examples of new therapeutic classes, recently approved, and novel agents in pre-existing groups for the treatment of T2DM.

AMP, Adenosine monophosphate; AMPK, adenosine monophosphate-activated protein kinase; EU, European Union; FFAR, free fatty acid receptor; FGF-21, fibroblast growth factor 21; GCGR, glucagon receptor; GIP, gastric inhibitory polypeptide; GIPR, GIP receptor; GLP-1, glucagon-like peptide-1; GLP-1R, GLP-1 receptor; HIP, human pro-islet peptide; 11β-HSD1, 11β-hydroxysteroid dehydrogenase 1; PPAR, peroxisome proliferator-activated receptor; PTP-1B, protein tyrosine phosphatase -1B; SGLT, sodium-glucose co-transporter; SIRT, sirtuins; T2DM, type-2 diabetes mellitus; TGR5, Takeda G protein-coupled receptor 5.
Conclusion
Since the ground-breaking work from the French physician Jean Sterne, who studied metformin for the first time in humans in the 1950s to treat DM, 284 the industry has come a long way in investigating, developing, and delivering beneficial treatment modalities in T2DM. Most novel compounds produced for treatment have shown a potent anti-hyperglycaemic effect; however, they need to be examined further to ensure that their use is safe and well-tolerated in clinical practice. Various new therapeutic targets have been explored; however, an extension of previously known mechanisms has yielded greater success as in the case of sotagliflozin, for example. Innovations in delivery methods and reduction in dosing frequency will undoubtedly improve compliance with these formulations in the real world. Oral and once-weekly insulin, insulin patch pumps and once monthly GLP-1 analogues are an exciting prospect with the potential of conferring significant clinical benefits to patients.
The future appears to be bright; there are 129 active interventional studies in T2DM registered over the last 10 years, currently in phase 1 to phase 4 globally, based on data from ClinicalTrials.gov from March 2021. Can the academic and pharmaceutical industry come together and uncover an agent which reverses the underlying mechanisms fuelling dysglycaemia and normalizes glucose homoeostasis resulting in the cure of T2DM? Perhaps the advances in monoclonal antibody and gene therapy will provide this answer in the future.
Footnotes
Author contributions
NS: conceptualization; writing—original draft; writing—review and editing. MAA: writing—review and editing. HD: writing—review and editing. TS: supervision and writing—review and editing.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.