
Abstract
Background and aims:
Oxidative stress (OS) induces the production of fibroblast growth factor 21 (FGF21). Previous data have revealed that FGF21 protects cells from OS injury and death, making it a potential therapeutic option for many diseases with increased OS. However, the association of this growth factor with OS markers in humans with chronic kidney disease (CKD) remains unknown. This study aims to evaluate the association of serum FGF21 with serum total antioxidant capacity (TAC) and oxidized low-density lipoproteins (OxLDL) in subjects in different stages of kidney disease.
Methods:
This is a cross-sectional study that included 382 subjects with different stages of CKD, irrespective of type 2 diabetes (T2D) diagnosis. Associations of serum FGF21 with OxLDL, TAC, sex, age, body mass index (BMI), fasting plasma glucose, estimated glomerular filtration rate (eGFR), T2D, and smoking, were evaluated through bivariate and partial correlation analyses. Independent associations of these variables with serum FGF21 were evaluated using multiple linear regression analysis.
Results:
Serum FGF21 was significantly and positively correlated with age (r = 0.236), TAC (lnTAC) (r = 0.217), and negatively correlated with eGFR (r = −0.429) and male sex (r = −0.102). After controlling by age, sex, BMI, T2D, smoking, and eGFR; both TAC and OxLDL were positively correlated with FGF21 (r = 0.117 and 0.158 respectively, p < 0.05). Using multiple linear regression analysis, eGFR, male sex, T2D, OxLDL, and TAC were independently associated with serum FGF21 (STDβ = −0.475, 0.162, −0.153, 0.142 and 0.136 respectively; p < 0.05 for all) adjusted for age, BMI, smoking, and fasting plasma glucose.
Conclusion:
A positive association between serum FGF21 and OS has been found independently of renal function in humans. Results from the present study provide novel information for deeper understanding of the role of FGF21 in OS in humans with CKD and T2D; mechanistic studies to explain the association of serum FGF21 with oxidative stress in CKD are needed.
Keywords
Introduction
Fibroblast growth factor 21 (FGF21), is a peptide hormone formed by 209 amino acids in humans 1 mainly expressed by the liver, and white and brown adipose tissues.2,3 In the last few years, the study of this growth factor has been of particular interest since it has been found that its serum concentration is elevated in many metabolic diseases such as the metabolic syndrome, obesity, and non-alcoholic fatty liver disease,4–6 and FGF21 is upregulated in physiological conditions like fasting, 7 protein deprivation, 8 and exercise. 6 In rodent models of diabetes and obesity, administration of FGF21 improved fat metabolism, serum triglycerides, and glycemia, and prevented high-fat-diet-induced obesity.9,10 On the other hand, outcomes of FGF21 administration in humans have been controversial. 11 Likewise, recent data have shown that oxidative stress (OS), a common pathologic mechanism among metabolic and chronic-degenerative diseases, induces FGF21 production through the activating transcription factor 4 (ATF4).8,12 Thus, a direct association between FGF21 and OS has been suggested. 13 In fact, novel data from pre-clinical studies have proved that the administration of FGF21 protects cells of different origins from OS injury.14,15
In chronic kidney disease (CKD), the serum concentration of FGF21 is also elevated16,17 and it gradually increases as estimated glomerular filtration rate (eGFR) declines. 18 Previous data from pharmacokinetics studies in rodents have revealed that nearly 80% of FGF21 is excreted through urine, 12% from feces, and less than 7% from bile. 19 Thus, it is possible that an increase of FGF21 could be directly attributed to the reduction in glomerular filtration in healthy humans, but the pharmacokinetics of endogenous FGF21 in patients with CKD has not been fully elucidated. To date, it is known that OS is involved in the development and progression of kidney disease.20,21 Hence, knowing that FGF21 is produced in response to OS, it is possible that the elevated serum concentration of FGF21 in subjects with CKD could be partially associated to their increased serum oxidative status, independently of its excretion rate. However, to the best of our knowledge, an association between FGF21 and OS in humans with CKD has not been fully yielded.
The prevalence of CKD and its complications are a major burden of disease worldwide. 22 Therapeutic options that effectively prevent its progression, unfortunately, are limited. Thus, prevention of CKD is one of the major health challenges worldwide. 23 Determining whether FGF21 has an independent association with OS markers in CKD could support its therapeutic potential targeting OS for CKD.
OS can be assessed both by the pro-oxidant and the antioxidant perspective, and serum oxidized low-density lipoproteins (OxLDL) are used as a pro-oxidant biomarker of oxidative stress in many metabolic diseases. 24 Likewise, total antioxidant capacity (TAC) is the measure of the overall effect of the antioxidant mechanisms in the oxidative status of serum. 25 Although high antioxidant activity reflects protection or benefit over oxidative stress, it also reflects upregulation of antioxidant mechanisms in response to chronic OS. Thus, TAC assays have been used as an overall indicator of the oxidative status.26–29
Therefore, the objective of this study is to evaluate the association of serum FGF21 with the OS biomarkers serum OxLDL and TAC in subjects with different stages of CKD, with or without type 2 diabetes (T2D), according to the Kidney Disease: Improving Global Outcomes (KDIGO) classification. The hypothesis is that as eGFR deteriorates, there is an increase in OS (demonstrated through the OxLDL and TAC), and that serum concentration of FGF21 is positively associated with these markers, independently of renal function and T2D diagnosis.
Methods
Participants
The subjects studied were randomly selected from the cohorts of three different protocols: The first cohort consisted of patients who participated in the Salt and Mexico (SALMEX) Study 30 (a cross-sectional study aimed to assess the average sodium, potassium, and iodine intake in the Mexican population); from this cohort 112 subjects were selected. The second cohort consisted of subjects diagnosed with T2D who attended the outpatient endocrinology clinic at the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), from which 166 subjects were selected. The third cohort consisted of subjects from Municipio de Hidalgo, Michoacan, Mexico [a town with the highest prevalence of CKD of Michoacan, with over 1000 subjects identified (Unpublished data, López-Cervantes M)]; from this cohort 104 subjects were included. Inclusion criteria for all participants were: Adults from 18 to 80 years old, irrespective of sex, T2D diagnosis or stage of renal function. Patients were excluded if they had any hospitalization in the past 3 months and within enrollment of the study, active cancer, febrile illness 6 weeks before enrollment, HIV, Hepatitis B or C infection, pregnancy or lactation, diagnosis of other type of diabetes (such as type 1, latent autoimmune diabetes in the adult or maturity onset diabetes of the young), and diagnosis of any other chronic disease.
This protocol was approved by the Research and Ethics Committee of the INCMNSZ (Protocol reference number 635). The study was conducted according to the Declaration of Helsinki. All participants signed an informed consent before the enrollment in the study.
Clinical evaluation
A clinical history and physical examination were obtained from all participants. Blood pressure was measured after 10 min of sitting rest; weight and height were assessed with an Omron® HBF-514C scale and a wall-mounted height measuring tape A.D.E® 10017 respectively. Body mass index (BMI) was calculated as weight in kg/(height in m) 2 .
Biochemical evaluation
Blood samples were obtained after 8–12 h of fasting. Total blood was drained into a BD® Vacutainer SST tube, then was centrifuged and the serum was frozen at −80°C until analysis. Serum creatinine and fasting plasma glucose were analyzed using the automated Beckman Coulter SYNCHRON® system. The eGFR was calculated using the Chronic Kidney Disease Epidemiology (CKD-EPI) formula. 31 Hemoglobin A1c (HbA1c) was analyzed only in subjects with diabetes (due to budget and practicality of the test) through high-performance liquid chromatography using a Bio-Rad® Variant II Turbo Hemoglobin testing system.
OS was assessed both by the pro-oxidant and the antioxidant perspective; OxLDL was used as the pro-oxidant OS biomarker and TAC as the antioxidant OS biomarker. OxLDL was assessed using a solid-phase two-site enzyme immunoassay (Mercodia® Oxidized LDL ELISA) following the use directions specified by the developer and read spectrophotometrically. TAC was measured using a QuantiChrom® kit (DTAC-100, BioAssay Systems) in which Cu2+ (Copper) is reduced by antioxidants to Cu+; the resulting Cu+ specifically forms a colored complex with a dye reagent, and the color intensity at 570 nm is proportional to the serum TAC of the sample. 32 Smoking status was defined as current if the subject self-reported that have smoked any tobacco in the previous 12 months and included those who had quit a year earlier; non-smokers were defined as those who have more than 1 year without smoking or who have never smoked. 33 None of the participants were taking any antioxidant or vitamin supplement.
Finally, Human FGF21 in serum was quantified with an FGF21 Sandwich ELISA kit (Millipore® ELISA kit) following the assay procedure recommended by the developer.
Statistical analysis
Subjects were categorized according to the KDIGO classification into six stages (G1, G2, G3a, G3b, G4, and G5). 33 Descriptive statistics were used to estimate means and standard deviation for normally distributed variables, and median and interquartile range for variables with skewed distribution. Frequencies were expressed in percentages. Differences in frequencies from categorical variables were assessed using the Chi 2 test. Means and medians were compared using ANOVA or Kruskal–Wallis tests. To evaluate the correlation between serum FGF21 and age, sex, BMI, T2D diagnosis, smoking status, TAC, OxLDL, and eGFR, Pearson’s correlation coefficients were performed. Finally, a multiple linear regression analysis was made to evaluate which variables were independently associated with the increase of serum FGF21. Serum FGF21, OxLDL, and TAC were log-transformed to improve discrimination, calibration, and to minimize influence of extreme observations in correlation and multilinear regression analyzes. Statistical significance was considered with a p < 0.05. SPSS v. 24.0 statistical package (SPSS Chicago, IL, US) was used for all analyses.
Results
Demographic, clinical, and biochemical characteristics of the subjects classified by stages of kidney disease (G1 to G5) are summarized in Table 1. Mean age for all subjects was 55.0 ± 9.7 years, and those in stage G1 were significantly younger than the rest of patients. Overall, 49% of all subjects were males, and the proportion was similar among the six groups (p = 0.147). T2D was present in 43% of the total population; ~96% of patients with eGFR lower than 45 ml/min/1.73 m2 had T2D, and was higher compared with the rest of patients (p < 0.05). Duration of T2D was also higher in subjects from the final stages of kidney disease (G3b, G4, and G5), but the difference was only significant when compared with subjects from stage G1 (p < 0.05 versus G3b and G4, p < 0.001 versus G5). Regarding smoking status, 22% of all participants were current smokers, and among all groups, the proportion of smokers was higher in the G5 stage group (47.6%), and the lowest proportion was on the G4 stage group (4.2%). In addition, BMI, systolic, and diastolic blood pressure were similar among all groups. Hemoglobin concentration was significantly lower in subjects from G3B, G4, and G5 stages when compared with those from G1, G2, and G3a (p < 0.05 for all). As commented above, HbA1c was only measured in subjects with T2D diagnosis, and it was significantly lower in subjects from G5 stage when compared with the other five groups, possibly due to decreased hemoglobin concentration in these patients. Median FGF21 serum concentration for all subjects was of 406 (234–683) pg/ml, and it tended to increase as renal function declined, except in G4 stage, where it presented a non-significant decrease when compared with G3b [746 (512–1343) versus 584 (352–887) pg/ml; p < 0.05], but it increased again in G5 stage [1313 (627–1735) pg/ml] (p < 0.05). Regarding the oxidative marker TAC, a visible increasing trend was observed throughout kidney disease stages, and there was only a significant difference in its median serum concentration between G1 [421 (350–549) µM/Trolox Eq.] and G4 stages [593 (452–690) µM/Trolox Eq.] (p < 0.05). Mean serum concentration of OxLDL for all subjects was 53.2 ± 18.8 IU/L; among groups, OxLDL serum concentration was similar (p = 0.148).
Demographic, clinical, and biochemical characteristics of participants categorized according to KDIGO stages of chronic kidney disease.
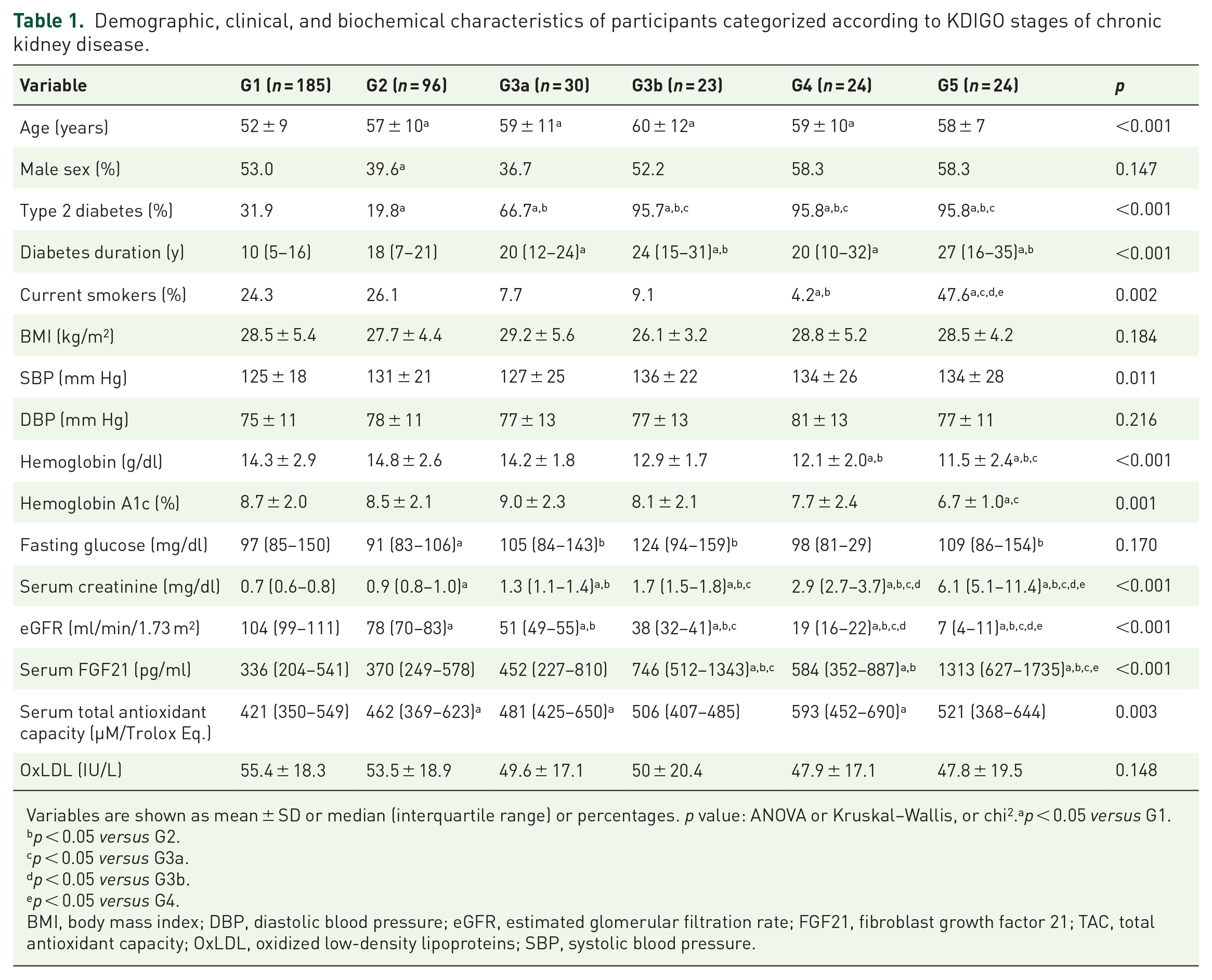
Variables are shown as mean ± SD or median (interquartile range) or percentages. p value: ANOVA or Kruskal–Wallis, or chi2.ap < 0.05 versus G1.
p < 0.05 versus G2.
p < 0.05 versus G3a.
p < 0.05 versus G3b.
p < 0.05 versus G4.
BMI, body mass index; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; FGF21, fibroblast growth factor 21; TAC, total antioxidant capacity; OxLDL, oxidized low-density lipoproteins; SBP, systolic blood pressure.
Pharmacological treatment of participants categorized according to KDIGO stages is presented in Table 2. There was a significant difference in subjects treated with metformin and insulin among groups, metformin being extensively used by patients in G1, G2, and G3 stages and poorly used in the final stages (p < 0.001). On the other hand, as the eGFR decreases, insulin treatment gradually increased (p < 0.001). Treatment with statins was present in 43.3% of the total population, and it tended to increase its use among eGFR lower than 90 ml/min/1.73 m2, but it was not significant (0.105). Angiotensin receptor blockers were significantly lower in stage G1 compared with G3b, G4, and G5.
Pharmacological treatment of the participants categorized according to KDIGO stages of chronic kidney disease.

Variables are shown as percentages. p value: chi2.
p < 0.05 versus G1.
p < 0.05 versus G2.
p < 0.05 versus G3a.
p < 0.05 versus G3b.
p < 0.05 versus G4.
ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; DPP4, dipeptidyl peptidase-4 inhibitors.
Bivariate correlation analyses are shown in Table 3. Overall, FGF21 serum concentration had a significant positive correlation with age (r = 0.236), and lnTAC (r = 0.217), and was negatively correlated with the eGFR (r = −0.429) and male sex (r = −0.102); (p < 0.05 for all). There was no significant correlation of serum FGF21 with OxLDL. The positive association of FGF21 with lnTAC remained significant (r = 0.117, p < 0.05) after controlling by age, sex, BMI, eGFR, smoking status, and T2D diagnosis (Figure 1). Additionally, after controlling by age, sex, BMI, T2D, smoking status and eGFR, a significant positive association between FGF21 and OxLDL was found (Figure 2) (r = 0.158, p < 0.05).
Correlation between FGF21, age, sex, BMI, T2D diagnosis, smoking status, TAC, OxLDL, and eGFR.

Pearson’s correlation coefficient. n = 382.
p < 0.05.
p < 0.001.
log-transformed variable.
BMI, body mass index; eGFR, estimated glomerular filtration rate; FGF21, fibroblast growth factor 21; OxLDL, oxidized low-density lipoproteins; T2D, type 2 diabetes; TAC, serum total antioxidant capacity.

Correlation between serum FGF21 and TAC, controlled by age, sex, BMI, T2D diagnosis, smoking status, and eGFR.

Correlation between serum FGF21 and OxLDL, controlled by age, sex, BMI, T2D diagnosis, smoking status, and eGFR.
Finally, a multiple linear regression was calculated to predict FGF21 serum concentration based on age, sex, BMI, T2D diagnosis, smoking status, fasting plasma glucose, TAC, OxLDL, and eGFR (Table 4). A significant regression equation was found (F = 13.154, p < 0.001, constant 6.0), with an R2 of 0.288. The eGFR, male sex, T2D diagnosis, OxLDL, and TAC were the independent variables that significantly influenced the serum concentration of FGF21 (STDβ = −0.475, 0.162, −0.153, 0.142, and 0.136 for eGFR, male sex, T2D diagnosis, OxLDL, and TAC respectively; p < 0.05 for all).
Multiple linear regression analysis using log-transformed serum FGF21 as dependent variable.

n = 382.
Constant = 6.008; F = 13.154; R2 = 0.288; p < 0.001.
Variables in bold had statistical significance in the regression model.
BMI, body mass index; FGF21, fibroblast growth factor 21; eGFR, estimated glomerular filtration rate; OxLDL, oxidized low-density lipoproteins; T2D, type 2 diabetes.
Discussion
In this cross-sectional study, a positive significant association between serum FGF21 and OS independently of renal function in humans was found. It is well known that excessive generation of reactive oxygen and nitrogen species (ROS and RNS) are contributors involved in the initiation and progression of CKD, 34 and that oxidized lipoproteins and TAC are markers of OS that are elevated in CKD and accumulate as kidney function deteriorates.27,35 Nevertheless, in this study, serum concentrations of OxLDL and TAC did not show significant increases as stages of kidney disease progressed. In an additional regression performed (Supplementary Table 1), smoking was positively associated with the serum concentration of OxLDL (STDβ = 0.144, p = 0.012). Hence, smoking status could influence in not having the expected difference of OxLDL between stages of kidney disease, since in G1 and G2 stages there were more active smokers than in the G3a, G3b, and G4 stages. Additionally, it has been reported that, in subjects with end-stage renal disease, type and form of substitutive renal therapy influences the serum oxidative status;36,37 unfortunately, given that the data of participants in this study were extracted from other previous protocols, no information was available about substitutive renal therapy of participants in the final stages of kidney disease. Therefore, it is not known whether this factor could intervene in the non-observed difference in OxLDL and TAC between CKD stages.
Although no significant increases in OxLDL and TAC were observed as eGFR decreased, serum FGF21 did have a notable tendency to increase throughout kidney disease stages. This finding, along with similar results reported previously,18,38,39 and as it has also been described that serum FGF21 is associated with an increased risk of developing nephropathy, 40 suggests that in CKD, FGF21 elevates as a compensating protection mechanism. 41
In both partial correlation and multiple linear regression analyses, serum FGF21 was positively associated with TAC and OxLDL. Actually, in the regression analysis it was found that the increase in one unit (µM/Trolox Eq.) of TAC was associated with the increase of 0.136 standardized units (pg/ml) of FGF21, and that the increase in one unit (IU/L) of OxLDL was associated with the increase of 0.142 standardized units (pg/ml) of FGF21. These associations were independent of age, sex, BMI, T2D diagnosis, smoking, fasting plasma glucose, and the eGFR. Taken together, these findings suggest that the elevated serum concentration of FGF21 in CKD is at least partially influenced by the serum oxidative status.
To date, evidence suggests that OS stimulates FGF21 production,8,12,13 and other studies have demonstrated that FGF21 protects cells from OS injury and death in cardiac cells exposed to hydrogen peroxide; 42 neuroblastoma cells (SH-SY5Y) exposed to amyloid-beta1-42; 43 mesenchymal stem cells exposed to hydrogen peroxide and tumor necrosis factor alpha (TNFa); 44 and in vivo in a rodent model of sciatic crush injury, 45 FGF21 has shown an antioxidant and protective effect.
In CKD, the approach of ameliorating OS in order to prevent or limit the progression of kidney deterioration has been explored for several years.34,46,47 Administration of some antioxidants has been associated with a significant reduction of the progression to end-stage renal disease and the improvement of the glomerular filtration rate; 48 the use of the nuclear factor erythroid 2-related factor 2 (Nrf2) activator, bardoxolone methyl, was shown to improve eGFR in patients with diabetic nephropathy;49,50 however, it increased albuminuria and blood pressure in patients with stage 4 CKD in the BEACON trial, and mortality was higher in the group receiving bardoxolone methyl,51,52 thus further study of this agent was suspended. It is discussed whether bardoxolone methyl could be more effective in subjects with earlier stages of CKD (G3) and if safety concerns might be associated with drug interactions. 53 On the other hand, in some antihypertensive and anti-hyperglycemic medications it has been shown that among the mechanisms that confer them their renal protective effects is the reduction of OS.54,55
Particularly, the use of FGF21 as a treatment for OS in CKD has been scarcely studied but it has had favorable results. For example, in rodent models of nephropathy associated to lipotoxicity and type 1 diabetes, this growth factor prevented kidney damage by suppressing 3-nitrotyrosine and 4-hydroxynonenal production in addition to reducing the inflammatory process and fibrosis; 56 indirectly, induction of the production of FGF21 through fenofibrate, and the consequent activation of the Akt-Nrf2 antioxidant pathway, prevented the death of tubular human cells exposed to high glucose concentrations and reduced OS markers. 57 Unfortunately, the therapeutic potential of FGF21 for OS in CKD in humans has not yet been studied, possibly due to its instability and short half-life. 58 Furthermore, to be able to consider FGF21 as a treatment in CKD, it is necessary to better understand the role of this growth factor in the mechanisms of the disease. The results of this study suggest that serum FGF21 is associated to OS markers in CKD; however, longitudinal studies that allow evaluation of causal associations would bring valuable information in this topic.
Although diagnosis of T2D was not correlated to FGF21 serum concentration in Spearman’s test, it was associated with increased serum concentration of FGF21 in the multiple regression analysis. Previous studies suggested that FGF21 serum concentration is elevated in subjects with T2D possibly due to increased visceral fat resistance to this growth factor 59 or the influence of BMI, total cholesterol, or triglyceride levels; 60 in our analysis, the association of FGF21 with T2D diagnosis was independent of BMI, but the lipid profile was not evaluated. Fasting plasma glucose did not show a significant association with FGF21 either in correlation or in regression analysis, possibly because there was no significant variance of glucose between groups.
In the correlation analysis, age was positively correlated with FGF21. Higher serum concentration of FGF21 in the elderly has been reported before; 61 furthermore, in healthy subjects, FGF21 has been found to increase with advancing age 62 and it has been suggested that it can improve lifespan. 63 However, in this study, the association of age with serum FGF21 was lost in the multiple linear regression, possibly due to the influence of the other independent variables studied. Sex did not show a significant correlation with FGF21, but in the multiple linear regression male sex was associated with an increase of 0.162 standardized units (pg/ml) of serum FGF21. Previous evidence had found that the concentration of FGF21 was higher in female subjects and it was associated with a higher risk of developing end-stage renal disease in women but not in men; 64 also in other study, serum concentration of FGF21 in women with T2D was associated with an increased risk of lower extremity atherosclerotic disease, but not in men. 65 It has been shown that estrogen influences liver production of FGF21; 66 however, the exact mechanisms of sex dimorphism in FGF21 regulation have not yet been fully elucidated.
The authors acknowledge the following limitations. First, the authors acknowledge that besides T2D, data regarding the etiology of CKD were not recorded. Second, it is known that TAC quantification is influenced by many biological compounds with chain-breaking antioxidant activity like urate, ascorbate, bilirubin, alfa tocopherol, carotenoids, and flavonoids; therefore, to make a more accurate interpretation of its values, the measurement of these compounds is recommended. 67 However, this assessment was not possible for us and we could only report that participants were not taking any vitamin or antioxidant supplements. Third, in some of the patients, total cholesterol, LDL-C, and HDL-C levels were not recorded, thus these variables were not included in the regression models, although lipid profile could provide more interesting information about the associations seen. Finally, due to budget limitations, TAC and OxLDL were the only biomarkers available to assess the association of OS and FGF21 serum concentration. Using other well-known biomarkers of OS in humans, such as serum lipid hydroperoxides, plasma malondialdehyde, or F2-isoprostanes, 68 to assess its association with serum FGF21 could provide valuable information regarding this research topic in future studies.
Conclusion
A positive association between FGF21 serum concentration and OS markers has been found independently of renal function in humans. Nevertheless, the present study cannot conclude that FGF21 serum values could make significant changes in OS. To the best of our knowledge, this study is the first to report this association. Since there is a great interest in the potential therapeutic use of FGF21 in relieving OS, the present study provides valuable information for the deeper understanding of the role of FGF21 in OS in humans with CKD with or without diabetes. Further mechanistic studies to explain the association of serum FGF21 with oxidative stress in CKD are needed.
Supplemental Material
sj-pdf-1-tae-10.1177_20420188211001160 – Supplemental material for Fibroblast growth factor 21 is associated with increased serum total antioxidant capacity and oxidized lipoproteins in humans with different stages of chronic kidney disease
Supplemental material, sj-pdf-1-tae-10.1177_20420188211001160 for Fibroblast growth factor 21 is associated with increased serum total antioxidant capacity and oxidized lipoproteins in humans with different stages of chronic kidney disease by Miguel Ángel Gómez-Sámano, Valerie Paola Vargas-Abonce, Froylan David Martínez-Sánchez, Lucía Palacios-Báez, Juan Mauricio Vera-Zertuche, María Fernanda Navarro-Flores, Mariana Guadalupe Morales-García, Jorge Ignacio Fonseca-Correa, Julia María Zuarth-Vázquez, Olynka Vega-Vega, Ricardo Correa-Rotter, Rodolfo Rincón-Pedrero, Luis E. Morales-Buenrostro, Josefina Alberú-Gómez, Julia Berenice Ramírez-González, Reyna Lizette Pacheco-Domínguez, Malaquías López-Cervantes, María de los Ángeles Mendoza-de-la-Garza, Yolanda Victoria Baeza-Arias, Ángeles Espinosa-Cuevas, Guadalupe López-Carrasco, Angelina López-Estrada, Luz Elizabeth Guillén-Pineda, Francisco Javier Gómez-Pérez and Daniel Cuevas-Ramos in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received funding from the department of Endocrinology and Metabolism of the Instituto Nacional de Ciencias Medicas y Nutricion Salvador Zubiran
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.