
Abstract
Objective:
To assess the real-world management practices of subjects with type 2 diabetes mellitus (T2DM) and type 1 diabetes mellitus (T1DM) in India.
Methods:
This cross-sectional study was conducted between 7 March 2016 and 15 May 2016 in India as part of the seventh wave (2016) of the International Diabetes Management Practices Study (IDMPS). Adult subjects with T1DM or T2DM visiting physicians during a 2-week recruitment period were included.
Results:
A total of 55 physicians included 539 subjects who met eligibility criteria. Of 495 subjects with T2DM, 303 were treated with oral glucose lowering drugs (OGLDs) only, 158 were treated with OGLD + insulin, and 27 received insulin only. Among 44 subjects with T1DM receiving insulin, 13 (29.5%) were also treated with OGLD therapy. The most commonly used insulin regimens were basal alone (69/184; 37.5%) and premixed alone (63/184; 34.2%) in subjects with T2DM, and basal + prandial insulin (24/44; 54.5%) in subjects with T1DM. Proportions of subjects achieving glycemic targets were low [glycated haemoglobin (HbA1c) <7%: T1DM = 7.3% (3/44), T2DM = 25.2% (106/495); as targeted by the treating physician: T1DM = 31.8% (14/44), T2DM = 32.1% (59/185); global target: T1DM = 4.8% (2/42) and T2DM = 1.7% (8/482)]. In subjects with T2DM, HbA1c <7% was noted in 11/22 subjects receiving insulin only and 76/260 receiving only OGLDs. Lack of experience in self-managing insulin dosing, poor diabetes education and failure to titrate insulin dosages were the main reasons for non-achievement of glycemic targets.
Conclusion:
Timely insulinization, education and empowerment of people with diabetes may help improve glycemic control in India.
Introduction
Diabetes mellitus (DM), characterised by abnormalities in insulin secretion and utilisation, is fast-attaining the status of a global pandemic. 1 In the absence of appropriate interventions, the number of people afflicted by the disease is projected to reach 629 million globally and 151 million in Southeast Asia by 2045.2,3 India has the second largest diabetic population (72.9 million) after China (114.4 million), and is expected to surpass China by 2045 (India: 134.3 million; China: 119.8 million).2–6 Many studies in India have shown a prevalence rate as high as 13% in some rural and urban areas.4,7,8
Recent data showed that glycemic control has remained suboptimal in developing nations for over a decade. 9 In India, a high potential disease burden, combined with early onset of the disease, predisposes people to diabetes-related micro- and macro-vascular complications, and these changes are significantly associated with higher rates of morbidity and mortality.4,9 These complications can often be attributed to poor glycemic control,4,10–12 and can be averted by adopting several measures, such as early insulinisation, continuing medical care and educational initiatives to improve self-management in those afflicted, as specified by published guidelines.5,13
Diabetes management can be optimised by tailoring treatment to each subject’s needs and status. 14 Owing to genetic and environmental factors, Indian subjects with diabetes share distinct clinical and biochemical characteristics (collectively known as the Asian Indian Phenotype), including greater insulin resistance, higher abdominal adiposity [i.e. higher visceral fat stores despite having a lower body mass index (BMI)], lower adiponectin concentrations, higher levels of highly sensitive C-reactive protein, significant procoagulant affinities, and a greater propensity to develop cardiovascular complications such as coronary artery disease (CAD) and atherosclerosis.4,7,8,15,16 Hence, it is imperative to develop and adopt country-specific guidelines to improve treatment outcomes and influence healthcare decision-making in Indian subjects with diabetes.2,7,8,15,16
In 2015, the Research Society for the Study of Diabetes in India (RSSDI) published clinical practice recommendations for the management of type 2 diabetes mellitus (T2DM) that were specifically designed for the Indian population while considering the diversity of socioeconomic and cultural backgrounds. 2 However, despite the widespread acceptance of the RSSDI guidelines by healthcare practitioners across India, several challenges have impeded effective diabetes care in India, including low awareness levels, reduced access to glycated haemoglobin (HbA1c) testing, and ‘clinical inertia’, resulting in delayed commencement of insulin therapy.2,4,13,17,18 In addition, due to the geographical, socioeconomic and ethnic diversity in India, there are a limited number of studies available to address these issues, 4 and there is an urgent need for studies evaluating diabetes management practices in India. Therefore, this study was conducted to assess real-world management practices of subjects with type 1 DM (T1DM) and T2DM in India.
Methods
The International Diabetes Management Practices Study (IDMPS) is an ongoing international, multicenter, non-interventional, observational study (CTRI/2018/04/013100) encompassing yearly surveys/waves (cross-sectional and/or longitudinal). The cross-sectional phase is of 2 weeks duration. The first wave of the study was performed in 2005; since then, six further waves have been assessed. The cross-sectional study (seventh wave, 2016) was carried out in 24 countries. 9
This study was conducted between 7 March 2016 and 15 May 2016 in India as part of the seventh wave (2016) of the IDMPS, in accordance with the principles of the 18th World Medical Assembly (Helsinki, 1964) and all applicable amendments, and the study was in compliance with the guidelines for Good Epidemiological Practice. All participating study sites were approved by Ethics Committee (Supplemental Table S1). Each participating site ensured that all submissions required for approval (e.g. Institutional Review Board/Independent Ethics Committee) were in compliance with local regulations, including the local data protection act. The study design and reporting format followed the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. All participating subjects provided written informed consent before starting the study.
Study design and participants
Each physician enrolled 10 consecutive adult subjects with T2DM who were consulted during the 2-week-long recruitment in the crossover period, as well as the first five visiting adults with T1DM who satisfied the eligibility criteria.
Physicians experienced in prescribing insulin therapy and managing patients with diabetes were selected randomly after stratification based on speciality. 9 The number and profile of the physicians required to participate in the study was country-specific, depending on the sample size of the subjects, as in the following.

The numbers were rounded off to the next digit. In India, 55 physicians were planned to be selected.
Inclusion/exclusion criteria
Adults (male and female) with T1DM or T2DM who consulted their physicians during the 2-week-long recruitment period were included in the study. Subjects concomitantly participating in another clinical trial, receiving temporary insulin treatment due to gestational diabetes, having had recent surgery or a diagnosis of pancreatic cancer and those who had participated in a previous wave of the IDMPS were excluded.
Baseline variables and demographic characteristics
Evaluable baseline variables were recorded by participating physicians. Since this study was non-interventional in nature, no safety data were collected, and spontaneous adverse events were reported based on guidelines specific to India. In this cross-sectional study, hypoglycemia-related information was collected by the investigator based on each subject’s cited history and the clinical notes available. The frequency and the severity of episodes of hypoglycemia in subjects with T2DM in the past 3 months were documented in the subjects’ files (source documents). The same information was transcribed in the case report form (CRF).
Statistical analysis
Sample size calculation
The sample size was determined on a country-by-country basis, using the following formula:

where ‘n’ represents the per country sample size, ‘p’ represents the estimated proportion of insulin-treated subjects with T2DM, εα = 1.96 for α = 5% and e = the absolute precision (20%) × p= the relative precision.
For India, assuming that insulin was the least prescribed therapy and that 15% of subjects receive insulin, to estimate the frequency of insulin-treated subjects with an absolute precision of 20% and a 95% confidence interval (CI), a sample size of 544 subjects was required.
Statistical methods
All recorded data were summarized using descriptive analyses. Mean, standard deviation (SD), median, and range (min–max) were used to describe continuous variables. Frequency and percentage (two-sided 95% CI) were used to describe categorical variables. Statistical analyses were performed using Statistical Analysis System (SAS) software, version 9.2 (SAS Institute, Inc., Cary, NC, USA).
Results
Physician characteristics
Of the 55 physicians who included at least one subject in the study, 52 were specialists (endocrinologists or diabetologists) and 3 were non-specialists (general practitioners, primary care practitioners and internists/cardiologists). The mean age of the physicians was 49.0 ± 8.4 years; 92.7% (51/55) were male. The specialist physicians had an average of 20.5 ± 9.6 years of clinical practice experience and usually attended 41 patients/day, while non-specialists had an average of 19.0 ± 1.0 years of experience and usually attended 20 patients/day.
All but one physician (98.2%) declared that they followed clinical practice guidelines, with the majority (49/52; 90.4%) following American Diabetes Association/European Association for the Study of Diabetes (ADA/EASD) guidelines.
Demographics and clinical characteristics
Of the 550 subjects recruited, 539 (44 with T1DM, 495 with T2DM) meeting the eligibility criteria were ultimately included. The mean age of all subjects was 53.3 ± 13.0 years. Overall, about 53.1% (286/539) of the subjects were male. The majority of subjects lived in urban areas (393/539; 72.9%) and had achieved a level of education at a secondary school level or higher (422/539; 78.3%) (Table 1).
Baseline characteristics.

Note: All variables represent n (%) other than those specified.
BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; max, maximum; min, minimum; OGLDs, oral glucose lowering drugs; SBP, systolic blood pressure; SD, standard deviation; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Medical history of diabetes
The total duration of diabetes disease progression was much longer than the duration of insulin treatment received by the subjects with T2DM who were receiving insulin alone (8.5 ± 7.7 years versus 4.1 ± 3.1 years) and in those receiving combination therapy with insulin + OGLDs (13.5 + 7.30 years versus 3.9 ± 4.4 years).
Diabetes-related complications were noted in 31.6% (156/493) of subjects with T2DM and 15.9% (7/44) of subjects with T1DM. Among the subjects with T2DM, 27.2% (134/493) had experienced microvascular complications and 6.1% (30/493) had experienced macrovascular complications.
Symptomatic episodes of hypoglycemia were noted in 45.5% (20/44) of subjects with T1DM and 13.6% (66/487) of subjects with T2DM in the preceding 3 months. Severe episodes of hypoglycemia (requiring assistance) were noted in 15.9% (7/44) of subjects with T1DM and 2.3% (11/487) of subjects with T2DM in the preceding 12 months. Hospitalisations due to diabetes-related complications were reported in 9.3% (4/43) of subjects with T1DM and 4.3% (20/462) of subjects with T2DM during the preceding 12 months (Table 2).
Diabetes medical history.

Note: All variables represent n (%) other than those specified.
OGLDs, oral glucose lowering drugs; SD, standard deviation; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Therapeutic management of diabetes in current practices
Most subjects (68.4%, 361/539) followed a healthy diet and exercise plan.
The major classes of drugs used for treatment of subjects are presented in the Supplemental Table S2. Among the 495 subjects with T2DM, 461 (93.1%) were being treated with OGLDs (alone or in combination with insulin), 303 were being treated with OGLDs only, 158 were receiving combination OGLD + insulin therapy and 27 were treated with insulin only. Among the 185 insulin-treated subjects with T2DM, basal insulin alone (69/184; 37.5%) and premixed insulin alone (63/184; 34.2%) were the most commonly used regimens. In all, 13.4% (24/179) of subjects with T2DM had discontinued insulin therapy in the past.
Among the subjects with T1DM, all 44 were on insulin and 13 (29.5%) were also receiving OGLD therapy. Basal + prandial insulin was the most commonly used regimen (24/44; 54.5%) in subjects with T1DM (Table 3).
Therapeutic management of diabetes.

Note: All variables represent n (%) other than those specified.
A subject could receive more than one type of basal/prandial/premix insulin.
A subject could use more than one device.
OGLDs, oral glucose lowering drugs; SD, standard deviation; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Glycemic control
A glycemic target of HbA1c <7%, as recommended by international guidelines, was achieved by about one-fourth (106/495; 25.2%) of subjects with T2DM, but by only 7.3% (3/44) of those with T1DM. Approximately 17.1% (7/41) of subjects with T1DM and 24.3% (102/420) of those with T2DM had tested below the HbA1c targeted value recommended by their physician.
In subjects with T2DM, an HbA1c <7% was noted in 50.0% (11/22) of subjects receiving insulin only and in 29.2% (76/260) of those receiving OGLDs only. Glycemic goals as targeted by the treating physician were reached in approximately one-third of all insulin-treated subjects (T1DM: 14/44, 31.8%; T2DM: 59/185, 32.1%).
Lack of experience in the self-management of insulin dosing (38/125; 30.4%), poor diabetes education (36/125; 28.8%), and improper titration of insulin doses (31/125; 24.8%) were the main reasons for non-achievement of glycemic targets in people with T2DM, whereas improper titration of insulin (14/30; 46.7%) was the major factor in people with T1DM. Among other factors, discontinuation of insulin use (T2DM: 20/125, 16.0%; T1DM: 3/30, 10%) was another reason for non-achievement of glycemic targets, as was the cost of testing strips in 23.3% (7/30) of subjects with T1DM and 13.6% (17/125) of subjects with T2DM.
Only 4.8% (2/42) of subjects with T1DM and 1.7% (8/482) of subjects with T2DM met the global target/triple target [HbA1c <7%, normal blood pressure (systolic blood pressure/diastolic blood pressure: 130/80 mmHg), and LDL cholesterol <100 mg/dl pooled together] recommended by international guidelines (Table 4).
Glycemic control.
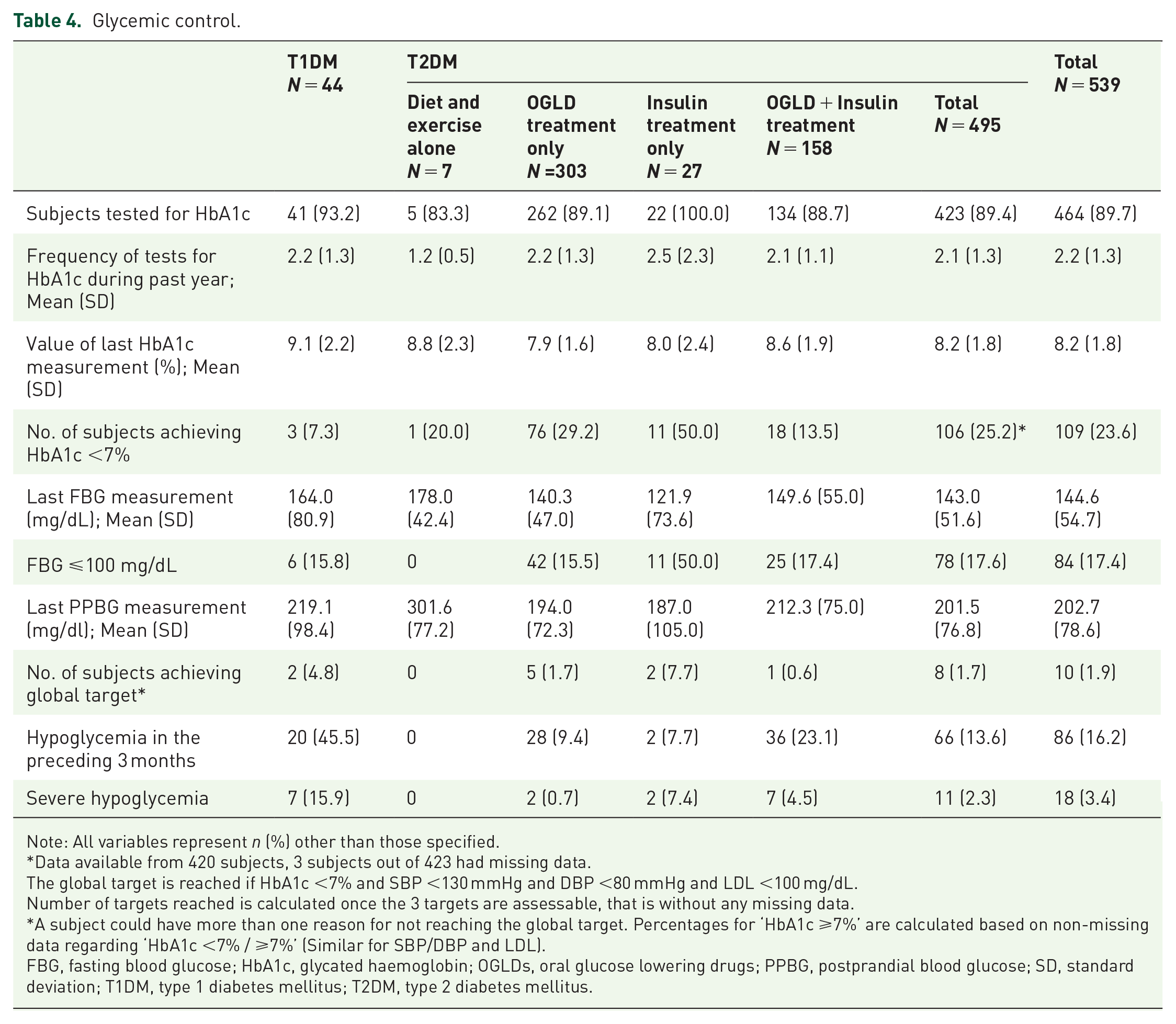
Note: All variables represent n (%) other than those specified.
Data available from 420 subjects, 3 subjects out of 423 had missing data.
The global target is reached if HbA1c <7% and SBP <130 mmHg and DBP <80 mmHg and LDL <100 mg/dL.
Number of targets reached is calculated once the 3 targets are assessable, that is without any missing data.
A subject could have more than one reason for not reaching the global target. Percentages for ‘HbA1c ⩾7%’ are calculated based on non-missing data regarding ‘HbA1c <7% / ⩾7%’ (Similar for SBP/DBP and LDL).
FBG, fasting blood glucose; HbA1c, glycated haemoglobin; OGLDs, oral glucose lowering drugs; PPBG, postprandial blood glucose; SD, standard deviation; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Diabetes self-care practices
About 45.8% (223/487) of subjects with T2DM and 75.0% (33/44) of subjects with T1DM had a glucometer, and most of those self-monitored their blood glucose concentrations. Approximately 27.8% (47/169) of subjects with T2DM and 53.8% (21/39) of subjects with T1DM were self-managing blood glucose (SMBG) and insulin levels. Of those with T2DM, 40.5% (75/185) self-adjusted insulin doses.
The cost of testing strips was a limiting factor for those regularly SMBG in more than one-third of subjects with T1DM (10/26; 38.5%) and T2DM (76/210; 36.2%) (Table 5).
Diabetes self-care practices.
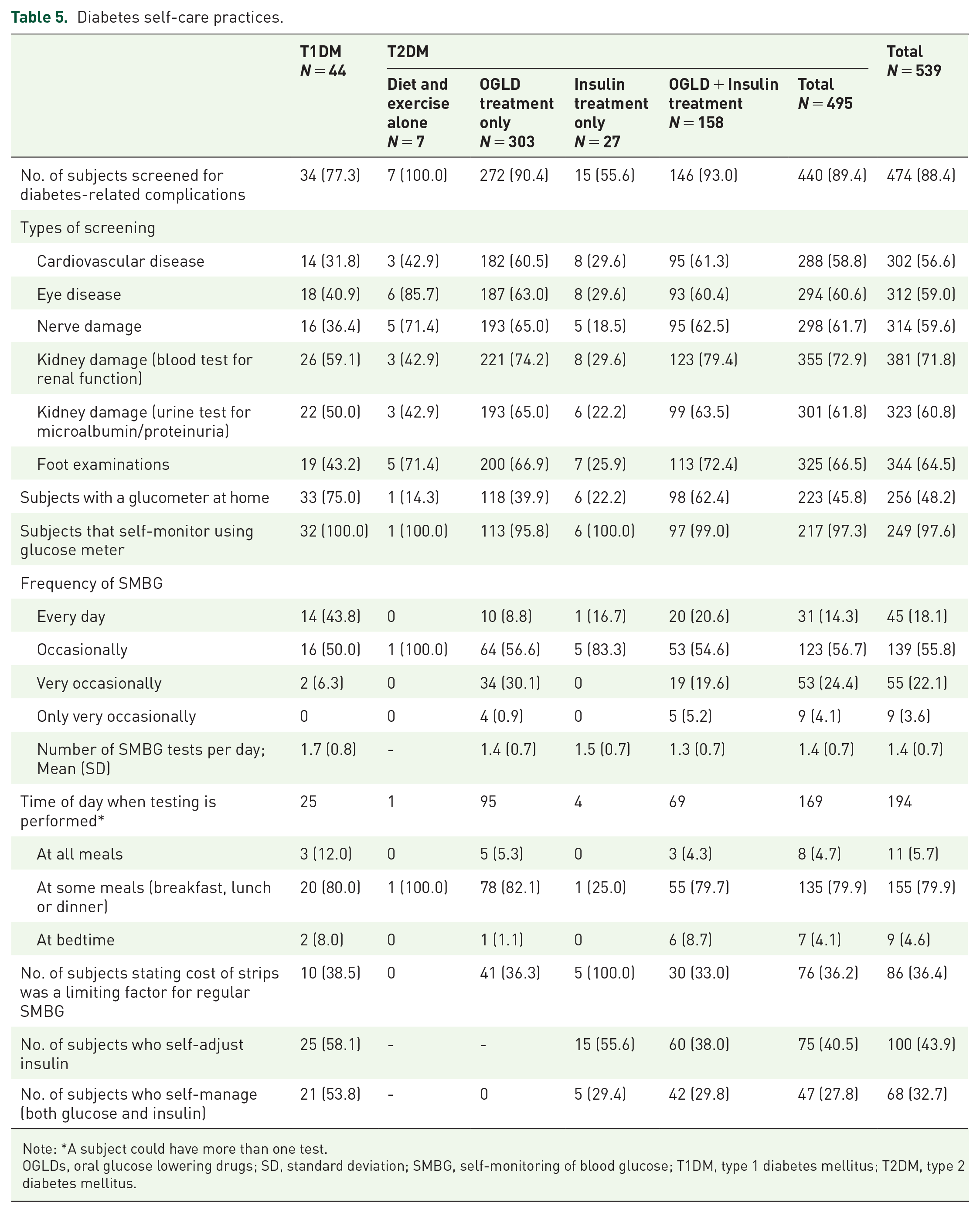
Note: *A subject could have more than one test.
OGLDs, oral glucose lowering drugs; SD, standard deviation; SMBG, self-monitoring of blood glucose; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Diabetes education
Most subjects with T1DM (39/44, 88.6%) and T2DM (459/493, 93.1%) had received diabetes education in the past, and most (T1DM: 38/44, 86.4%; T2DM: 443/491, 90.2%) were involved in an educational program provided by the physician or his/her clinical staff (Table 6).
Diabetes education and knowledge among subjects.
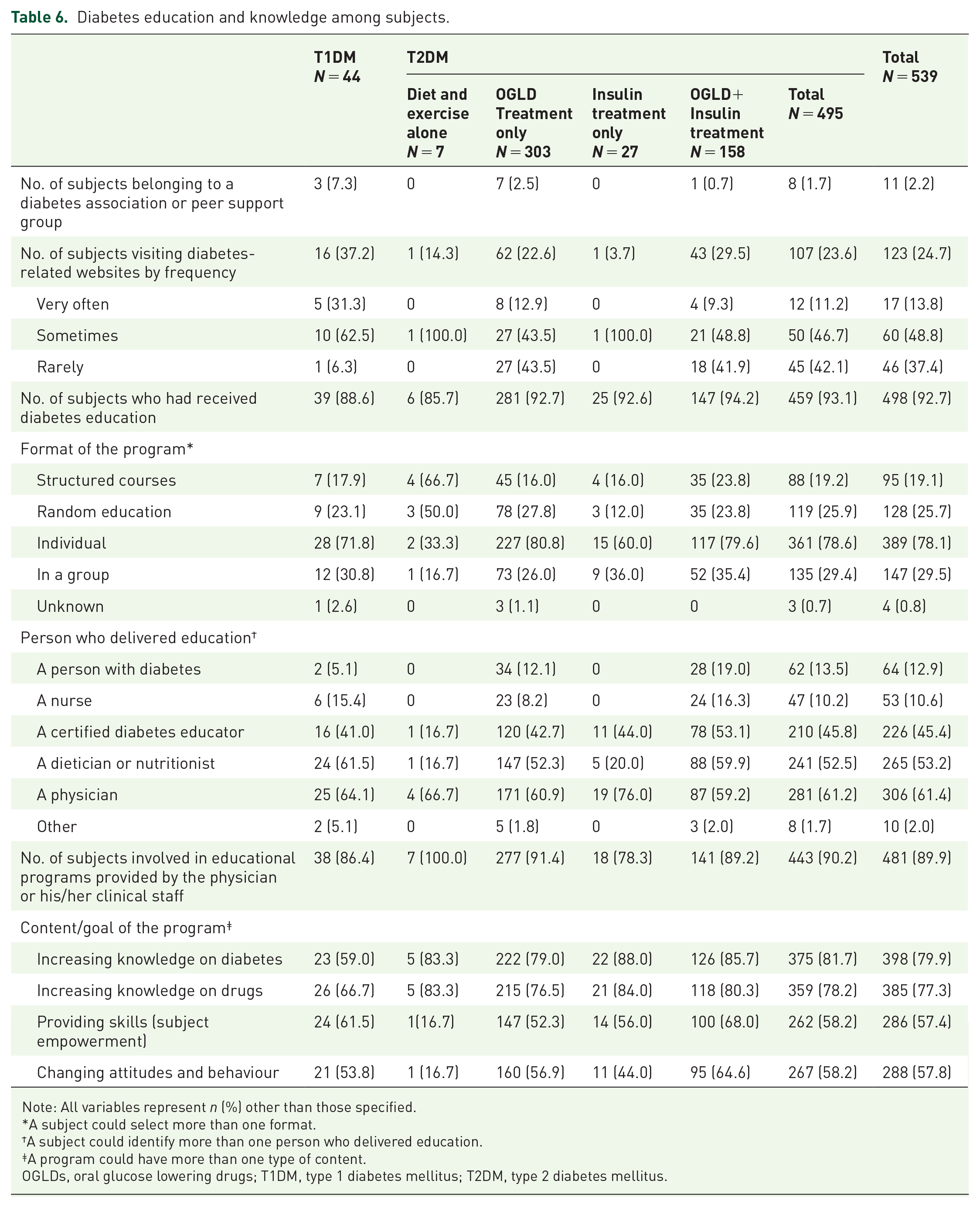
Note: All variables represent n (%) other than those specified.
A subject could select more than one format.
A subject could identify more than one person who delivered education.
A program could have more than one type of content.
OGLDs, oral glucose lowering drugs; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Discussion
This cross-sectional study conducted in India as part of the seventh wave (2016) of the IDMPS showed that, despite suboptimal glycemic control and diabetes-related complications in subjects with T2DM in India, there was a considerable delay in initiation of insulin treatment. A low proportion of subjects with T1DM and T2DM achieved glycemic targets (either in accordance with international guidelines (HbA1c <7%), targets set by the treating physician or pooled global targets), though a greater number were on target in the group receiving insulin alone. Among subjects with T2DM, a higher proportion of those treated with insulin alone had HbA1c <7% than those treated with OGLDs alone. The principal reasons for non-achievement of glycemic targets were a lack of experience in self-managing insulin dosing and poor diabetes education for subjects with T2DM, while a lack of insulin titration and inexperience in the self-management of insulin dosing were the main contributing factors overall.
In this study, a substantial proportion of subjects with T1DM and T2DM followed a healthy diet and exercise plan. Diet and lifestyle modifications are particularly necessary in Indian subjects with diabetes, as cardiovascular diseases such as CAD occur two to four times more frequently compared with the rates in those without diabetes, and they occur prematurely in Indians, typically one to two decades earlier than in the Western world. 19
In addition to diet and lifestyle modifications, the ADA/EASD guidelines recommend basal insulin as the primary therapeutic option, either as a monotherapy or as an add-on, when OGLDs fail. In line with these recommendations, basal insulin was the most commonly administered insulin regimen in subjects with T2DM in this study, while basal + prandial insulin was the most commonly used regimen in subjects with T1DM. 20 In this study, the duration of diabetes progression was longer than the duration of insulin use to treat it, indicating that, in India, initiation of insulin treatment in subjects with T2DM was delayed for many years after disease onset/diagnosis. Moreover, among subjects with T2DM receiving OGLDs alone, almost three-quarters were treated with more than two OGLDs, though more subjects receiving insulin alone achieved their glycemic targets than those receiving OGLDs alone. This suggests better glycemic control is possible when insulin treatment is initiated early, when no benefit is experienced with OGLDs. In India, physicians are often apprehensive about treating patients with diabetes due to the perceived complexities of the insulin regimen and the associated weight gain and possibility of hypoglycemic events. This results in a ‘clinical inertia’ whereby initiation of insulin therapy is delayed; thus, continuing medical education programs for general practitioners may help overcome resistance to insulin initiation. 4
Only 25.2% (n/N = 106/420) of subjects with T2DM and 7.3% (n/N = 3/41) of subjects with T1DM in this study had HbA1c <7%, indicating suboptimal levels of glycemic control in India. The overall rate of glycemic control observed in this study of participants in India was marginally lower than that observed in other developing nations, 9 and was much lower than that observed in the DiabCare Asia study, a large-scale study designed to assess diabetes control, management, and complications in subjects with diabetes from Asian countries 21 ; the latter study reported that in India, approximately half the subjects with diabetes had poor glycemic control.
In patients with diabetes, suboptimal glycemic control has serious implications and is a major risk factor for the development of micro- and macro-vascular complications. 22 Thus, it can be speculated that the high incidence of micro- and macro-vascular complications observed in this study resulted from inadequate glycemic control. Large scale studies such as the United Kingdom Prospective Diabetes Study (UKPDS) and Action to Control Cardiovascular Risk in Diabetes (ACCORD) have shown that intensive glycemic control can reduce the risk of cardiovascular events by 16% (combined fatal and non-fatal myocardial infarction and sudden death) and can slow the onset and/or progression of early stage microvascular complications. 23 This makes a strong case for aggressive clinical measures to initiate early insulin treatment, along with proper dose titration to improve diseases outcomes.
Efforts to improve diabetes management by various governments and agencies around the world, including those in the United States, Australia, the United Kingdom and the United Arab Emirates have resulted in improved disease outcomes in their respective countries.4,24–27 In India, similar efforts to improve the quality of care and clinical outcomes will require appropriate government interventions and combined efforts from all stakeholders at a ‘grass roots’ level.4,28
This study clearly indicates there are areas for improvement, as lack of experience in the self-management of insulin dosing and lack of diabetes education were the main reasons for not achieving glycemic control. The AT-LANTUS, Asian Treat to Target Lantus Study (ATLAS), and the India subset of the ATLAS studies proved that subject-driven self-titration algorithms are superior to physician-managed algorithms in achieving significantly improved glycemic control with a low incidence of severe hypoglycemia.29–31 Hence, while physicians may be approached to facilitate the implementation of screening and early detection programs, involvement of people to proactively manage diabetes with SMBG can greatly reduce disease-related morbidity and mortality.4,32 Also, as the cost of testing strips was a limiting factor in SMBG in more than one-third of subjects with T1DM and T2DM, it may help to improve access to less expensive glucometers and test strips, in addition to creating greater awareness of the benefits of regular SMBG. Further, educational campaigns to improve subjects’ self-management skills and to motivate them to make necessary lifestyle changes can go a long way in improving disease outcomes. 33
As country-specific data pertaining to diabetes management in India has been scarce, this multicenter cross-sectional study provides valuable real-world data on diabetes prevalence, routine management practices, and associated complications. This data, which is specific to India, is comparable with other international data of the IDMPS on standards of diabetes care, and it highlights gaps and areas for improvement, providing a basis for formulating healthcare policy and guiding appropriate healthcare interventions. Nonetheless, the observational design of the study had some inherent shortcomings such as bias, confounding factors, and an inability to discern cause-and-effect relationships between variables. Moreover, by nature of its cross-sectional design, the study did not permit long-term follow up to study associations between other factors. Though the study did identify suboptimal glycemic control in India, it could not objectively scrutinise the barriers preventing control or evaluate newer therapeutic endpoints such as quality of life measures that have now gained substantial weighting in diabetes management decisions.
Conclusion
This real-world study in people with diabetes who were treated in India revealed that a low proportion of subjects were able to achieve their glycemic targets. Considering the evident cost barriers in resource-constraint settings of India, improving people’s access to economically viable glucometers and test strips, providing timely insulinisation, and facilitating education and empowerment of people to self-manage glucose levels and self-adjust insulin doses, may help people to better manage their glycemic targets and improve diabetes treatment in India.
Supplemental Material
sj-pdf-1-tae-10.1177_2042018820937217 – Supplemental material for Suboptimal glycemic control among subjects with diabetes mellitus in India: a subset analysis of cross-sectional wave-7 (2016) data from the International Diabetes Management Practices Study (IDMPS)
Supplemental material, sj-pdf-1-tae-10.1177_2042018820937217 for Suboptimal glycemic control among subjects with diabetes mellitus in India: a subset analysis of cross-sectional wave-7 (2016) data from the International Diabetes Management Practices Study (IDMPS) by Ambady Ramachandran, Sunil M. Jain, Sagarika Mukherjee, Sanjeev Phatak, Shailesh Pitale, Shailendra K. Singh, Navneet Agrawal, Anirban Majumdar, Neeta Deshpande, Sandeep Jhulka, Shunmugavelu Minakshisundaram, Manoj Chawla, Sailesh Lodha, Anuj Maheshwari, Brij Mohan Makkar, Sadashiva Rao, Parag Shah, Romik Ghosh, Senthilnathan Mohanasundaram, Shalini Menon, Deepa Chodankar, Vaishali Kanade and Chirag Trivedi in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-pdf-2-tae-10.1177_2042018820937217 – Supplemental material for Suboptimal glycemic control among subjects with diabetes mellitus in India: a subset analysis of cross-sectional wave-7 (2016) data from the International Diabetes Management Practices Study (IDMPS)
Supplemental material, sj-pdf-2-tae-10.1177_2042018820937217 for Suboptimal glycemic control among subjects with diabetes mellitus in India: a subset analysis of cross-sectional wave-7 (2016) data from the International Diabetes Management Practices Study (IDMPS) by Ambady Ramachandran, Sunil M. Jain, Sagarika Mukherjee, Sanjeev Phatak, Shailesh Pitale, Shailendra K. Singh, Navneet Agrawal, Anirban Majumdar, Neeta Deshpande, Sandeep Jhulka, Shunmugavelu Minakshisundaram, Manoj Chawla, Sailesh Lodha, Anuj Maheshwari, Brij Mohan Makkar, Sadashiva Rao, Parag Shah, Romik Ghosh, Senthilnathan Mohanasundaram, Shalini Menon, Deepa Chodankar, Vaishali Kanade and Chirag Trivedi in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Acknowledgements
The authors would like to thank the study participants, their families, and caregivers who were involved in this study. Editorial support during the preparation of this manuscript was provided by Alina Gomes of AG Communications, India, which was paid for by Sanofi. Editorial support was also provided by Anahita Gouri and Rohan Mitra of Sanofi, India. The authors individually and collectively are responsible for all content and editorial decisions, and did not receive any payment from Sanofi directly or indirectly (through a third party) related to the development or presentation of this study.
Author contribution(s)
Conflict of interest statement
Shunmugavelu Minakshisundaram was a study investigator and received an honorarium during the period in which the study was conducted. Anirban Majumdar is a consultant and/or speaker for Eli Lilly, Novo Nordisk India, Sanofi India Limited, and Wockhardt India Ltd. that market different insulin preparations. MC is a member of the speaker bureau for Sanofi, Eli Lilly, Novo Nordisk, Boehringer Ingelheim, AstraZeneca, USV, IPCA, Biocon, and Cipla. SMJ has been associated with Sanofi, Novo, Eli Lilly, Novartis, Boehringer-Ingelheim, and AstraZeneca for various trials and educational initiatives. AR, Sagarika Mukherjee, Sanjeev Phatak, Shailesh Pitale, NA, ND, SJ, SL, Anuj Maheshwari, BMM, SR, PS, and SKS declared no conflict of interest. RG, Senthilnathan Mohanasundaram, Shalini Menon, DC, VK, CT are employees of Sanofi.
Data Sharing Statement
Qualified researchers may request access to person-level data and related study documents, including the clinical study report, the study protocol with any amendments, the blank case report form, statistical analysis plan, and dataset specifications. Patient level data will be anonymised and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi’s data sharing criteria, eligible studies, and process for requesting access can be found at: ![]() .
.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sanofi.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.